
Abstract
BACKGROUND:
Many patients who have suffered from a stroke show decreased walking ability, characterized by asymmetric gait. For such patients, the recovery of symmetry in walking is important.
OBJECTIVES:
The purpose of this study is to investigate the effect of visual feedback with rhythmic auditory cue on treadmill gait in persons with chronic stroke.
METHODS:
Seventeen chronic subjects who have been diagnosed at least six months or before were recruited in G Hospital, located in Incheon. The subjects who were enrolled in this study were instructed to walk randomly on a treadmill: treadmill with visual feedback and rhythmic auditory cue (VF+RAC), treadmill with visual feedback (VF), general treadmill (Control; non-feedback). Three factors were observed and estimated: paretic step length, non-paretic step length, spatial asymmetry ratio at comfortable speed. Also, in VF and VF+RAC, calibration of feedback accuracy was measured.
RESULTS:
Results showed that paretic step length and spatial asymmetry ratio were significantly improved in VF+RAC compared to that of the VF and control (p < 0.05). Accuracies of paretic and non-paretic leg were significantly increased in VF+RAC than that of the VF (p < 0.05).
CONCLUSIONS:
According to this result, it seems that application of VF+RAC in treadmill gait significantly improved gait of these patients. Also, we can conclude that VF+RAC in treadmill gait is thought to be useful in clinical settings where there are many chronic patients who are in need of improvement in their gait ability.
Introduction
Most persons with stroke suffer from impaired physical mobility, sensation vision and cognition (O’Sullivan & Schmitz, 2007). The persons with stroke suffer from functional disability in walking due to reduced walking speed and balance (Ivey, Macko, Ryan, & Hafer-Macko, 2005; Michael, 2002; Newman et al., 2003; Patterson et al., 2007; von Schroeder, Coutts, Lyden, Billings, & Nickel, 1995). The characteristics of walking difficulty after stroke trigger reduced walking abilities including reduced walking speed, cadence, step length, and stride length (von Schroeder et al., 1995; Wall & Ashburn, 1979), as well as asymmetrical walking patterns (Brandstater, de Bruin, Gowland, & Clark, 1983; Kim & Eng, 2003; Roth, Merbitz, Mroczek, Dugan, & Suh, 1997; Wall & Turnbull, 1986). For such patients, the recovery of symmetry in walking improves the walking speed and efficiency (Patterson, Gage, Brooks, Black, & McIlroy, 2010; Titianova, Peurala, Pitkanen, & Tarkka, 2008), musculoskeletal damage of lower limbs (Norvell et al., 2005), and the risk of bone density loss in the paralyzed leg (Jorgensen, Crabtree, Reeve, & Jacobsen, 2000). Therefore, the recovery of symmetry in walking is more important, thus further requiring a therapeutic intervention to enhance such ability.
Begg et al. (2014) reported that the treadmill training applied with the visual feedback of kinematic gait factors regarding the lower limbs of persons with stroke were effective in adjusting the trajectory of feet. Lewek et al. (2012) stated that when treadmill training with visual feedback and proprioceptive feedback was applied on two persons with chronic stroke, there were more improvements in the walking speed and the symmetry of walking than in the previous study regarding conventional treadmill training (Hornby et al., 2008; Patterson, Rodgers, Macko, & Forrester, 2008; Silver, Macko, Forrester, Goldberg, & Smith, 2000). They reported that the visual feedback, which was applied to recover the walking symmetry during treadmill gait training, was effective in improving the gait of persons affected by stroke (Lewek, Feasel, Wentz, Brooks, & Whitton, 2012). Also, among the therapies, rhythmic auditory cues provide rhythmic cue during exercise, to successfully elicit the synchronization of time of movement control (Thaut et al., 2007). The rhythmic auditory cue enhances the walking ability of persons with stroke, as was reported from numerous studies (Mandel, Nymark, Balmer, Grinnell, & O’Riain, 1990; Prassas, Thaut, McIntosh, & Rice, 1997; Schauer & Mauritz, 2003; Thaut, McIntosh, & Rice, 1997; Van Peppen et al., 2004), and, is thought of as being additionally applied to the other interventions for walking (Thaut et al., 2007).
