
Abstract
BACKGROUND:
Traditionally, postpartum care is confined to inpatient care immediately post birth and one appointment approximately six weeks postpartum. Data supports a continuum of care model as best for the health of mother and baby. Despite most women having significant concerns about the postpartum period, these concerns are frequently incompletely addressed by providers. We surveyed prenatal and postpartum patients to understand their concerns and experiences discussing postpartum care with providers.
METHODS:
Cross sectional surveys were administered between June 2019 and May 2021. Principal component analysis was used to show higher than average (positive) or lower than average (negative) conversations with providers about postpartum care examined by race, education, and parity. Chi squared tests were conducted to examine the significance of specific postpartum concerns.
RESULTS:
421/450 patient surveys were analyzed, based on completion. Most patients were White (193), had post graduate degrees (188), privately insured (236), married (248), first time pregnant (152), and used doctors as their primary provider (267). Patients with lower education, higher parity and Black patients without postgraduate degrees reported higher than average postpartum counseling. Additionally, most patients expressed significant concerns about postpartum exhaustion (65.8%), breastfeeding (62.3%), pain (61.2%), physical activity (54.9%) and the baby blues (50.4%).
CONCLUSIONS:
Postpartum concerns are incompletely and inconsistently addressed amongst patients based on race, parity, and education. A continuum of care approach, beginning in the third trimester, through the postpartum period, may provide better counseling to address all patients’ concerns.
Introduction
The postpartum period is defined as the first six weeks following childbirth. While generally painted as an exciting time, new mothers face significant emotional, physical, and social challenges. Notably, these include the “baby blues,” breastfeeding, pain, urinary incontinence, healthcare access, and family planning options [1, 2]. Postpartum care has lasting health impacts on the mother including preventing unwanted weight retention and the development of Type II diabetes from gestational diabetes [3]. Additionally, some argue that the infant’s health is dependent on the mothers, yet another important aspect of postpartum care [4, 5]. Despite the traditional definition of postpartum, a study evaluating the adaptation in the postpartum period suggests that this transition period is a process that lasts at least four to six months [6]. Many professionals are calling for there to be a “fourth trimester,” with a focus on addressing maternal health at 12 weeks, rather than six weeks, following birth [7–10].
The standard of care in the United States has been for women to receive one postpartum visit around the six-week mark after delivery. Studies have shown this inadequately addresses the concerns of women, as issues arise before and after this period. A 2007 study using qualitative data collected from the 2000 Pregnancy Risk Assessment and Monitoring Systems, found that 32% of respondents felt they had inadequate social support, 23.5% wished they had more breastfeeding education, and 21% felt they had inadequate newborn education at discharge [11]. Other concerns included inadequate help with postpartum depression (9.5%), perceived need for longer hospital stays (8%), and further maternal health insurance coverage outside of delivery (6%). In 2013, the World Health Organization (WHO) suggested that there be a home visit within the first week post-partum to accommodate individual constraints [2]. The WHO also recommended multiple visits postpartum to evaluate a woman’s emotional and physical wellbeing (WHO 2013) [2]. In 2018, the American College of Obstetricians and Gynecologists (ACOG) revised their recommendations, calling to shift postpartum care away from a single check-in appointment into a continuous care plan tailored to an individual’s needs, with anticipatory guidance given during the antenatal period [1].
Despite these recommendations, the postpartum visit is underutilized, with about 40% of new mothers not attending a postpartum visit [1]. Explanations for this include limited knowledge of the postpartum visit’s purpose, unavailability of providers, poor insurance coverage, and challenges of finding time, transportation, and childcare [1, 12]. Low turnout means that many women are not receiving the care and information they need during this crucial time, which can lead to unintended pregnancies and complications that increase maternal mortality [12, 14]. Maternal mortality, defined as deaths occurring during pregnancy and up to one year postpartum, is highest in the US amongst other economically comparable nations. Most of these deaths occur in the postpartum period and disproportionately affect women of color and those with lower education [15, 16].
