
Abstract
Introduction
Over the last 20 years, evidence from basic science has influenced rehabilitation, particularly in the domain of stroke-related upper limb paresis. Stroke is the leading cause of disability in Western countries and is a growing burden for low- and middle-income countries (Feigin et al., 2014). Increasedunderstanding of neuroplasticity following brain damage and of factors that optimize motor recovery have led to new approaches to rehabilitation and the development of innovative therapeutic tools to implement these strategies. It is now well established that intensive and repetitive interventions can produce changes in sensorimotor neural networks, enhancing motor outcomes in the upper limb; moreover, there appears to be a dose-response relationship (Buma, Kwakkel, & Ramsey, 2013; Bütefisch, Hummelsheim, Denzler, & Mauritz, 1995; Cooke, Mares, Clark, Tallis, & Pomeroy, 2010; Feys et al., 2004; Han, Wang, Meng, & Qi, 2013; Kwakkel, Wagenaar, Twisk, Lankhorst, & Koetsier, 1999; Kwakkel et al., 2004; Lincoln, Parry, & Vass, 1999; Lohse, Lang, & Boyd, 2014; Wolf et al., 2006). In addition to these main features, several studies have highlighted the importance of active participation by the patient and the need for challenging exercises (Krishnan, Kotsapouikis, Dhaher, & Rymer, 2013; Shirzad & Van der Loos, 2015). Some researchers have therefore suggested that training should be minimally assistive (Casadio et al., 2009; Emken, Benitez, Sideris, Bobrow, & Reinkensmeyer, 2007), while others have stressed the importance of stimulating active participation in the training process as much as possible, even in patients with more severe impairment (Basteris et al., 2014). The use of control strategies that promote patient cooperation has been shown to improve active participation (Krishnan, Ranganathan, Dhaher, & Rymer, 2013). However, a key issue is can patients with severe stroke sustain their engagement during hundreds of movement repetitions?
Scientific knowledge has stimulated the development and the use of technological devices in order to incorporate elements of motor relearning into exercise-based training. Thus, rehabilitation robots are becoming increasingly integrated into post-stroke rehabilitation programs because they can offer safe, intensive, repetitive, sensor-based therapy for the paretic upper limb (Lo et al., 2010; Lum, Burgar, Shor, Majmundar, & Van der Loos, 2002; Mehrholz, Hädrich, Platz, Kugler, & Pohl, 2012; Volpe et al., 2000). Indeed, the most advanced robotic systems are equipped with sensors that can measure and record kinematic data from hand trajectories in order to quantify movement performance (Gilliaux et al., 2014; Zollo et al., 2011), as well as patient-robot interactions that indicate the amount of active participation by the patient (Duret, Hutin, Lehenaff, & Gracies, 2015). These measurements are carried out continuously during therapeutic exercises.
Despite a growing body of literature on the use and effectiveness of robot-mediated therapy, there is still a lack of evidence regarding patient-robot interactions and the effects of robotic paradigms on motor performance (Kahn, Lum, Rymer, & Reinkensmeyer, 2006). Assist-as- needed training is the most commonly applied robotic algorithm (Basteris et al., 2014). Although it is possible to calculate the assistance provided by the robot and therefore to deduce the amount of patient activity, this is not routinely done and has not been studied. It is therefore not known if patients tend to minimize, stabilize or maximize their activity. Furthermore, there is a paucity of research on the optimal kinematics of repeated motor activity (motor input) that stimulate motor skill acquisition. It has been hypothesized that neuronal networks might encode motion kinematic parameters in the learning processes (Kantak, Jones-Lush, Narayanan, Judkins, & Wittenberg, 2013), thus it may be important to consider the kinematic parameters of movements performed in rehabilitation. This is very difficult using classical rehabilitation methods but is possible using robotic instruments.
The aim of this retrospective study was to characterize upper limb motor activity during robotic training sessions in patients with severe stroke by analyzing patient participation and motor performance within and across training sessions that consisted of hundreds of active- assisted movements.
