
Abstract
Introduction
Postural instability is one of the most disabling features of Parkinson Disease (PD) and is potentially responsible for an important loss of autonomy due to falls and injuries. Both axial rigidity and poor trunk coordination contribute to the poor stability of PD patients in response to shoulder pulling or backward body sway, pointing to a dysfunction of postural reflexes. This could result from impaired sequencing of automatic motor programs for anticipatory postural corrections and/or impaired motor learning (Krebs, McGibbon, & Goldvasser, 2001).
The aim of this study was to assess differences in anticipatory control of postural stability function between subjects affected by PD with comorbid leukoaraiosis (LPD), idiopathic Parkinson disease (IPD), and elderly healthy subjects (EHS) as control group. In IPD, poor stability is clinically detected later in the course of the disease and is generally considered a sign of more advanced PD. In LPD, comorbid white matter disease is a greater determinant of axial motor impairment, leading to impaired postural responses, than nigrostriatal dopaminergic denervation per se (Bohnen et al., 2011).
We focussed on the postural vertical alignment pattern while expecting a series of balance perturbations. Dynamic posturography using a movable platform may be the most pertinent measure for understanding the mechanisms contributing to impaired postural responses in PD. Posturographic protocols allow to simulate everyday life unexpected perturbations, such as with slipping or tripping, which require the patient to respond immediately. The posturographic trajectory of the body during quiet standing or while expecting a perturbation can be represented by the Center of Pressure (CoP) defined as the point of application of the ground reaction forces under the feet (Winter, 1995). Following the first trial (an unexpected backward platform translation along the antero-posterior axis), subjects were exposed to repeated balance perturbations with the aim at investigating how previous experience modulated the preparatory postural pattern (Popa, Bonifazi, della Volpe, Rossi, & Mazzocchio, 2007, 2008).
This knowledge is critical in the light of potential therapeutic interventions targeting specific mechanisms and dysfunctions using ad hoc rehabilitation protocols and strategies (Cioncoloni et al., 2016).
Methods
Subjects
This repeated measure design study involved 16 patients with Parkinson’s disease and 8 age/weight matched elderly healthy subjects (EHS). Patients met the UK Parkinson’s Disease Society Brain Bank Research Centre clinical diagnostic criteria for Parkinson’s disease (Hughes, Ben-Shlomo, Daniel, & Lees, 1992). Patients were selected based on having mild-to-moderate severity of disease according to Hoehn and Yahr stages (Hoehn & Yahr, 1998) and postural instability. All participants were outpatients, and were not affected by unstable cardiovascular disease or other chronic conditions that could interfere with their safety during the assessment. All patients were ambulant and independent with Activities of Daily Living (ADL) and had no difficulty in following instructions or in comprehending the aims of the study. In addition, patients had no other neurological conditions or mental deterioration (Mini Mental State Examination score >24) (Dick et al., 1984).
Patients were subclassified into two subtypes depending on whether or not white matter abnormalities (WMA) were present at MRI scans. WMA ranged from mild-to-moderate according to the categorization into the three severity classes of the scale of Fazecas et al. (Fazekas, Chawluk, Alavi, Hurtig, & Zimmerman, 1987).
Patients used their regular anti-Parkinson medication, and testing took place during subjective ON phase and in the afternoon. All subjects gave written informed consent prior to the experiments, which were approved by the local ethical committee.
Clinical assessment
All participants were assessed by the Unified Parkinson’s Disease Rating Scale (UPDRS) motor (Items 18– 31) subscore (Goetz et al., 2008). The pull-test (UPDRS Item 30) was performed by the same examiner in all subjects using the protocol recommended by Visser et al., 2003 and the UPDRS scoring system. Two trials were conducted to be sure that participants understood the task, and the lowest (best) score was recorded. The UPDRS and related subscales have showed high reliability ad high psychometric properties in describing patients’ clinical status (Siderowf et al., 2002).