Insurance limitations make following ACOG guidelines and supporting recommendations around postpartum continuous care more difficult. Especially among Medicaid recipients, postpartum visit turn-out is an abysmal 40% [17]. Horwitz highlights the bundled-payment model as being particularly damaging to equitable access to care [10]. Under this model, providers earn a fixed payment for all services given from the first prenatal visit up to six weeks postpartum. This payment plan is effective in reducing waste, but it fails to incentivize providers to individualize care during the postpartum period [10] Additionally, the Healthcare Effectiveness Data and Information Set, which is used by providers for reimbursement purposes, specifies only one checkup between three to eight weeks postpartum [10]. Furthermore, women may experience gaps in insurance coverage. An analysis of medical claims data found that many of the women with Medicaid were eligible because of the pregnancy and only 30% had coverage after six months postpartum [18]. The Medicaid expansion portion of the Affordable Care Act was found to have a positive effect on postpartum visit attendance and increased usage of outpatient care, but these provisions were not adopted by every state [17].
Postpartum care is also complicated by the fragmented nature of care provided and a disconnect between provider and patient concerns. In the prenatal period, mother and child are treated as a single unit, but once the baby is born, care becomes separated. Several studies demonstrate this disconnect [5, 13]. A limited study that interviewed postpartum women found that patients were generally aware of the importance of the postpartum visit as well as what to expect, but there was confusion around who was responsible for certain concerns [18]. This seems to be a common thread with interrelated health issues that impact both mother and infant. For example, topics including breastfeeding, postpartum depression, and family planning overlap in pediatric and obstetric visits. Mothers find it confusing to determine who is the proper provider to convey these concerns to and tiresome to repeat stories to multiple providers [5].
Many studies have investigated the challenges of postpartum care and adequately highlight low postpartum visits as a significant barrier to improving maternal and infant health. Evidence is mixed, however, one randomized controlled study evaluating postpartum visit attendance at different intervals found there to be an improvement in attendance with shorter intervals, but no change to health outcomes when comparing two to three week follow up with six week follow up [19, 20]. This suggests that attendance is just one component to improving maternal and infant healthcare. Few studies examine the components of the postpartum visit to determine if education and communication have impacts on postpartum health outcomes. This study examines third trimester and postpartum visits to assess provider’s communication, and patient concerns about the challenges of the postpartum period.
Materials/methods
Patients and procedures
Participants included 450 prenatal women attending appointments at the George Washington Medical Faculty Associates (GW MFA) offices in Washington, DC. Patients were approached by a recruiter and asked if they qualified for the third trimester or postpartum survey. Data was collected between June 2019 and May 2021. Participants were at least 18, in their third trimester, and competent in English to fully answer the survey questions. The study was approved by the George Washington University Committee on Human Research, Institutional Review Board (NCR191393). All surveys were answered voluntarily, and patient information was not-identifiable.
Surveys
The survey consisted of multiple choice, Likert scale and short answer responses and consisted of 17 questions that asked about the patient’s concerns and current knowledge of the postpartum period. Demographic information including insurance status, race, education, and type of provider (e.g., obstetrician versus midwife) was collected.
Data Analysis
Only 421/450 prenatal surveys were analyzed due the 29 excluded surveys being incomplete. Patients were grouped by race as either White, Black or “all others,” which included American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander or other. Data was grouped as “Other” since there was insufficient data from each of these specific descents, individually. All data were analyzed using χ2 tests to compare categorical variables by race, education, and parity. Five survey questions (Table 1) were combined into a Counsel score using principal component analysis with positive scores equating more than the average and negative scores equating less than the average counseling. Counsel scores were compared by race, education and parity using ANCOVA and multivariate statistics with maternal birth year and gestational age as covariates.