Persons affected by stroke perform asymmetrical walking, exhibit shorter step and stride lengths compared to unimpaired walking (Brandstater et al., 1983; Olney, Griffin, & McBride, 1994; Turnbull, Charteris, & Wall, 1995). Also, in the study which the treadmill gait and rhythmic auditory cues were conducted together (Roerdink, Lamoth, Kwakkel, van Wieringen, & Beek, 2007), persons with stroke exhibited shorter step and stride lengths compared to the normal people. Also, in a treadmill gait study, which the rhythmic auditory cues were applied to both lower extremities during gait, temporal asymmetry was reduced while the spatial asymmetry affected by the auditory cue did not improve (Roerdink et al., 2009). Therefore, mediation is required to improve the spatial symmetry of walking while also increasing the step length and stride length at the same time.
However, regarding treadmill training with persons with chronic stroke, there are only a few studies focused on the combined influence of visual feedback and rhythmic auditory cues on the mediation of asymmetrical walking. Basic data with respect to how the visual feedback and rhythmic auditory cues affect the treadmill walking are necessary. Therefore, in this study, the influence of visual feedback on step length and the effect of rhythmic auditory cues on step cycle initiation during treadmill gait should be investigated as a possible mediation for the asymmetric walking, in order to suggest an appropriate treatment for persons with chronic stroke.
Methods
Participants
Among the persons with stroke who were hospitalized in the G hospital in Incheon, seventeen patients who had agreed to the terms of the experiment were selected as the subjects of this study. The inclusion criteria were as follows: (1) patients who were diagnosed with stroke more than 6 months ago, (2) patients who were capable of performing independent walking without using an assistance device, (3) patients without critical cognitive impairments with MMSE scores over 24 and who could perform the equipment evaluation according to given instructions, (4) patients without hearing disabilities and (5) patients with a Brunnstrom’s stage of greater than 4. The exclusion criteria were as follows: (1) patients with orthopedic disabilities that affected walking, (2) patients with cardiac diseases, (3) patients with unregulated hypertension and (4) and patients with hemianopsia or dysopia. The subjects were carefully explained of the contents, procedures, and risk factors of the study, and agreed to participate in the experiment after they had signed the consent of agreement forms. The current study was approved by the Institutional Review Board of Sahmyook University. General characteristics of the subjects are as shown in Table 1.
General characteristics of the subjects (N = 17)
General characteristics of the subjects (N = 17)
aMMSE: Mini Mental State Examination, bMBI: Modified Barthel Index, cMAS: Modified Ashworth Scale of the paretic leg, dMonth, eBrunnstrom Stage of the paretic leg, fHemorrhage.
The present study was a cross-sectional study. The treadmill gait along with the visual feedback and rhythmic auditory cues, as conducted in this study, were implemented by allowing the subjects to walk while providing visual feedback on their step length with the target step length, and rhythmic auditory cues on the step cycle initiation were provided. The implementation method was provided by the gait analysis module of the Reoambulator® (Motorika Ltd., USA, 2011). First, in order to measure the basic initial variables during the treadmill gait, the Reoambulator® was used to measure the comfortable walking speed on the treadmill, and the step length was measured on both the affected side and unaffected side. Based on the step lengths of the affected and non-affected sides, the visual feedback and rhythmic auditory cues were configured. The visual feedback was applied to the target step length on the side with the longer step of the patient. The feedback to the target step length was provided to the patient in the form of three colors, along with the actual step length in real time. The green indicated that the deviation from the target step length was within 10 cm, while the blue indicated that the deviation ranged from 10 to 30 cm. The red indicated that the deviation was more than 30 cm. The rhythmic auditory cues regarding the step cycle initiation was provided by the gait analysis module program of the Reoambulator® by synchronizing the treadmill walking speed with the target step cycle initiation. To commence the randomly-ordered treadmill walking with the three conditions, the subjects were asked to select one amongst the three envelopes which contained a note indicating the walking order before the start of the experiment. The subjects walked for 5 minutes under the following randomized orders of: treadmill walking with visual feedback with rhythmic auditory cue (VF+RAC); only visual feedback (VF); and general treadmill gait (non-feedback, Control). The treadmill speed was identical in all three conditions based on the comfortable walking speed, as was measured prior the experiment. In the VF+RAC condition, the visual feedback and rhythmic auditory cues were provided through the 40-inch TV screen in front of the treadmill, in real time. Based on the auditory cues, the patients were advised to walk while adjusting their step lengths according to the target step length. Under the VF condition, only the muted TV screen without the rhythmic auditory cue was provided. In the control condition (non-feedback condition), the walking was conducted without the visual feedback or the rhythmic auditory cues.