Posturography protocol
Postural stability was evaluated with the The Equitest system (Neurocom Int. Inc., Clackamas, OR, USA, see Fig.1). The Equitest System includes a movable support surface and a visual surround. Strain gauges within the platform measure the tangential forces and the total vertical force exerted by the feet resting upon its surface. Foot position and stance width are standardized and depend on subject’s height. Force plate changes are measured along the medio-lateral (ML) axis, i.e X-axis, and the antero-posterior (AP) axis, i.e. Y-axis. In addition, the platform can be moved backwards or forwards according to a pre-defined algorithm. The platform movement is proportional to subject’s height: it covers 0.5* (height in cm/180) centimeters in 200 ms, which would be the equivalent of a 0.7 degree sway.

The Equitest System.
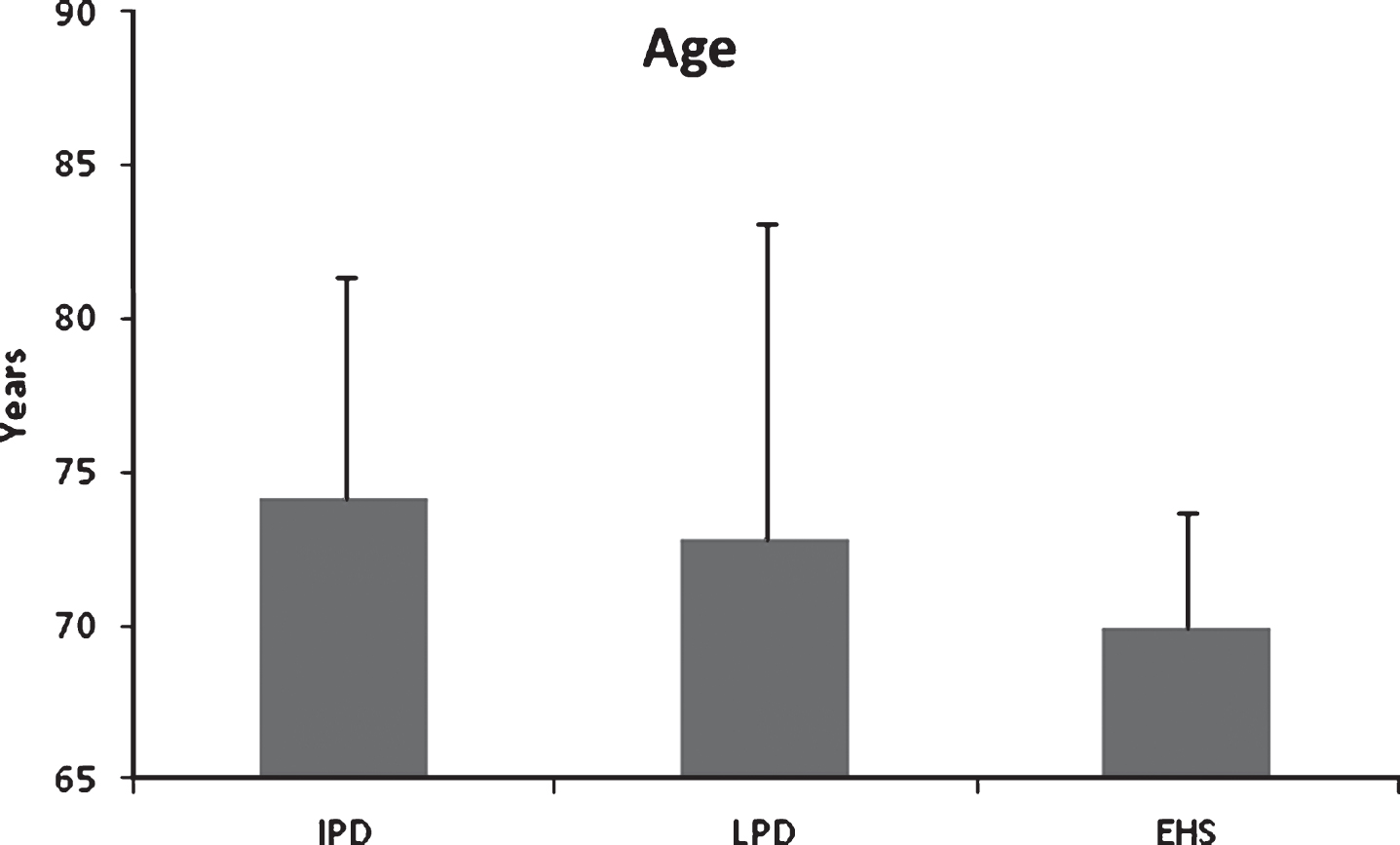
The figure shows the mean age (SD) in the three groups of subjects. No significant differences were found. Legend: IPD, Idiopathic Parkinson’s Disease; LPD, Leukoaraiosis Parkinson’s Disease; EHS, Elderly Healthy Subjects.
