
Abstract
Introduction
The restoration of independent walking is one of the major goals of post-stroke rehabilitation (Dobkin, 2005). Several studies have investigated the effects of automated electromechanical and robotic-assisted gait training devices for post-stroke improvement in walking (Geroin et al., 2013; Mehrholz, Elsner, Werner, Kugler, & Pohl, 2013). An exoskeleton, the Robot Suit Hybrid Assistive Limb® (HAL®) has been developed to assist voluntary control of knee and hip joint motion by detecting very weak bioelectric signals on the surface of the skin (Lee & Sankai, 2005). The single-leg version of the HAL® is a new wearable robot for patients with hemiplegia that has the cybernic voluntary control mode and the cybernic autonomous control mode (Kawamoto, & Sankai, 2002; Kawamoto, Hayashi, Sakurai, Eguchi, & Sankai, 2009). The cybernic voluntary control mode provides physical support and actuation according to the operator’s voluntary intentions (Suzuki, Mito, Kawamoto, Hasegawa, & Sankai, 2007). The cybernic autonomous control mode can autonomously provide effective physical support based on fundamental motion patterns (Kawamoto, Hayashi, Sakurai, Eguchi, & Sankai, 2009). Wall, Borg, & Palmcrantz (2015) reported that gait training using HAL® may have beneficial effects on post-stroke gait function and independent walking. However, well-designed and controlled studies are needed. Because many previous studies did not include control subjects, the benefits of gait training using HAL® in stroke patients require clarification. Therefore, randomized controlled trials are needed to compare the efficacy of HAL®-assisted gait training with conventional gait training (CGT) in terms of the improvement of walking ability in stroke patients.
Our previous study was the first randomized, controlled pilot trial to show the efficacy of gait training using HAL® compared to CGT (Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014). However, the long-term and medium-term efficacies of gait training using HAL® in stroke patients remain unclear. Therefore, in this study, we added 2-month follow-up data to compare the medium-term efficacy of gait training using a single-leg version of the HAL® on the paretic side with CGT in recovery-phase stroke patients.
Methods
Participants
Post-stroke patients who were admitted to a recovery-phase rehabilitation ward in Tsukuba Memorial Hospital between February 2013 and December 2013 participated in this study. All patients who participated in the previous study (Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014) were included with the addition of two new patients. The final follow-up was conducted in January 2014. The inclusion criteria, exclusion criteria, recruitment and randomization were the same as in our previous study (Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014).