During the experiment, two physical therapists were in position for observation in order to set the visual feedback and rhythmic auditory cue and to check the safety of the patients (Fig. 1). To exclude the carry-over effect, practice effect, and order effect that may be caused by the three conditions, each condition was applied in random order 1 hour after each condition application. Sufficient 30 minute-rest periods were provided between the treadmill gait conditions to minimize the overlapping effect.
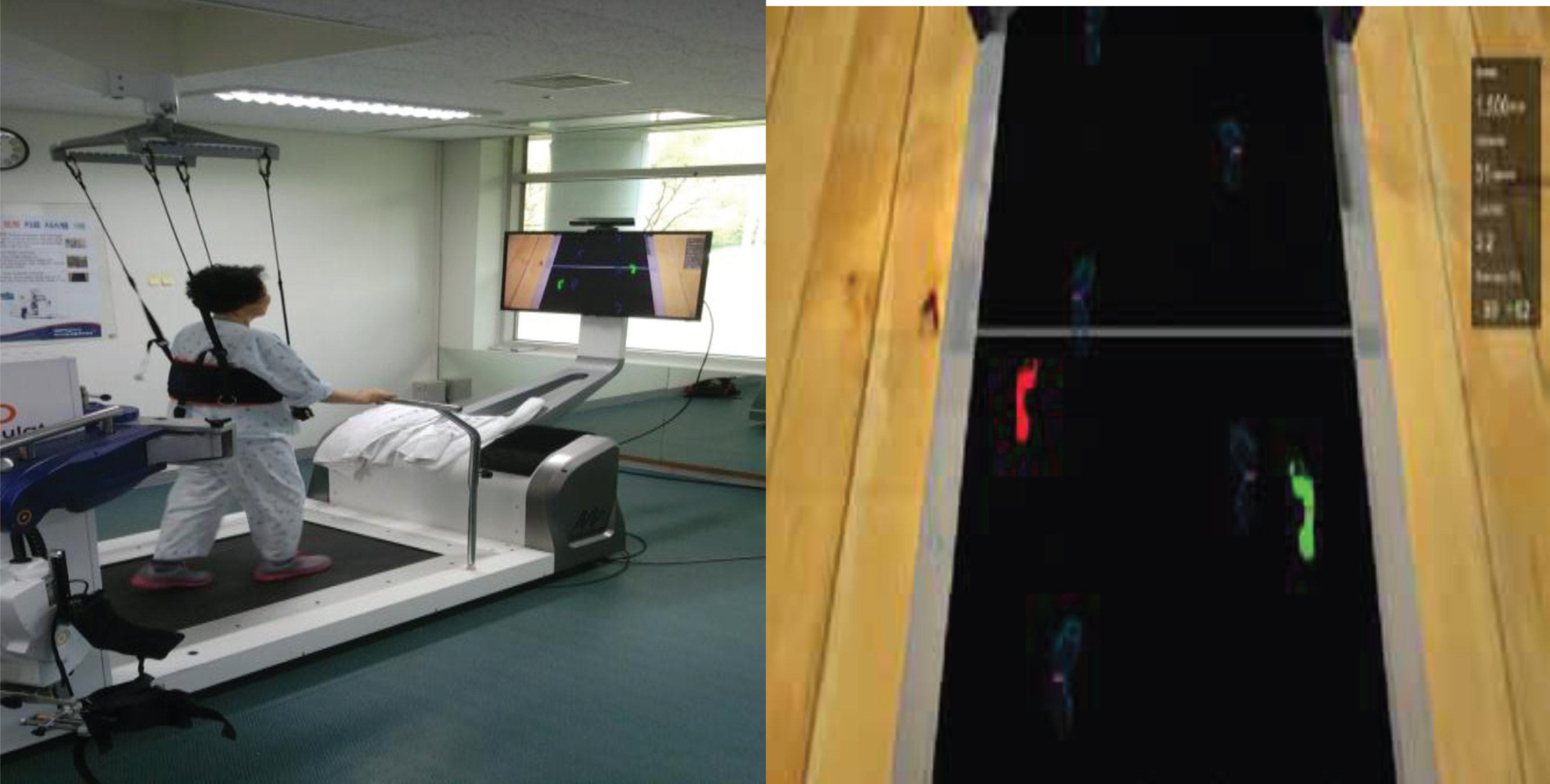
Visual feedback and rhythmic auditory cue applied on treadmill gait.