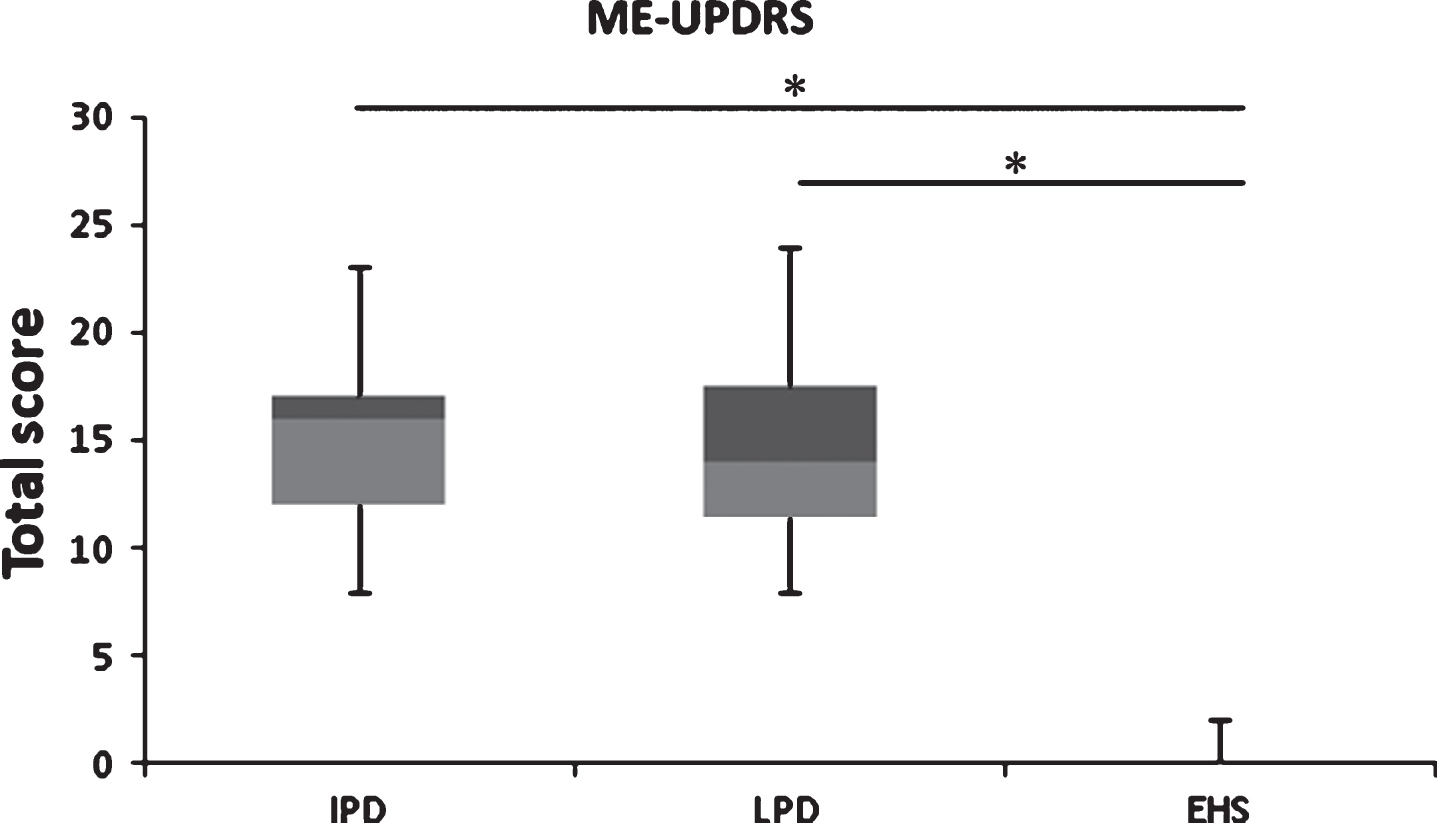
The figure shows the median and IR of ME-UPDRS total score in the three groups of subjects. Significant differences were found between IPD vs EHS and LPD vs EHS. Legend: ME-UPDRS, Motor Examination of the Unified Parkinson’s Disease Rating Scale; IPD, Idiopathic Parkinson’s Disease; LPD, Leukoaraiosis Parkinson’s Disease; EHS, Elderly Healthy Subjects.
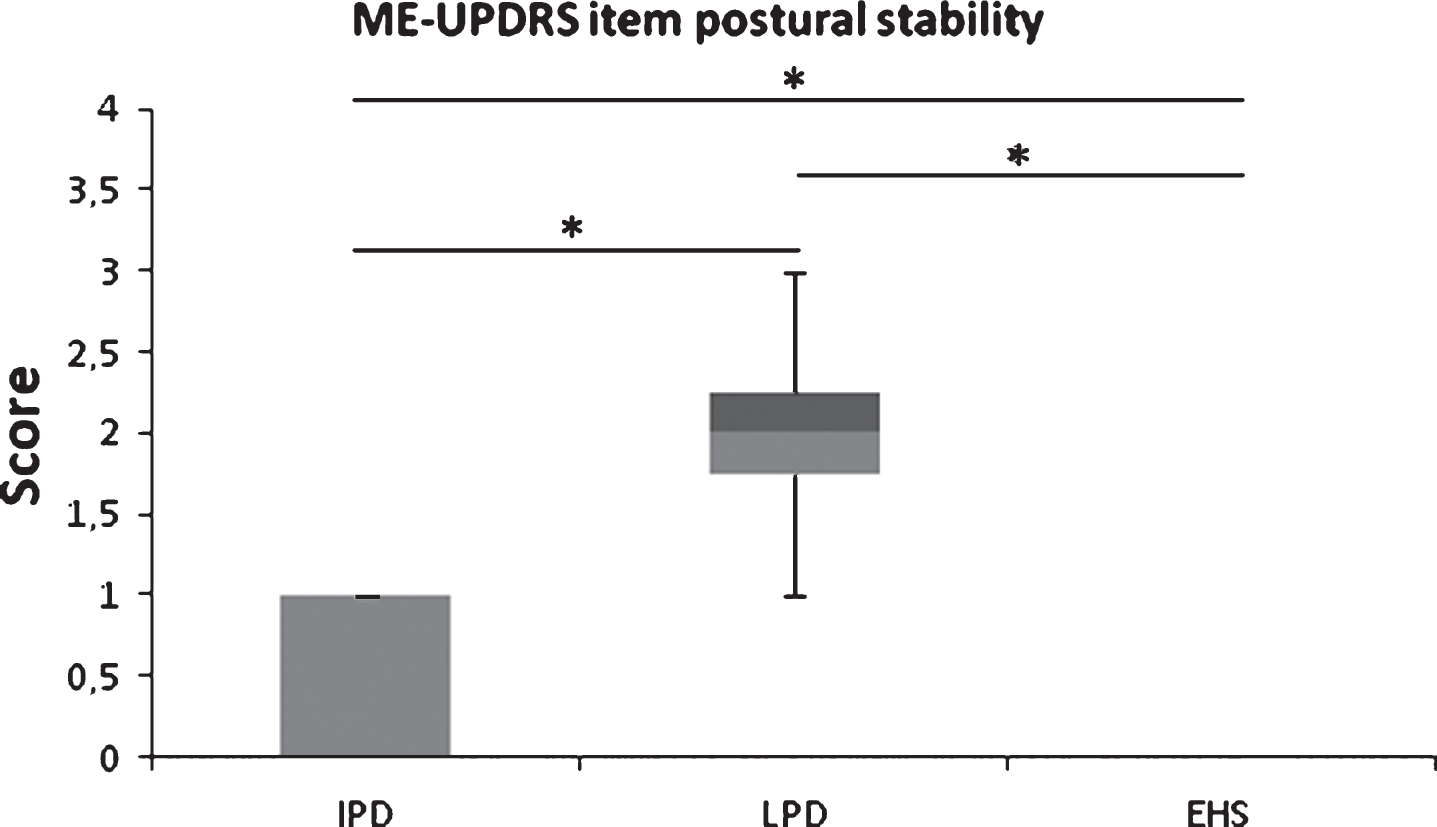
The figure shows the median and IR of ME-UPDRS item 30 “postural stability” in the three groups of subjects. Significant differences were found between IPD and EHS, between LPD and EHS, and between IPD and LPD indicating the presence of larger postural instability in LPD patients. Legend: ME-UPDRS, Motor Examination of the Unified Parkinson’s Disease Rating Scale; IPD, Idiopathic Parkinson’s Disease; LPD, Leukoaraiosis Parkinson’s Disease; EHS, Elderly Healthy Subjects.