Material and methods
Subjects
This retrospective study was conducted in the Neurorehabilitation unit of Les Trois Soleils hospital. Charts of patients involved in the upper limb robotic program were reviewed, based on the following inclusion criteria: age over 18, first ever and single stroke confirmed on CT or MRI scan less than 6 months previously, and completion of at least 640 movements per session.
Sixteen patients met the inclusion criteria. Their characteristics are summarized in Table 1.
Participant characteristics
Participant characteristics
Results are expressed as mean±SD. F: Female; M: Male; H: hemorrhagic; I: ischemic; L: Left; R: Right; FMA: Fugl Meyer Assessment; SD: Standard deviation.
The InMotion Arm robot (Interactive Motion Technologies, Inc., Watertown, MA, Fig. 1), an end-effector robot, was used. This interactive robotic system is a 2 translational degree of freedom device that emphasizes shoulder (flexion/extension) and elbow (flexion/extension) movements in the horizontal plane. This device comprises several training modes, including a performance-based (or assist-as-needed) program that adjusts forces to assist or challenge the patient’s movement according to his/her motor performance. If a task cannot be completed volitionally, the robot provides assistance to reach the target. Moreover if the patient does not initiate the movement within 2 seconds, the robot initiates the movement.
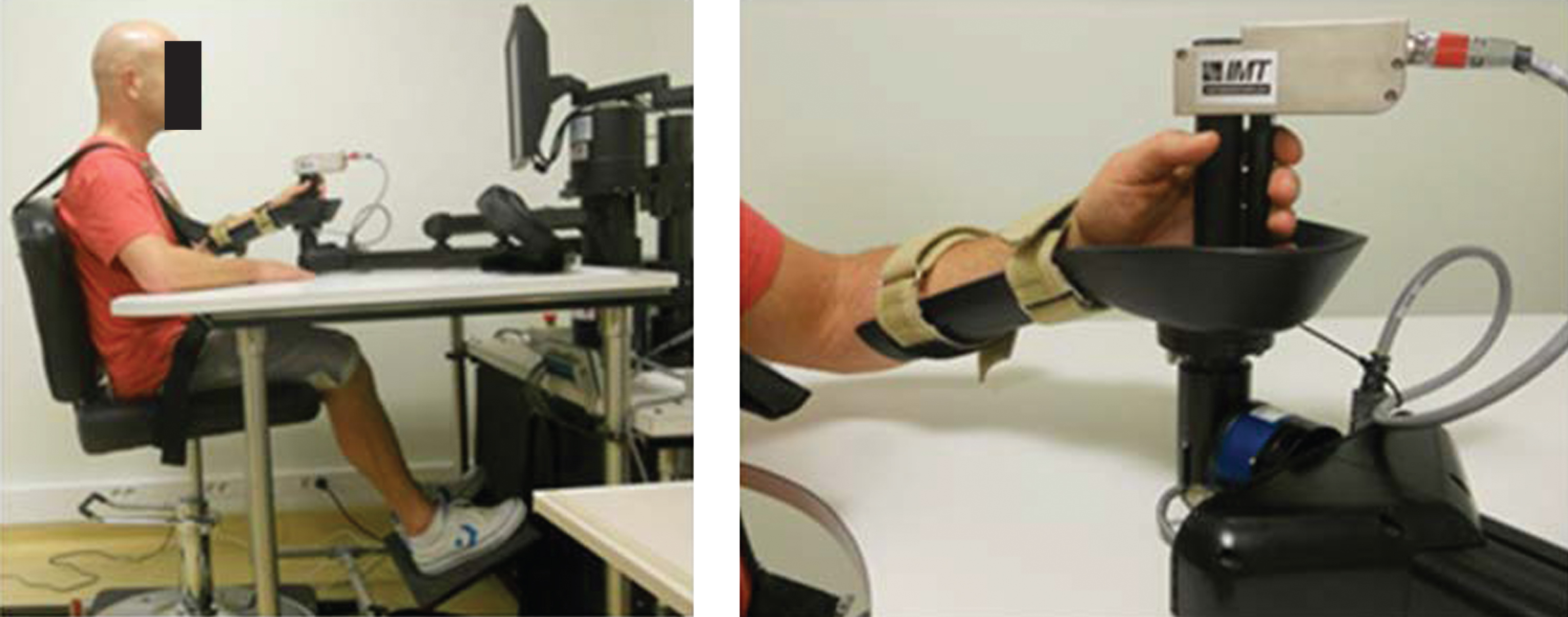
In Motion ARM 2.0 Robot.