In this study the experimental HAL® group was 8 male and 4 female patients (12 total) with a median age of 66.9 ± 16.0 years. 7 of this group had ischemic stroke and 7 had right side paresis. The average time since stroke was 57.0 ± 44.3 days in this group. The control group was 8 male and 4 female patients (12 total) with a median age of 76.8 ± 13.8 years. The average time since stroke in the control group was 48.1 ± 33.3 days. No differences were observed between the groups in either characteristics or baseline clinical data. Patient flow is shown in Fig. 1.
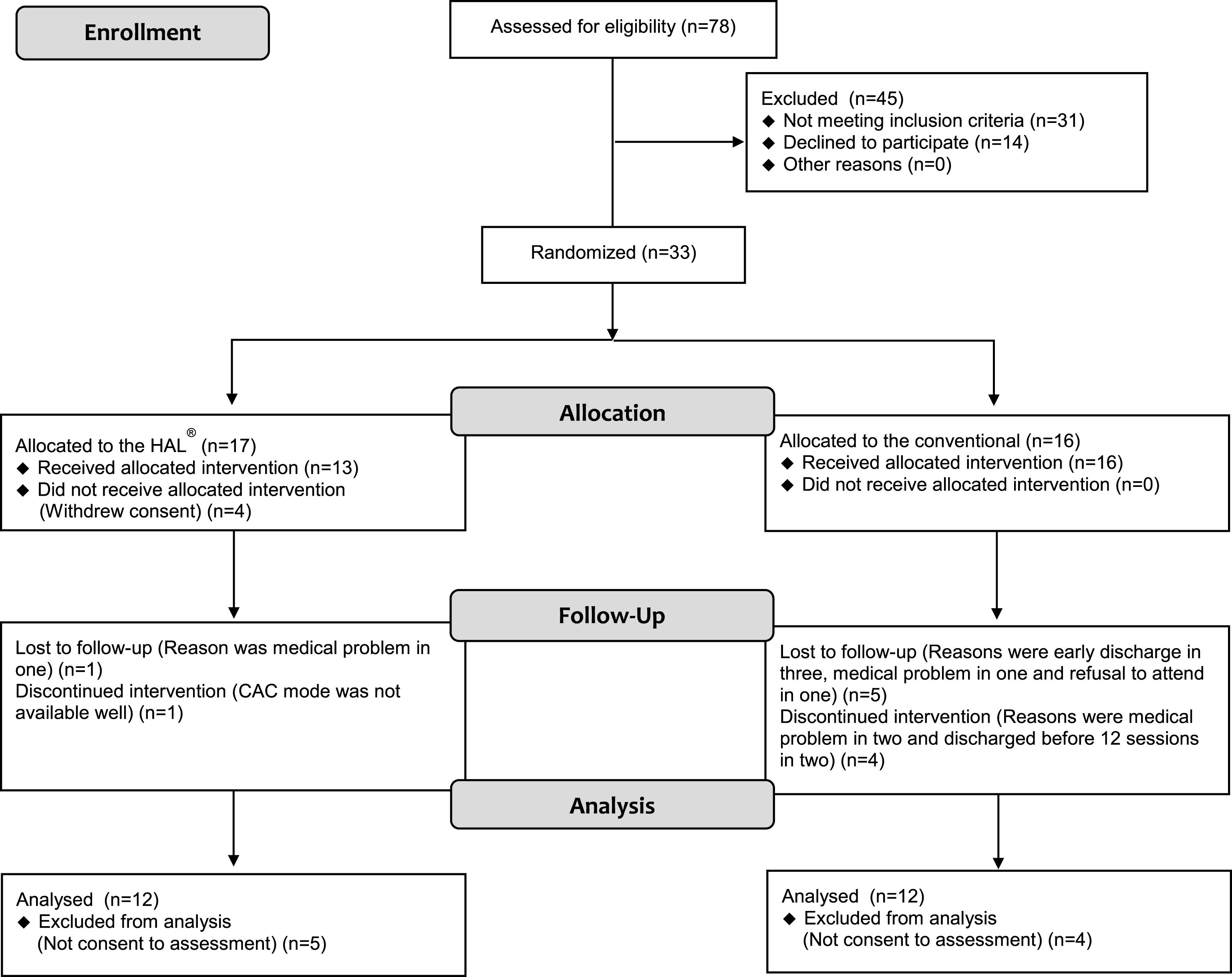
Flowchart of the study. CAC, cybernic autonomous control.
The ethics committees of the University of Tsukuba and of Tsukuba Memorial Hospital approved this study and written informed consent was provided by all of the subjects or their legal representatives. This study is registered in the University Hospital Medical Information Network (UMIN) clinical trials registry in Japan with the registration number UMIN000022335.
HAL® patients performed gait training using HAL® 3 times a week with a total of 12 HAL® training sessions (4 weeks). CGT patients performed CGT 3 times a week with a total of 12 CGT training sessions (4 weeks). The intervention goal and structure in both groups have been described in detail in our previous study (Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014).
Assessment
All measurements were done by physical therapists who were trained to perform standardized assessment procedures. The primary outcome measure was Functional Ambulation Category (FAC). Secondary outcomes measures were maximum walking speed, stride, cadence, 6-min walking distance, Timed Up-and-Go test, and Fugl-Meyer Assessment of the lower extremity.
All outcomes were assessed prior to training, after 12 sessions (4 weeks), and at 8 and 12 weeks after intervention initiation. These outcomes were assessed without wearing the HAL® because we wanted to show the effectiveness of the HAL® as a rehabilitation device, not as an orthosis for patients with stroke. Participants, therapists, and evaluators were not blinded to the treatment allocation.
Statistical analysis
The outcome measures in each group were compared prior to training, after 12 sessions (4 weeks), and at 8 and 12 weeks after intervention initiation. Interaction effects of groups (time×effect) were calculated using the mixed-effects model. SPSS version 23.0 was used for all statistical analyses. Statistical significance was set at P < 0.05.
Results
The HAL® group showed significant improvement in FAC after 12 sessions, and at 8 and 12 weeks post-intervention compared to the conventional group (P = 0.02). The interaction effects (time×effect) were significant for FAC. However, the secondary outcome measures did not differ between the two groups (Table 1). Values are expressed as number or mean ± SD.
Differences within groups and differences between groups with a 2-month follow-up
Differences within groups and differences between groups with a 2-month follow-up
Values are mean ± standard deviation or as otherwise indicated. FAC, Functional Ambulation Category, TUG, timed Up-and-Go test, LE, lower limb. #P value for Interaction, mixed-effects model.