Subjects stood barefooted with ankles directly above the X-axis of the force platform and feet equidistant from the Y-axis, their arms hanging loosely by their sides, facing the visual surrounding and maintaining optic fixation straight ahead on a small cloud drawn at the center of the scenery. A safety harness was used to prevent falls.
For this study, subjects were standing while expecting three backward translations of the platform (backward platform translation total task = 2.5 s). There were random delays of 1.5–2.5 s between platform movements to prevent possible sway-translation resonance contamination between trials. In the subsequent data analysis, data of the “pre-backward platform translation period”, lasting 500 ms, were analyzed in order to investigate changes in the “preparatory mode”, prior to translation. The position of the CoP was recorded with a 100 Hz sampling rate. The AP (Y-axis) displacements (cm) of CoP were stored for off-line analysis.
To compare age and clinical assessments of the three groups, a statistical analysis was performed using one way ANOVA and the U Mann-Whitney test, respectively. If these tests were significant, the presence of a statistical difference between each group was investigated with the Bonferroni post-hoc test.
The CoP position in the Y-axis (CoP-Y), collected from three trials, was calculated and normalized by subject’s height. Each factorial combination was tested for normal distribution with Shapiro-Wilk test. The normal distribution was assumed since each factorial combination showed a p-value >0.05. To test changes in CoP-Y position between the three pre-backward platform translation periods in each group, a two-way repeated measures ANOVA with factors “group” at three levels (IPD, LPD, EHS), and with factor “trial” at three levels (trial 1, trial 2, trial 3) was run. If the ANOVA resulted significant, the CoP-Y position in each of the three trials within each group was compared by applying Bonferroni post-hoc test. The levels of significance were set at p < 0.05.
Results
Table 1 describes the main subjects’ characteristics. There was no statistical difference in age among groups (p = 0.533).