To measure the treadmill walking applied with visual feedback and rhythmic auditory cues and the variables of treadmill walking, the Motorika’s Reoambulator® was utilized. The gait analysis module is capable of monitoring the walking on the treadmill without wearing robotic legs and providing the visual feedback and rhythmic auditory cue in real time. The step length measurements were performed by the infrared sensors on the rail and both sides of the treadmill, and the accuracy of the step length, in comparison with the target step length was performed by measuring the distance (deviation) between the lower extremities, and by calculating the average values for each session. In this study, for each of the randomly ordered conditions, gait was conducted for five minutes to measure the step length of both the affected and unaffected sides three times repeatedly to calculate the average value. In the VF+RAC and the VF conditions, the accuracy of walking under feedback, and the satisfactory levels regarding the simplicity in understanding and following the instructions were satisfied by the Likert-type scale with 10 points as the perfect score. Also, spatial asymmetry was calculated by the difference in the step lengths between the affected and unaffected side (Tyrell, Roos, Rudolph, & Reisman, 2011).
Data analysis
All statistical analyses were calculated by SPSS 12.0 (SPSS Inc., Chicago, IL, USA), and the results were shown in the forms of means and standard deviations. The general characteristics of the subjects adopted the descriptive statistics. To compare the variables of walking under the three conditions (VF+RAC, VF and Control), a one-way repeated measures ANOVA was adopted. The least significant difference (LSD) was used as the post-hoc comparison. To compare the accuracy and satisfaction levels between the affected side and unaffected side under the VF+RAC, and VF conditions, the matching sample independent t-test was conducted. All the levels of significance in the statistical analyses were set as p < 0.05.
Results
As a result, during the treadmill walking under VF+RAC, VF and control conditions, the changes in the step lengths of the affected and non-affected sides, and the spatial asymmetries were found as shown in Table 2 and Fig. 2. The treadmill walking applied with VF+RAC showed significantly improved step length of affected side compared with the VF and control (non-feedback) conditions (p < 0.05), and the spatial asymmetry reduced significantly (p < 0.05). The VF condition showed significantly improved step length of the affected side compared with the control condition (p < 0.05). In all three treadmill gait conditions, the step length of the unaffected side did not show any significant difference. Also, the VF+RAC walking condition showed significantly increased accuracy between the affected and unaffected sides compared to the VF walking condition. The satisfactory level was significantly higher in the treadmill walking applied with VF+RAC (p < 0.05). (Table 2, Fig. 2).
Changes in gait parameters in VF+RAC, VF and control (N = 17)
Changes in gait parameters in VF+RAC, VF and control (N = 17)
aMean±SD. VF+RAC, treadmill with visual feedback and rhythmic auditory cue; VF, treadmill with only visual feedback; Control, non-feedback treadmill; P, paretic; NP, non-paretic. *Significantly different compared to the Control (p < 0.05), †Significantly different compared to the VF (p < 0.05).