Survey question response rates
Survey question response rates
A total of 421/ 450 patient surveys were analyzed (Table 2). The average age of White patients was 37 years, for Black patients 31 years and all other patients, 35 years old (P < 0.001). Significant differences amongst these three populations also existed for educational attainment, insurance coverage, marital status, parity, and choice of medical care provider. Question 11 of the survey asked “has your medical provider discussed a plan for your medical care after you give birth. Question 12 asked if a doctor, nurse, or midwife discussed a) The challenges you may face after giving birth b) the importance of a health assessment after you give birth c) how soon after you give birth should you have a health assessment, and d) who you should see if you have health concerns after giving birth. Using a principal component analysis of question 11 and 12, a counseling score was created and examined for differences among the women based on educational degree, parity, and race. A positive score meant women were counseled more than the average about postpartum care, and a negative score reflecting less than average counseling. Overall, women with college degrees or higher were less likely to report their health care provider discussing postpartum health care (P < 0.001; Fig. 1).
Maternal characteristic and exposure by race
Maternal characteristic and exposure by race
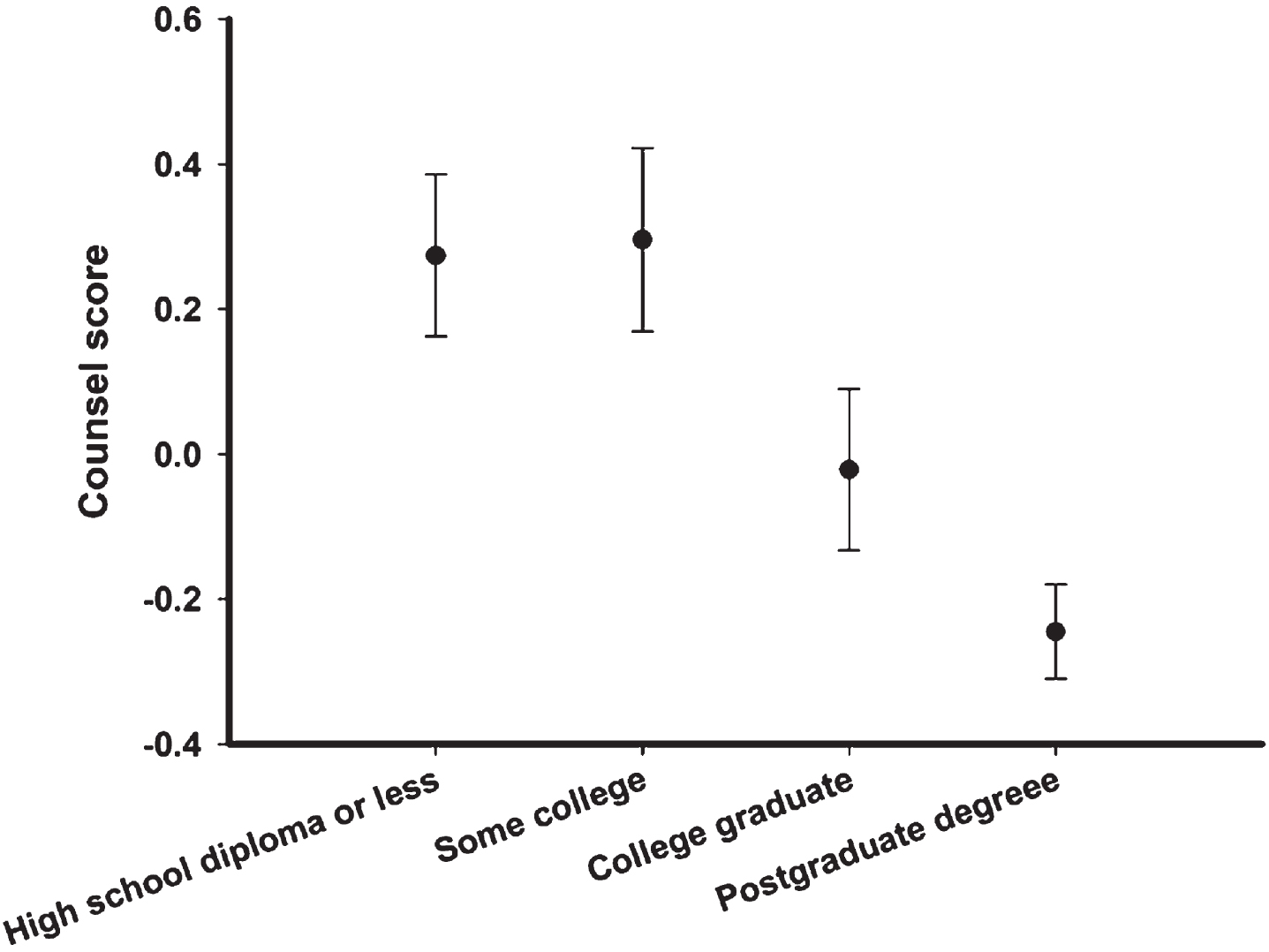
Discussion with providers about postpartum care per degree level. (High School Diploma or less = 0.274±0.112; Some College = 0.256±0.127; College Graduate = –0.0216±0.111; Postgraduate Degree = –0.245±0.065. P < 0.05).