Subject details at time of the assessment
Subject details at time of the assessment
Legend: ME-UPDRS, Motor Examination of the Unified Parkinson’s Disease Rating Scale. Item 30, “Postural Stability”; IPD, Idiopathic Parkinson’s Disease; LPD, Leucoaraiosis Parkinson’s Disease; EHS, Elderly Healthy Subjects. aMean (standard deviation). bMedian (interquartile range).
The clinical examination by the motor examination (ME)-UPDRS showed significant differences among groups in the total score (p < 0.001). Subsequently, the post-hoc comparisons showed a statistical significant difference in the UPDRS total score between groups IDP and EHS (p < 0.001), between LPD and EHS (p < 0.001), whereas no difference was found between IPD and LPD (p = 0.711).
When the post-hoc analysis was performed by comparing the UPDRS item 30 “postural stability” score, significances were found among the three groups (IPD vs EHS, p = 0.009; LPD vs EHS, p < 0.001; IPD vs LPD, p < 0.001), pointing to a greater dysfunction in postural reflexes in LPD.
Figure 5 shows the CoP-Y (SE) values collected from the three trials in each group normalized by height. When the overall CoP-Y data of assessments between the three groups were compared, no significant main effects was evident (F1–22 = 0.121; p = 0.887). Similarly, no main effects were found in the comparison between data of the three trials (F1–22 = 0.146; p = 0.866). On the contrary, the interaction between factors “group”/“trial” was significant (F1–22 = 7.28; p < 0.001). The Bonferroni post-hoc comparisons showed no statistical differences between the three trials within subjects in the group IPD (trial 1 vs trial 2, p = 0.243; trial 1 vs trial 3, p = 0.221; trial 2 vs trial 3, p = 1.00), as well as in the group EHS (trial 1 vs trial 2, p = 0.453; trial 1 vs trial 3, p = 0.177; trial 2 vs trial 3, p = 0.667) while a significantly backward CoP-Y position was observed within the group LPD in the comparisons between the trial 2 and the trial 3 vs the trial 1 (trial 1 vs trial 2, p = 0.026; trial 1 vs trial 3, p = 0.020; trial 2 vs trial 3, p = 1.00).