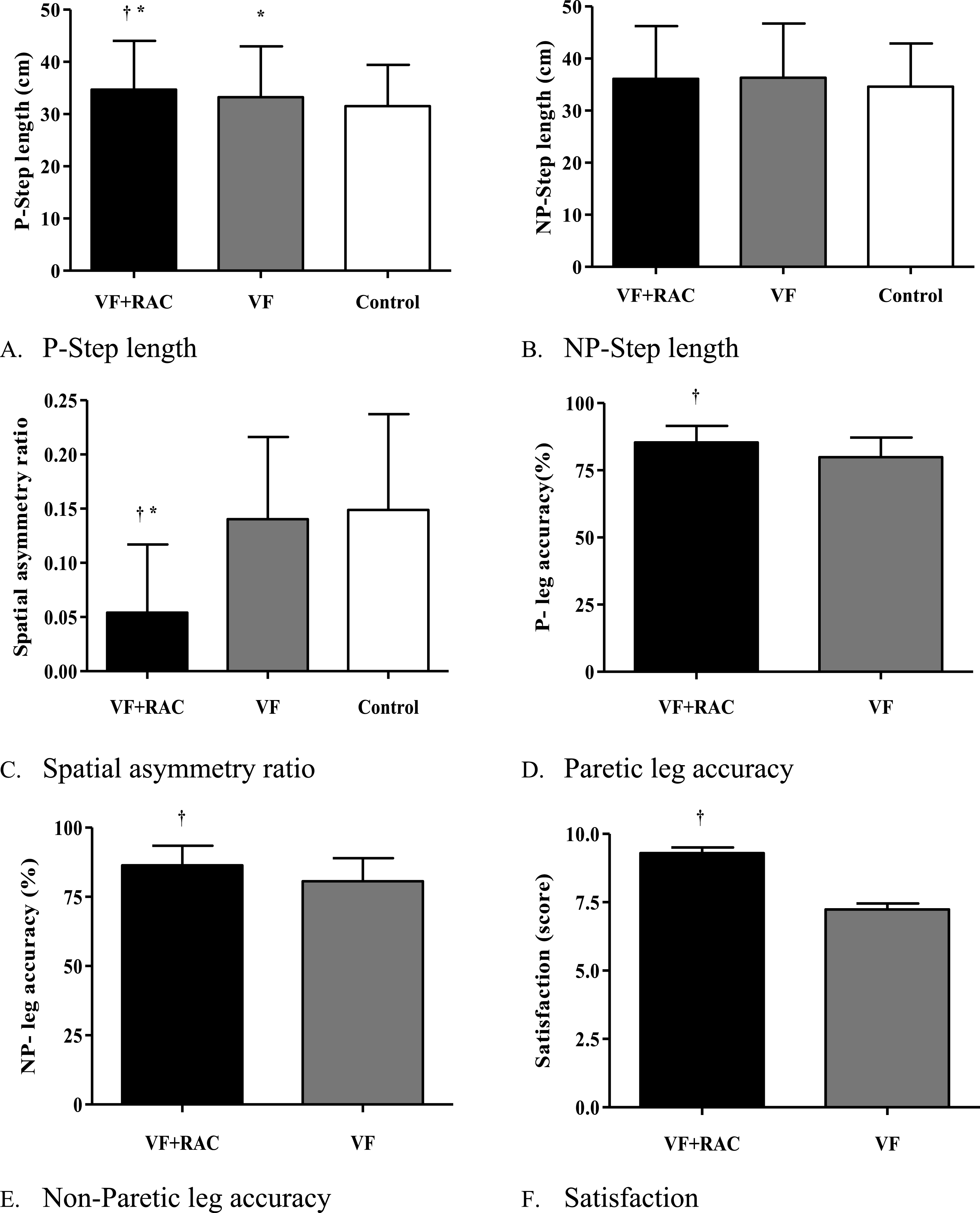
Comparison of gait parameters in VF+RAC, VF and control.
The treadmill walking applied with VF+RAC was found to increase the spatial symmetry and the accuracy of visual feedback assignment, as well as it is effect for additionally applying the auditory cue to understanding and facilitating the feedback assignment, in comparison with the case where only the visual feedback is applied to walking.
Lewek et al. (2012) conducted a study on treadmill gait applied with virtual reality-based visual feedback and proprioceptive feedback to examine the symmetry of step length and stance phase in two persons with stroke. Both patients were shown to have increased walking speeds and spatiotemporal symmetry in walking. Begg et al. (2014) conducted a study on treadmill training applied with visual feedback by providing information which designates the target range of “toe-ground clearance” (updated in real time), in order to raise the level of the toe during the minimum toe clearance (middle swing phase) of nine elderly persons and one persons with chronic stroke. As a result, it was found that the visual feedback was effective for the change in the trajectory of the toe and the reduction of toe drag during the middle swing phase. The increased step length on the affected side, as shown in this study, was found to be the effect of self-correction due to the visual feedback that was provided by the step length of the actual patient and the target step length, which were updated in real time. Therefore, it is thought that the step length of the affected side can be effectively increased by using visual feedback during gait training on a treadmill. Also, persons with stroke have the tendency to display impaired senses on the affected side, and are more dependent on visual senses in order to compensate for the loss while walking, such as by looking at their feet during walking (Walker, Hyngstrom, & Schmit, 2016). The utilization of visual feedback is considered to be effective in increasing the step length of the affected side.