During the training sessions, the patients were seated on an adjustable chair with the trunk restrained by a harness to decrease compensatory movements. The paretic forearm was fixed in a support that allowed gravity-compensation. The shoulder was in 45° elevation and the elbow slightly flexed. The wrist was in a neutral position and the fingers were placed around the handle (Figs. 1 and 2).
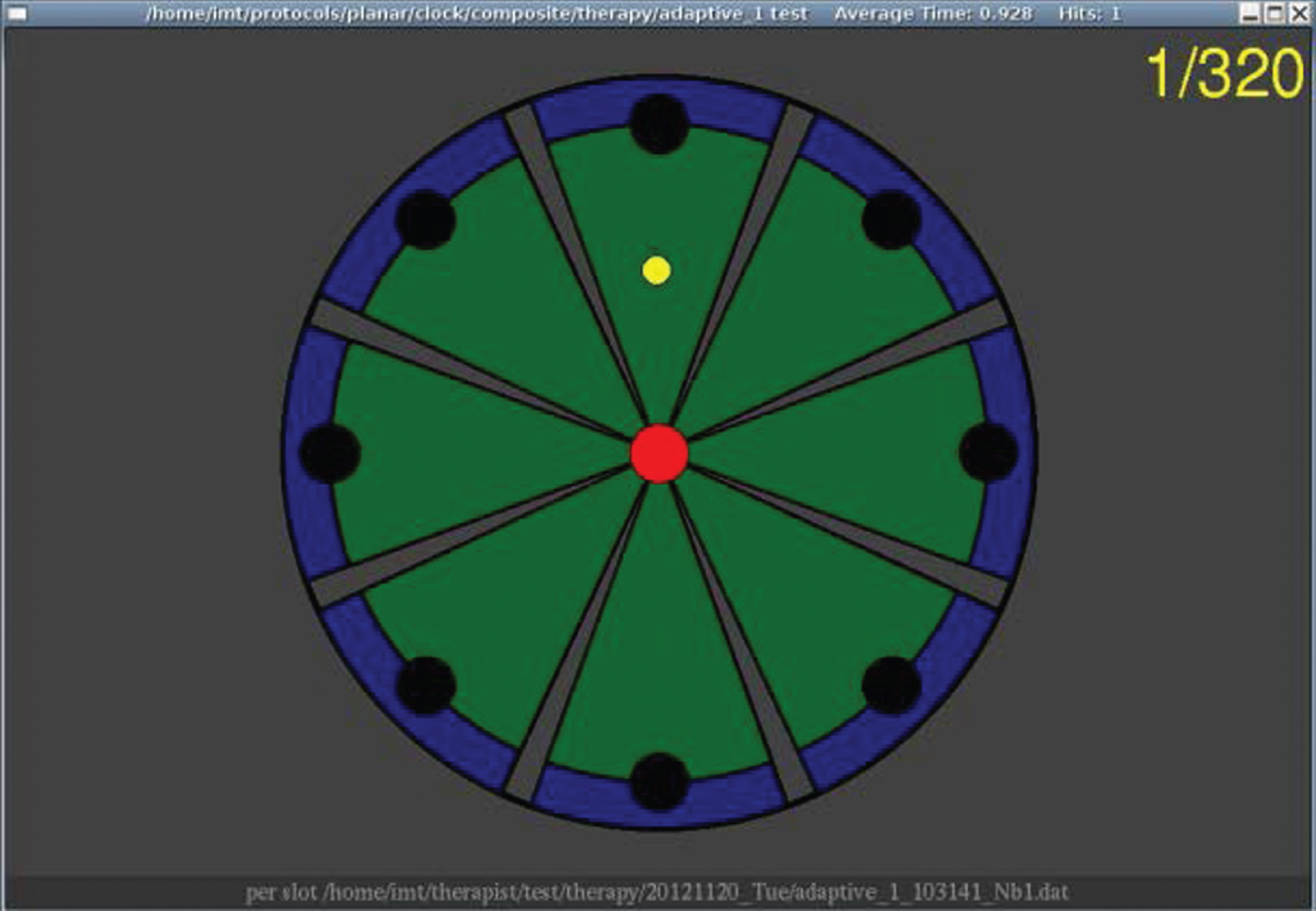
Visual interface of point to point tasks.