Women with lower parity were also less likely to report their health care provider discussing postpartum health care plans (P < 0.001; Fig. 2). Overall, Black patients reported the highest percentage of conversations with providers about postpartum care, followed by Other patients and then White patients (P < 0.001; Fig. 3). However, when these three factors were examined together with gestational age as a covariate, only parity (P < 0.001) and education (P < 0.001) remained significant (race and gestational age, P > 0.2). There were significant interactions between education and race (P = 0.008) and parity and race (P = 0.045). A large proportion of White patients had postgraduate degrees and were having their first baby (Table 2). Restricting the analysis to women without postgraduate degrees, Black women had higher counsel scores than did White women (0.337 versus –0.268, P < 0.001). Looking only at White patients, education but not parity was a significant factor for counsel score, with less education associated with higher score. Examining women with postgraduate degrees all had low counsel scores regardless of race or parity.
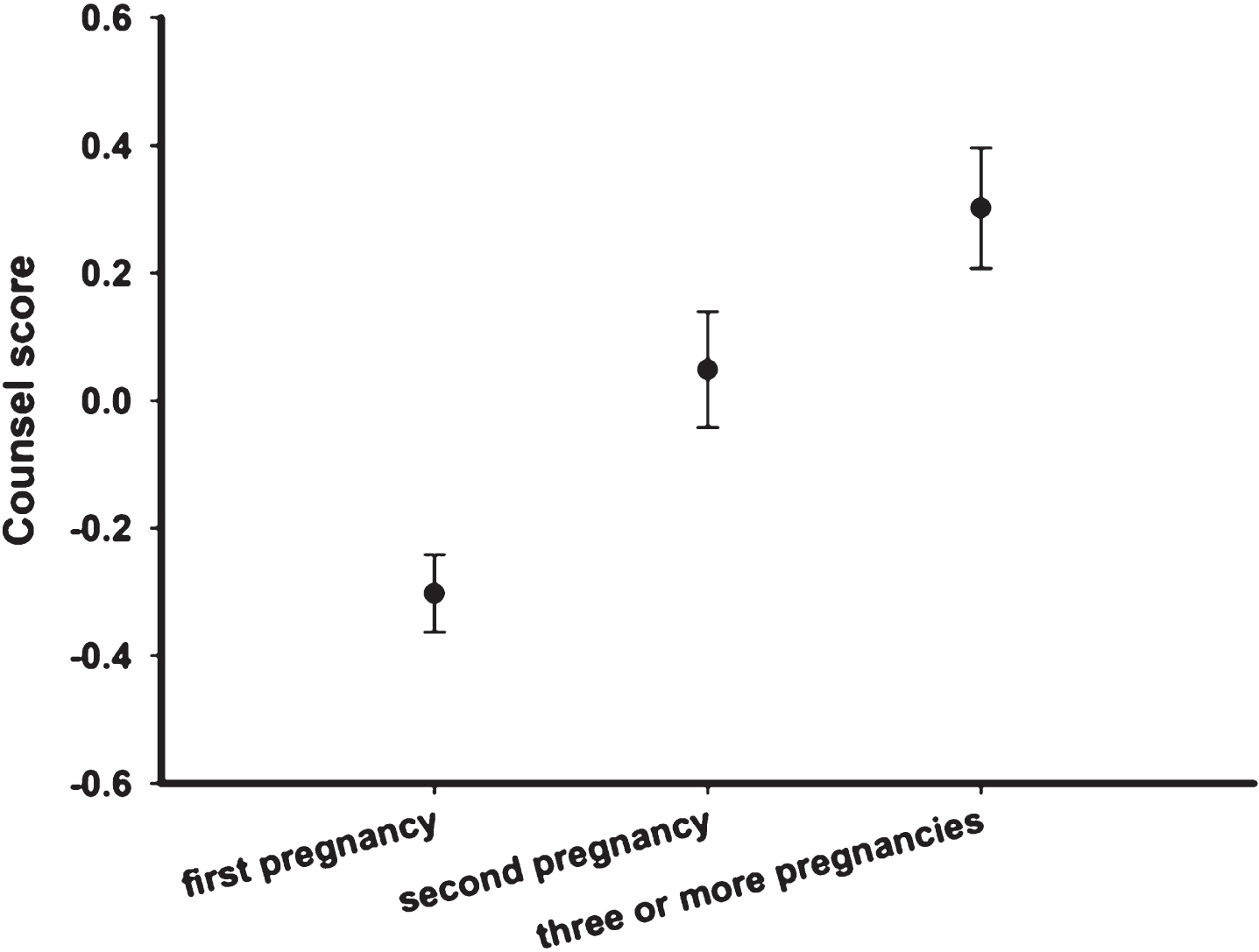
Discussion wit providers about postpartum care per parity. (First Pregnancy = –0.303±0.061; Second Pregnancy = 0.049±0.091; Three or More Pregnancies = 0.302±0.095. P < 0.05).
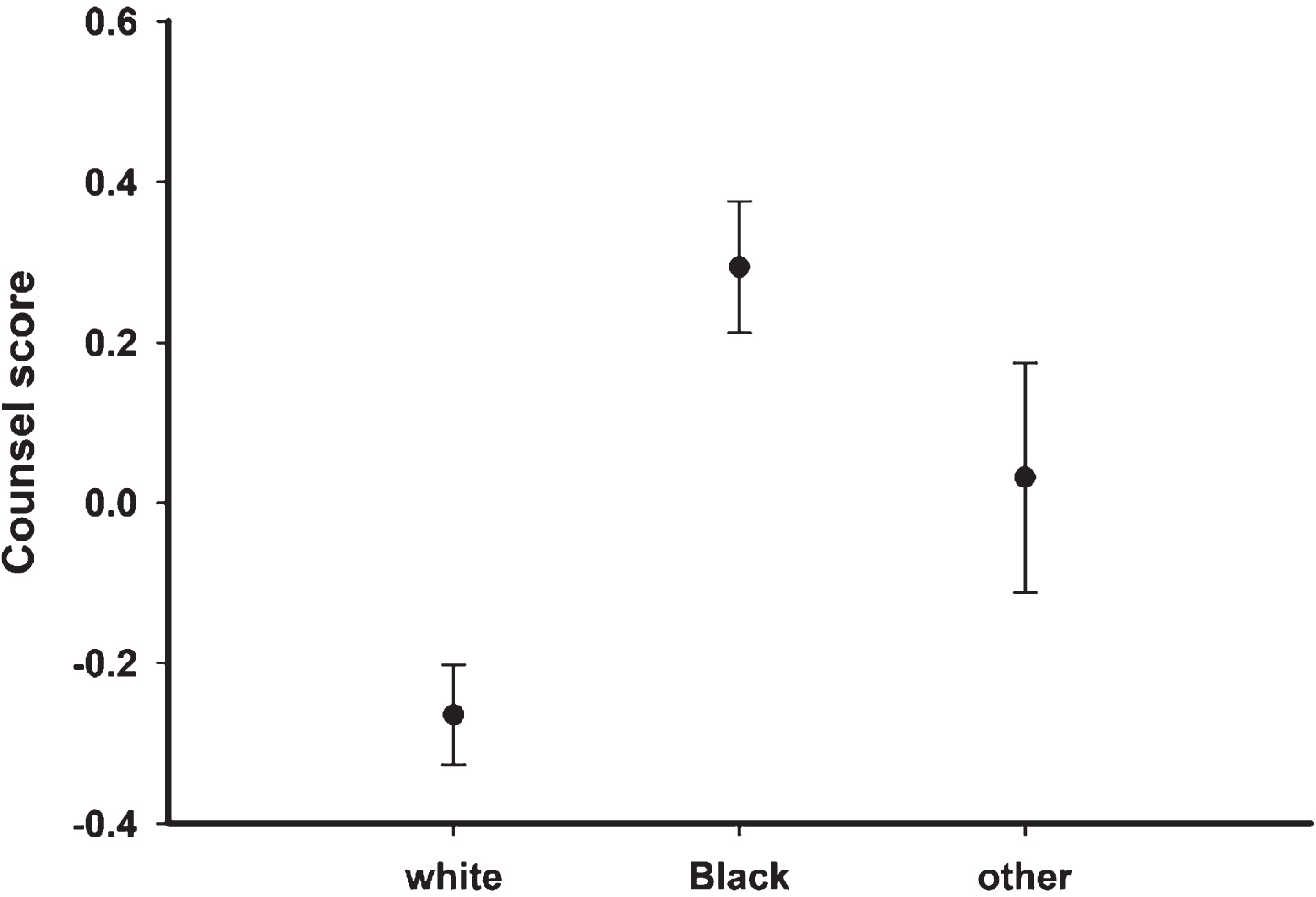
Discussion with providers about postpartum care per race. (White = –0.265±0.062; Black = 0.294±0.082; Other = 0.032±0.082, P < 0.05).