However, when the visual feedback and the rhythmic auditory cues were applied together, the effect in increasing the step length of the affected side to the level of normal side (target step length) was significantly higher than the case where only the visual feedback was applied. The RAC has the advantage in that is uses repetitive auditory signals to synchronize the movement with time (Thaut et al., 2009), and the influence of instantaneous synchronization between the intrinsic time structure of such rhythmic cue and motor response increases the temporal predictability through the adjustment of intervals, thus making the adjustments to perform movement (Thaut et al., 2007). Such temporal rhythmic cues for movement cannot only adjust the timing and speed of movements, but also recovers the motor skills and enhances the temporal-spatial factor in terms of brain rehabilitation (Homberg, 2005; Hummelsheim, 1999; Molinari, Leggio, De Martin, Cerasa, & Thaut, 2003). Also, the rhythmic cue can facilitate the selection of speed variables such as the trajectory and acceleration of ideal movements, and increase the temporal accuracy while reducing the fluctuations during the motion (Thaut et al., 2007). The step length, which was further increased during the application of VF+RAC in the study, helps structuralize and adjust the movement of the affected leg. It is considered that through the repetitive auditory cues in the repetitive treadmill gait, the errors, which could have been triggered by the visual feedback, had decreased.
The visual feedback as applied in this study can be viewed as a closed-loop control system, where the error (deviation) of the patient’s step length is compared to the target step length and is visually indicated in real time, whereas the rhythm auditory cue can be viewed as an open-loop control system where the cue (feedback) regarding the step cycle initiation is provided regardless of the patient’s movement and deviation (Baram, 2013). Thaut et al. (2007) stated that the combination between externally-provided auditory rhythm and rhythmical movement can become an effective tool for improving the performance of movement. Also, in other studies, it was reported that the rhythmical and repetitive patterns in the movement can contribute positively to the walking ability of persons with stroke (Mandel et al., 1990; Prassas et al., 1997; Schauer & Mauritz, 2003; Thaut et al., 1997; Van Peppen et al., 2004). Applying the auditory cue along with the visual feedback can complement the shortcomings of the visual feedback. In other words, the difficulties experienced by the persons with stroke in which they cannot accurately adjust the step length on the affected side compared to the target step length, can be provided with additional feedback from the rhythmic auditory cues by acknowledging the step cycle initiation (Pelton, Johannsen, Chen, & Wing, 2010). At the same time, the patients can maintain the constant step cycle as well (Prassas et al., 1997). By correcting the deviations between the affected and non-affected sides, a higher level of accuracy can be accomplished. The satisfaction level was also significantly higher when applying the visual feedback along with the rhythmic auditory cues compared to when only the visual feedback was applied. This was due to the difference in the accuracy of feedback, which can be confirmed in real time, and it also proved that the additional application of rhythmic auditory cues during the treadmill walking facilitated the adjustment of the affected side more than the visual feedback alone.
The present study confirmed that the application of both the visual feedback and rhythmic auditory cue during the treadmill gait was effective in enhancing the walking pattern. However, since the number of subjects was small, it is difficult to generalize the study results. In addition, the current study was a cross-sectional study and only confirmed the spatial difference as to the application of visual feedback and the rhythmic auditory cue. Therefore, in the future, the influence of visual feedback and rhythmic auditory cues on the temporal and kinematic variables in walking should be investigated. Also, more studies should be focused on proving the clinical significance of treadmill training that is applied with visual feedback and rhythmic auditory cues through systematic training programs.
Considering the results of this study, regarding the treadmill gait of persons with chronic stroke, the application of visual feedback and rhythmic auditory cues was found to be effective in improving the walking pattern. Also, the method of this study can be suggested as an effective way to provide basic data for applying the visual feedback and rhythmic auditory cue, and to improve walking ability during the treadmill training.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Footnotes
Acknowledgments
This study was supported by Sahmyook University (2016).