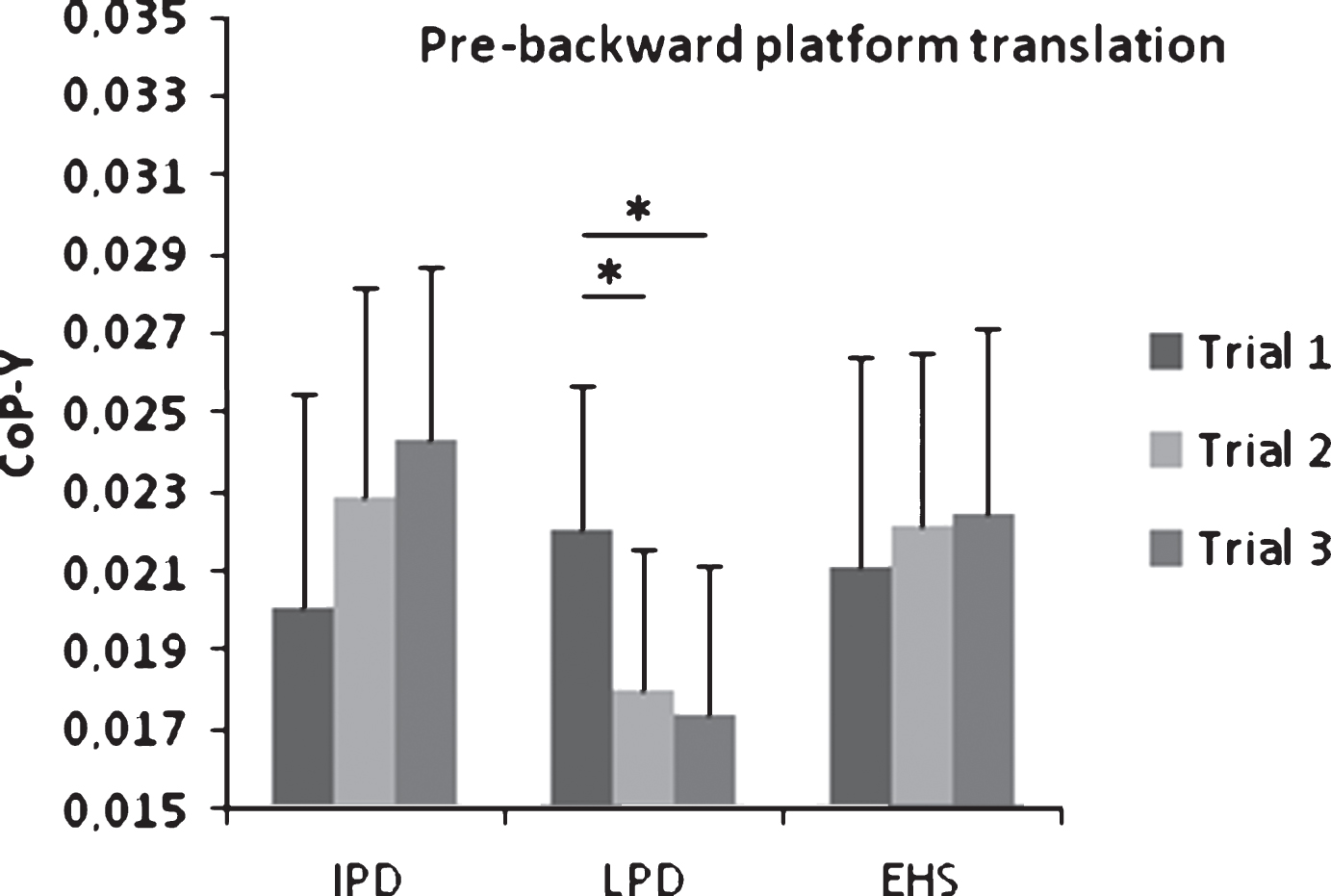
The figure shows the CoP-Y (cm, normalized by subjects height) (SE) values collected from the three trials in each group. In the period preceding the backward platform translations, the CoP-Y was positioned significantly backward in the trial 2 and in the trial 3 when compared with the trial 1 in LPD. Legend: CoP-Y Center of Pressure y-axis; IPD, Idiopathic Parkinson’s Disease; LPD, Leucoaraiosis Parkinson’s Disease; EHS, Elderly Healthy Subjects.
There was no difference in age among LPD, IPD and EHS. As expected, there was a significant difference in the ME-UPDRS between the pathological group (LPD and IPD) and the control group (EHS).
Standing while waiting for a series of backward translations of the support platform makes healthy subjects progressively shift forward the CoP-Y (Popa et al., 2007, 2008). Similarly, decreases in the amount of recruited muscle activity and reductions in the extent of trunk excursion while balancing during a series of backward perturbations have been reported (Visser et al., 2003). Altogether, these data suggest that optimization of postural control strategy be based on the subjects’ training responses.
The present results show that after experiencing the first backward translation, LPD patients positioned the CoP-Y significantly backward while waiting for the second and third platform translations, with respect to their COP-Y position in preparation for the first platform backward translation. This was not the case for the IPD and EHS groups who showed a preserved training response with no significant differences in the CoP-Y position among the repeated perturbation trials. The posturographic behaviour in LPD patients is suggestive of inability to rescale an effective preparatory postural pattern to known, repeated perturbations. This is coherent with the clinical data assessing postural stability by the ME-UPDRS item 30 indicating a larger postural instability in the LPD group compared to the IPD group.