Question 13 of the survey asked patients if “when you think about what might happen in the first few weeks AFTER you give birth, do you worry about any of the following?” Except for blood pressure control, a significant percentage of women, both White and Black, reported concern for 11/12 categories of their postpartum health (Table 3). White patients were more likely to express concern except for diet postpartum, contraception, and developing diabetes, where as Black patients were more likely to express concern (Table 3).
Percent of women with the following postpartum concerns by race and overall
Overall, we found that Black patients, and patients with lower education and higher parity reported higher levels of discussion with providers about the postpartum period. Seemingly, this data shows a positive trend that providers are attempting to compensate for the historically poor postpartum care for Black and low-income patients by emphasizing to these patient populations the importance of attending postpartum visits as well as beginning these discussions when the patient is adherent to prenatal visits. This data is particularly interesting since numerous studies have shown distinct and unfortunate racial and ethnic disparities in postpartum care that were exacerbated during the COVID-19 pandemic, but there is little data studying if these disparities could decrease if postpartum discussions were initiated in the third trimester or if providers had multiple follow ups with patients postpartum [10, 21–23]. However, the multivariate result indicates that education and parity may be driving these results, not race. Because there is such a large difference in educational attainment between the White and Black patients in this study (Table 2) it is difficult to disentangle the results. The fact that women with postgraduate degrees report low levels of counseling regardless of race and that in women without postgraduate degrees Black women do report more counseling suggests that providers are using multiple criteria to guide their counseling efforts.
The parity results are interesting. It is not clear why providers would counsel women who have previously experienced childbirth more extensively about postpartum care compared to their counseling of first-time mothers. We suggest three possibilities. One, providers have limited time to counsel their patients. Perhaps providers focus their counseling more on issues that are important during pregnancy for first-time mothers. Another possibility is that counseling on postpartum care may be driven by the patients, with women who have experienced childbirth and the postpartum period more concerned about it and thus more likely to raise the issues with their provider. Finally, higher parity and recalling discussions with providers about postpartum care is likely influenced by memories of previous births and the postpartum period, increasing the likelihood that questions have, or appear to have, been addressed.