The present study is the first randomized controlled trial to compare the medium-term efficacy of gait training using a single-leg version of the HAL® on the paretic side with CGT in recovery-phase stroke patients. The HAL® group showed significant improvement in FAC after 12 sessions, and at 8 and 12 weeks post-intervention compared to the conventional group. The interaction effects (time×effect) were significant for FAC. However, the secondary outcome measures did not differ between the two groups. The data indicate that gait training using HAL® is beneficial for hemiparetic, non-ambulatory, recovery-phase stroke patients.
A recent Cochrane review (Mehrholz, Elsner, Werner, Kugler, & Pohl, 2013) reported that electromechanical-assisted gait training in combination with physical therapy increased the odds of independent walking in participants (odds ratio: 2.39, 95% confidence interval: 1.67– 3.43; P < 0.01). Our data showed similar findings. The HAL® system enables such a repetitive gait training by providing motion assistance in response to the patient’s voluntary drive using an exclusive the cybernic voluntary control and the cybernic autonomous control technology (Lee & Sankai, 2005; Suzuki, Mito, Kawamoto, Hasegawa, & Sankai, 2007; Kawamoto, Hayashi, Sakurai, Eguchi, & Sankai, 2009). This new type of HAL®-assisted gait training might improve independent walking in patients with subacute stroke. (Kawamoto et al., 2013) reported that user control over the amount of assistance provided by HAL® is effected by voluntarily adjusting myoelectric activities. Thus, this mechanism forms a proprioceptive feedback loop that adjusts to each user.
Several studies have investigated the effects of locomotion training using HAL® for stroke patients (Kawamoto et al., 2013; Nilsson, Vreede, Häglund, Kawamoto, Sankai, & Borg, 2014; Watanabe, Tanaka, Inuta, Saitou, & Yanagi, 2014; Mizukami et al., 2016). Kawamoto et al. (2013) reported that the dependent ambulatory levels (FAC 2-3 with chronic stroke) showed significant differences in comfortable walking speed between before and after a total of 16 HAL® training sessions. The cybernic voluntary control mode was used during HAL® locomotor training in most patients. During locomotor training, the patients walked on a floor and were harnessed in a mobile suspension system. Mizukami et al. (2016) discussed that the harness walker system enabled patients to walk continuously without risk of falling. Therefore, the use of mobile suspension system played an important role in enhancing the HAL® training effect. In this present study, all subacute stroke patients were classified into the dependent ambulatory levels (FAC 0–3) prior to HAL® training but the cybernic voluntary control mode was available for only ten patients. Thus, two patients use had to the cybernic autonomous control mode to complete locomotion training. Of these, 1 subject exhibited reduced dependence on walking assistance and 1 did not change. It is still unclear whether gait training using HAL® benefits post-stroke patients who could not use the the cybernic autonomous control mode. Further study is needed to discuss the indications and the efficiency of each mode of HAL® for post-stroke gait training.
Other reports in the literature also detail the usage of a gait trainer in improvement of patient condition after stroke. Chua, Culpan, & Menon (2016) evaluated long-term efficacy and suggested that the use of an electromechanical gait trainer in combination with conventional physical therapy was as effective as conventional physical therapy alone for improving ambulation in subacute stroke. Morone et al. (2012) evaluated the long-term efficacy of robotic gait training in stroke patients at approximately 2 years after hospital discharge. To the best of our knowledge, this is the longest follow-up study reported at this time. In our study, the HAL® group showed greater efficiency in the improvement of independent walking compared with that observed with CGT at 1 and 2 months after intervention. Although this is a short-term result, gait training using HAL® was shown to be superior to CGT in subacute stroke patients. Further study is needed to evaluate longer follow-up periods (months to years) of gait training using HAL®. Such data will allow for comparisons with previously published long-term studies.
There are few limitations in our study. The statistical power was low because of the small number of subjects. In addition, we could not exclude observer bias because the same therapists implemented training and assessment; there was no blinding in the treatment allocation. Furthermore, regarding the sufficient duration and the long-term efficacy of gait training using HAL®, we will attempt to answer these questions in our future investigations.
Conclusions
In conclusion, the present study is the first randomized controlled trial with a 2-month follow-up period to compare the medium-term efficacy of gait training using a single-leg version of HAL® on the paretic side with CGT in recovery-phase stroke patients. The results suggested that a gait training program based on HAL® may improve independent walking more efficiently than CGT at 1 and 2 months after intervention. Further study is needed to evaluate the long-term efficacy of gait training using HAL®.
Conflict of interest
None to report.