It has been reported that Parkinsonian patients show inflexible and weak postural responses (Frank, Horak, & Nutt, 2000; Termoz et al., 2008). These may arise from abnormal feedback gains due to impaired kinesthesia (Jacobs & Horak, 2006) and load leg extensors sensitivity (Dietz & Colombo, 1998) with subsequent inability to set postural responses (Kim, Horak, Carlson-Kuhta, & Park, 2009) that may affect CoP-Y re-allocation. While a peripheral contribution to altered premotor postural setting is possible, this did not seem to affect the posturografic performance of the IPD group.
Leucoaraiosis, as in our LPD group, is highly implicated in axial motor impairment and its severity significantly correlates with retropulsion test scores, UPDRS rating of posture, worsening motor performance that is independent of the nigrostriatal dopaminergic denervation level (Bohnen et al., 2011), as represented by the IPD group.
Similarly, in elderly people falls and mobility are related to white matter loss in frontal lobe but not to basal ganglia dysfunction (de Laat et al., 2011; de Laat et al., 2012; Poggesi et al., 2013). This suggests that the complex motor network (i.e., prefrontal cortex, subthalamic nucleus, pedunculopontine/cuneiform nucleus complex) that guarantees the integrity of central coordination of stance and gait may be challenged through a critical amount of white matter lesions in subcortical regions (Buchman, Leurgans, Nag, Bennett, & Schneider, 2011), pathogenetically linked with small vessel cerebrovascular disease (Pantoni, 2010; Buchman et al., 2011). Specifically, the frontal lobe plays a crucial role in preparation for perturbation of balance (Mihara, Miyai, Hatakenaka, Kubota, & Sakoda, 2008), while a decrease in the parieto-occipital white matter volume has been associated with balance disturbance (Novak et al., 2009), possibly resulting from impaired processing and integration of multiple sensory modalities in the parietal lobe (Murray et al., 2010). Higher-level gait and postural stability disorders may be a consequence of frontal executive dysfunction characterized by inability to change motor programs rapidly and to process information from complementary, but competing, motor, cognitive, and limbic inputs.
The current literature on rehabilitation of postural impairment in PD patients suggests that interventions should be task-specific and task-oriented for postural control function, for example by improving feedback and feedforward postural reactions (Smania et al., 2010; Shen & Mak, 2015) and by facilitating postural sensory-motor integration (Capato, Tornai, Avila, Barbosa, & Piemonte, 2015). In terms of diagnostic utility, measuring the CoP-Y change or improvement in the preparatory posturographic pattern to a series of backward balance perturbations may give important indications on trainability of balance in the PD population helping to differentiate IPD patients with a preserved training response who, presumably, will maximally benefit from neurorehabilitation programs based on recovery of function.
On the other hand, in LPD patients the presence of executive function deficit and reduced structural and/or functional connectivity of the circuitries subserving the coordination of stance and gait unfavourably predicts to challenging balance rehabilitation strategies suggesting that balance rehabilitation outcome depends on the state of frontal lobe white matter (King et al., 2015) and related motor learning capability. In LPD patients as well as in those who show inability to rescale an effective preparatory postural pattern, the rehabilitation strategy should be based more on “compensative reeducation” than on “recovery of functions”, keeping in mind that these patients have a higher risk of falling. Compensatory training procedures may be boosted by the application of neuromodulatory protocols aiming at inducing functionally meaningful changes in the CoP position (Cioncoloni et al., 2016).
In conclusion, this study shows that that PD patients affected by leukoairosis (LPD) are unable to rescale an effective preparatory postural pattern to known, repeated backward balance perturbations suggesting impaired sensory-motor integration and processing for postural strategy selection. On the other hand, anticipatory postural patterns remain effective in IPD patients, as well as in healthy subjects of similar age. These findings may suggest that different rehabilitation strategies are needed to manage postural impairment in the PD population.
Conflict of interest
We declare that there are no financial and personal relationships with other people or organizations that could inappropriately influence (bias) our work.