Currently, evidence for third trimester appointments focuses on infection prevention, offering membrane sweeps, and dates for labor induction [24, 25]. This may reflect that the third trimester visits are more focused on maternal-fetal health leading into delivery, and the expectation that the postpartum hospitalist obstetrician and pediatrician will discuss topics including postpartum care with the patient. Unfortunately, postpartum exhaustion makes it a poor time to discuss serious aftercare and the next time a woman sees her provider is six weeks later.
Regardless, these data show that women still experience significant concerns about the postpartum period, with most women surveyed worried about exhaustion, breast feeding, pain, exercise and activity, and the baby blues. While some anxiety surrounding these topics is natural, providers can still improve their care by discussing and addressing many of these concerns with their patients.
Limitations to this study are that surveys were based on convenience sampling and based on patient self-identification for demographics. Additionally, this study does not have a comparison, standardized population, and may only reflect demographics for its region and not be generalizable to other patients, as evidenced by the high proportion of White women with postgraduate degrees in this population. Given that the results indicate White women with postgraduate degrees reported less counseling, this may reflect this population’s individual research and education. Therefore, these patients initiated less questions requiring postpartum counseling than their Black or lower-educated counterparts. Based on the historical inequality with counseling, it is expected that in other parts of the country, White women with postgraduate degrees would report higher levels of counseling compared to their peers, and the results from this paper may not be generalizable. However, this study was conducted during business hours and patients were randomly sampled, increasing the likelihood this data could be generalized to a similar population. Finally, the survey questions asked women to report the counseling they received but did not ask about what they asked their providers. We suggest that future research should include investigating the extent to which counseling on postpartum care is influenced by patients’ questions to their provider.
Conclusion
This study shows that education and counseling about the postpartum period is influenced by education and parity, and possibly by race. Additionally, the data supports that pregnant patients still feel significant concerns about several postpartum health topics. All women should receive consistent counseling about postpartum healthcare, especially since close follow-up has a positive impact on both the mother’s and infant’s health. This supports the increasing focus for postpartum care to be viewed as a continuum, rather than confined to one appointment, to address the many needs that arise as the mother heals and adjusts to life with a newborn. This suggests that there is space for some postpartum counseling to begin in the third trimester, to help prepare the patient for upcoming challenges. Specific recommendations include developing specific, standardized, postpartum topics that should be addressed by a conversation initiated by a provider at a set third trimester appointment. Additionally, policymakers should focus on increasing postpartum care coverage such as an optional two-week postpartum appointment or at home or remote nursing visit as a check-in for mother and baby. Further research should focus on delineating specific time frames within the third trimester and postpartum to better define what is the most effective continuum of care for postpartum counseling. This will help standardize education as well as provide support for insurance coverage of these appointments.
Abbreviations
The American College of Obstetricians and Gynecologists
Centers for Disease Control and Prevention
Confidence Interval
George Washington Medical Faculty Associates
World Health Organization
Consent for publication
Not applicable.
Availability of data and materials
The datasets used for this study are available from the corresponding author on reasonable request.
Funding
This work is supported in part by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) [under cooperative agreements UA6MC31609 and U4DMC39438: Pregnancy-Related Care Research Network]. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
Conflict of interest
The authors declare no competing interests.
Author’s contributions
All authors were involved in designing the study. AP, JW, NG and ACB collected and entered data. MLP analyzed and interpreted the data. JW drafted the initial introduction and AP revised the introductions and drafted the abstract, methods, results, and conclusions. All authors revised the manuscript and contributed to the final submission. All authors read and approve of the submitted paper.
Footnotes
Acknowledgments
JS and MLP are supported by a cooperative agreement from the Health Resources and Services Administration (UA6MC31609) which supports the Pregnancy-Related Care Research Network.