The patients performed goal-directed exercises displayed on a monitor in front of them. The reaching tasks consisted of point to point movements towards 8 visual targets displayed in the 8 compass directions (14 cm apart) and presented in a clockwise order. The patients were instructed to perform as many accurate robot-assisted movements as possible in the allocated time. The adaptive training consisted of series of 320 repetitions (4 blocks of 80 movements). Patients were allowed a 1 to 3-minute break after each block and had to perform at least 2 series of 320movements.
All patients also underwent usual care for the upper limb that consisted of one-hour sessions of occupational therapy, 5 days per week. These sessions included various passive and active interventions tailored to the problems and abilities of each patient. They also underwent one- hour daily (5 days a week) sessions of physical therapy based on lower limb rehabilitation (without upper limb therapy) and, if necessary, one hour of speech therapy 3-4 times a week.
Clinical evaluations
All patients underwent a clinical evaluation using the upper extremity portion of the Fugl- Meyerassessment (FMA) scale (Fugl-Meyer, Jääskö,Leyman, Olsson, & Steglind, 1975) before beginning training, but only 13 patients were evaluated at the end of the training. The FMA scale is a well-known, validated clinical scale that measures the ability to move the paretic arm and consists of 33 items related to movements of the shoulder, elbow, wrist and hand, rated on a 3-point ordinal scale (maximum score, 66 points).
Performance measures
The robot recorded the position of the hand during all the movements carried out during the training sessions. Four metrics were then computed to measure motor performance during the reaching tasks (active patient participation + robotic assistance):
The outcome measures recorded during Sessions 1 (S1), S4, S8, S12 and S16 were analyzed. Moreover, the same parameters recorded within the first and the second series of 320 movements of each session analyzed were also analyzed. The values recorded after the 80th movement of each series were analyzed because during the first 80 movements, these parameters are adjusted every 16 movements by the robot, they remain quite stable thereafter.
Robotic assistance parameters
Parameters related to robotic assistance, which provide a quantitative assessment of patient participation were measured:
Statistical analysis
A paired student t-test was used to compare the FMA scores before and after the training. Performance measures and Robotic assistance parameters were compared between the 1st and 2nd series of 320 movements for S1, S4, S8, S12 and S16, using a paired student t-test.
Performance measures and Robotic assistance parameters were compared across sessions (S1, S4, S8, S12 and S16) using a non-parametric Friedman test and a post-hoc analysis was carried out using a Wilcoxon test.
Results
Comparison of parameters measured during series 1 and series 2
There was no difference in Robotic assistance parameters or Performance measures between series 1 and series 2 for any session (Table 2).
Intra session parameters
Intra session parameters
Results are expressed as mean (SD). aSeries1 Vs Series2, p < 0.05.
Robotic assistance parameters: There was a decrease in slottime (p = 0.0035) and initiation (p = 0.045) after S8 and a decrease in stiffness (p = 0.003) and robot power (p = 0.024) after S12 (See Table 3 for details).
Within session parameters
Within session parameters
Results are expressed as mean (SD). aVersus S1, p < 0.05.
The following measures improved after S12: Movement extent, p = 0.008; Straightness, p = 0.038 and Time, p = 0.004. There was no change in Jerk (Table 3).
Clinical scores improved after training. The FMA score increased by at least 9 points at the end of the 16 sessions in 9 patients.
Discussion
This study measured the active participation of patients with severe sub-acute stroke during assist-as-needed upper limb robotic training. Performance parameters and Robotic assistance parameters were measured in order to gain an understanding of the treatment ‘dose’. To our knowledge, this is the first study to evaluate both quantitative and qualitative parameters relating to patients’ motor activity during movement execution, mainly because, without the use of a robotic device, i.e. during conventional rehabilitation, these parameters are very difficult to measure.
The results demonstrated that, despite the large number of movements carried out during each session (at least 640) using an “assist-as-needed” robotic algorithm, the patients’ active participation did not dwindle over the course of the session. Moreover, the robotic assistance decreased from session to session, indicating an increase in active participation over sessions. In parallel, there was no loss of quality or efficiency over the 2 series of movements practiced within each session. Furthermore, kinematic measures of movement efficiency and quality (respectively related to active range of motion and movement accuracy) improved after the 12nd session.
Use of robotic devices to quantify performance and participation
This study highlighted the advantage of robotic devices for the measurement of the amount of motor activity performed, a parameter that can be likened to ‘dose’ for medication. This measurement provides an insight into the ingredient components of movement-based rehabilitation, and follows the recommendations of Page, Schmid, and Harris (2012) to quantify the intensity of physical treatments i.e. “the amount of physical or mental work put forth by the client during a particular movement or series of movements, exercise, or activity during a defined period of time.” A critical and emerging concern raised in the literature on stroke rehabilitation is the need for consensus and homogenization regarding the question of which components of rehabilitative interventions affect motor outcomes in stroke survivors (Lang, Lohse, & Birkenmeier, 2015; Page et al., 2012). A growing body of evidence suggests that the amount of motor activity performed by stroke patients (Cooke et al., 2010; Han et al., 2013; Kwakkel et al., 2004; Lincoln et al., 1999; Lohse et al., 2014) is the primary factor that influences motor outcomes; however, little is known regarding the constitutive ingredients of the motor activity. Most studies in the field of stroke rehabilitation measure the amount of rehabilitation in terms of time spent carrying out the intervention (without considering active therapy time), although some have counted the number of repetitions performed during therapy sessions (Lang et al., 2009). Robot-assisted upper limb training provides large numbers of movement repetitions in comparison with usual therapies (Kimberley et al., 2010; Lang et al., 2009), and can keep track of the numbers of repetitions. An added value of a robotic paradigm is the precise control of the number of movements carried out. Several studies have shown (Hsieh et al., 2012; Lo et al., 2010; Volpe et al., 2000) that stroke patients perform hundreds of movements during robotic therapy, a magnitude that has been demonstrated to effectively induce neuroplastic changes in animal models, and thus is likely to also induce such changes in humans (Kleim et al., 2002; Krakauer, Carmichael, Corbett, & Wittenberg, 2012). Although there is evidence that delivering highly repetitive usual care- based interventions is feasible in the acute stages of severe stroke (Waddell, Birkenmeier, Moore,Hornby, & Lang, 2014), fatigue and pain were reported as limiting factors by patients.
However, beyond the need to provide high numbers of repetitions, rehabilitation techniques must promote engagement (Blank, French, Pehlivan, & O’Malley, 2014). The “effort” generated by patients during the training is crucial. It has been shown to be an active ingredient of the physical treatment, approaching what most clinicians used to name intensity. Studies of robot-assisted gait training have demonstrated that a critical determinant of training effectiveness is level of participation. Such rehabilitation is more effective when the user actively participates in the movement, and the use of full, passive guidance has a negative impact on recovery in stroke patients (Collantes, Asin, Moreno, & Pons, 2012; Krishnan, Kotsapouikis, et al., 2013; Pennycott, Wyss, Vallery, Klamroth-Marganska, & Riener, 2012).
The present study showed that the assist-as-needed robotic algorithm did not reduce the patient’s level of active participation. Thus, the patients’ engagement was maintained despite the large number of movement repetitions. This could be attributed to the fact that the robot only provides the necessary assistance to complete the movements and moreover, it challenges the patient by delivering exercises tailored to his/her capacity, increasing engagement (Shirzad & Van der Loos, 2016). The visual biofeedback provided might have enhanced the motivation and the engagement of patients in the exercises (Rosati et al., 2011; Secoli, Milot, Rosati, & Reinkensmeyer, 2011), since it provided quantitative and qualitative information on actual performance, as well as comparisons with previous sessions. It is also likely that the ‘recreational’ nature of the treatment distracts from any fatigue and pain and motivates the patient to strive to improve his/her performance (Malloy & Milling, 2010).
Analysis of the change over time of assistance parameters and Performance measures showed that velocity related measures improved beforemovement accuracy (Stiffness and Straightness). These has previously been found by our team (Duret, Courtial, et al., 2015; Duret & Hutin, 2013) and others (Colombo et al., 2008) and gives valuable information regarding the process of motor recovery and/or motor learning after stroke. Indeed, these results suggest that two months after stroke, motor performance improvement follows a speed/accuracy trade-off pattern, a feature that characterizes motor skill learning (Lefebvre et al., 2015).
Is movement quality important?
It is well known that large numbers of active movement are crucial to stimulate neural motor networks (Carey et al., 2007; Levy, Nichols, Schmalbrock, Keller, & Chakeres, 2001; Takeuchi & Izumi, 2013). However, it is not really known if certain parameters relating to motor activity enhance the stimulation of neural networks. Although some researchers have suggested that activity-dependent plasticity requires the practice of close-to-normal movements (Daly & Ruff, 2007; Nudo, Wise, SiFuentes, & Milliken, 1996), there has been little consideration regarding the specific kinetic and kinematic parameters that rehabilitation should emphasize. However, there have been advances in the understanding of mechanisms underlying motor deficits after stroke during the last decade. Cirstea, Mitnitski, Feldman, & Levin, (2003) showed that the motor planning of reaching movements may be impaired and, more recently, Rizzo et al., (2015) found two movement-planning codes, one representing the direction of a desired movement (vector code) and the other one for the desired endpoint (target code). In addition, Howard, Ingram, &Wolpert (2011) have shown that rhythmic and discrete movements, two components of the motor repertoire (Hogan & Sternad, 2012) are controlled by distinct neural pathways. However, knowledge of the neural substrates of motor skill learning and neuromechanical principles underlying motor learning process (Ting et al., 2015) is still in its infancy.
If we compare movement therapy to pharmaceutical agents, it can be assumed that the qualitative features (motion kinetics and kinematics) of input signals might be of relevance to drive motor recovery and skill learning. Sensor-based interventions, such as robotic therapy, enable the biomechanical assessment of the movements carried out by the patients, providing insight into the kinematics and kinetics of motor input. Our results indicated that the algorithm implementing the robotic behavior (assist-as-needed) both actively assists and challenges patients, stimulating the quality of movement over time during within-session practice, as well as producing an incremental improvement in kinematics during the training. Although the effect of different qualitative features of movement on recovery post stroke is not known, it is likely that controlling the motor input or providing patients with feedback on their motor performance might be helpful in the design of more effective motor learning paradigms. Cirstea & Levin, (2007) showed that skill reacquisition could be augmented by feedback of knowledge of performance (attention directed on movement kinematics) more than knowledge of results in which the goal is to achieve the movement, regardless of the strategy. With regard to interventions based on motion kinematics, much knowledge can be gained from studies that have evaluated the effects of error augmentation-based algorithms that constrain the patient to actively control the end-effector displacement as accurately as possible to prevent any destabilization (Tropea et al., 2013), or to correct trajectory deviations induced by the robot (Abdollahi et al., 2014; Patton, Stoykov, Kovic, & Mussa-Ivaldi, 2006).
Conflict of interest
The authors have no conflict of interest to declare.