
Abstract
BACKGROUND:
Robotic-assisted gait training (RAGT) has been proposed as a novel, promising intervention paradigm to improve gait function in subacute or chronic stroke neurorehabilitation. However, the benefits of RAGT combined with conventional physical therapy for gait recovery in patients with subacute and chronic hemiparetic stroke remain unclear.
OBJECTIVES:
The aim of the present study was to compare the effect of RAGT combine with conventional physical therapy on hip joint kinetics, kinematics, and clinical function characteristics between subacute and chronic hemiparetic stroke.
METHODS:
Seventeen patients with hemiparetic stroke (nine subacute and eight chronic patients) performed progressive RAGT (session 1, 40 min) combined with conventional physical therapy (session 1, 40 min) 5 days per week, for an average of 86 sessions over 8 weeks. The clinical outcomes included the Functional Ambulation Category (FAC), modified Rankin scale (mRS), Korean version of the modified Barthel index (K-MBI), and modified Ashworth scale, in addition to hip joint kinetics and kinematics before and after intervention.
RESULTS:
The mean change in active torque, resistive torque, and stiffness in the paretic hip joint did not differ significantly between the two groups. However, Cohen’s effect size suggested a moderate difference between the groups in the hip flexion phase (d = 0.58, d = 0.70, and d = 0.70). The mean change in maximal hip flexion kinematics in the chronic group was significantly greater than that in the subacute group (p = 0.04, d = –0.70). The mean change in the clinical function test results between the groups was not statistically significant. However, both groups showed significantly improved FAC, mRS, and K-MBI scores.
CONCLUSIONS:
RAGT combine with conventional physical therapy may be useful when selecting therapeutic interventions to improve the active torque, resistive torque, and stiffness in the paretic hip flexion phase in patients with chronic hemiparetic stroke who reached a plateau in the maximum locomotor recovery after conventional locomotor training.
Introduction
Hip flexion stiffness is an important neuromechanical marker that contributes to an asymmetrical hemiplegic hip flexion gait pattern in spastic hemiparetic stroke (Balaban & Tok, 2014; Woolley, 2001). Hip flexion stiffness results from hypertonicity of the hip flexors such as rectus femoris (Hutin et al., 2010; Robertson et al., 2009; Stoquart et al., 2008). It has been postulated that hypertonicity of the hip flexors is associated with cortical disinhibition in the affected hemisphere in patients with stroke and is correlated with poor motor outcomes (Dobkin, 2005; Hyngstrom et al., 2010; Sheean, 2002; Sheean & McGuire, 2009). Moreover, such increased hypertonicity and associated stiffness of the hip flexors can reciprocally inhibit gluteus maximus activity and restrict hip extension movement from the terminal stance to the pre-swing phases (Balaban & Tok, 2014; Finley et al., 2008). The lack of hip extension movement will cause hip joint instability during the stance phase and increase the risk of falls in hemiparetic stroke (Weerdesteyn et al., 2008). During the pre-swing phase, the forward momentum is also compromised, decreasing the symmetrical stride or step length and velocity (Balasubramanian et al., 2007). To compensate for this deficiency in hip extension movement control, a hip hiking or circumduction gait becomes evident with an overutilization of the quadratus lumborum, and causes an inefficient energy consumption (Balaban & Tok, 2014; Woolley, 2001).
Contemporary locomotor rehabilitation techniques include treadmill gait training, partial weight support gait training, and robotic-assisted gait training (RAGT). However, their outcomes are inconclusive (Duncan et al., 2011; Fisher et al., 2011). Among these techniques, RAGT system is engineered to systematically provide an accurate kinematic and kinetic locomotor pattern for patients with abnormal gait patterns due to neurological impairments, such as spinal cord injury, stroke, traumatic brain injury, or cerebral palsy and other related gait impairments (Jung, Lee, You, & Lee, 2009; Kim, Shin, Joa, Shin, Lee, & You, 2013; Kim, Yang, Park, Kim, Park, You, & Shin 2015). RAGT has recently gained widespread acceptance among neurorehabilitation clinicians because it provides the advantages of an intensive, repetitive, resistive, fun, and task-specific gait training paradigm with comparable results to conventional stroke rehabilitation (Kim et al., 2015). A previous study has reported that a 30-min RAGT session significantly decreased knee flexion stiffness associated with hamstring spasticity and improved knee extension torques during the terminal swing phase in hemiparetic stroke (Kim et al., 2013). A systematic review of RAGT studies supported that locomotor retraining with robotic-guided assistance is beneficial for enhancing locomotor function in individuals with hemiparetic stroke (Mehrholz & Pohl, 2012). In particular, early mobilization using RAGT is recommended to prevent the potential development of connective tissue contracture because of prolonged immobilization and spasticity. There is accumulating clinical evidence supporting the effects of robotic therapy administered during the subacute phase of post-stroke onset (Morone, Bragoni, Iosa, De Angelis Venturiero, Coiro, & Paolucci, 2011; Morone et al., 2012). However, the effects of RAGT were not compared between patients with subacute and chronic stroke. Furthermore, the therapeutic effects of RAGT on hip stiffness and kinematics in hemiparetic stroke remain unclear.
Therefore, the objective of this study was to compare the effect of RAGT combined with conventional physical therapy on hip joint stiffness, kinematics, and clinical function tests between patients with subacute and chronic hemiparetic stroke. We hypothesized that RAGT combined with conventional physical therapy would have different effects on hip joint stiffness, kinematics, and clinical function outcome measures in these different patients.
Materials and methods
Materials
The Walkbot (P&S Mechanics, Seoul, South Korea) is a state-of-the-art robotic-assisted system equipped with various control strategies, including passive (trajectory tracking), active-assistive, and active modes that modify control parameters based on ongoing participant performance and real-time visual biofeedback for torque and stiffness, in addition to kinematics for the hip, knee and ankle joints during gait training. Unlike other robotic-assisted systems, the Walkbot system has an independent ankle actuator in addition to hip and knee actuators for foot clearance, which naturally simulate the optimal gait trajectory (Jung et al., 2009; Lee et al., 2016). The motorized treadmill speed and torque (assistance and resistance) can be adjusted to provide the user with safe and challenging locomotor retraining modes as the training progresses.
Participants
Patients with a verified diagnosis of stroke with lower extremity hemiparesis via computed tomography or magnetic resonance imaging were screened for eligibility at a major university medical center. The inclusion criteria were as follows: (1) first-ever stroke or prior stroke with no residual deficits affecting ambulation; (2) supratentorial lesions; (3) age between 18 and 80 years; (4) significant ambulation deficits (functional ambulation category [FAC] <3) (Holden et al., 1986); (5) ability to follow a three-step command; and (6) ability to perform rehabilitation management at least 5 days per week. The exclusion criteria were as follows: (1) severe spasticity (modified Ashworth scale [MAS] >2) in the affected lower-extremity with a range of motion <80% (Kim et al., 2015; Morone et al., 2011); (2) uncontrolled high blood pressure; (3) severe visual and cognitive impairments; (4) musculoskeletal or integumentary system impairments (bedsores around the loading area of the suspension belt); (5) previous robotic interventions for ambulation training; and (6) body mass >135 kg or height <150 cm. After screening, the enrolled patients were evaluated for baseline characteristics and stratified in according to the time from stroke. The patients with an elapsed time from stroke of 4 weeks to 6 months were allocated to the subacute group, while the patients with an elapsed time of >6 months were allocated to the chronic group (Adams et al., 1994) (Fig. 1).
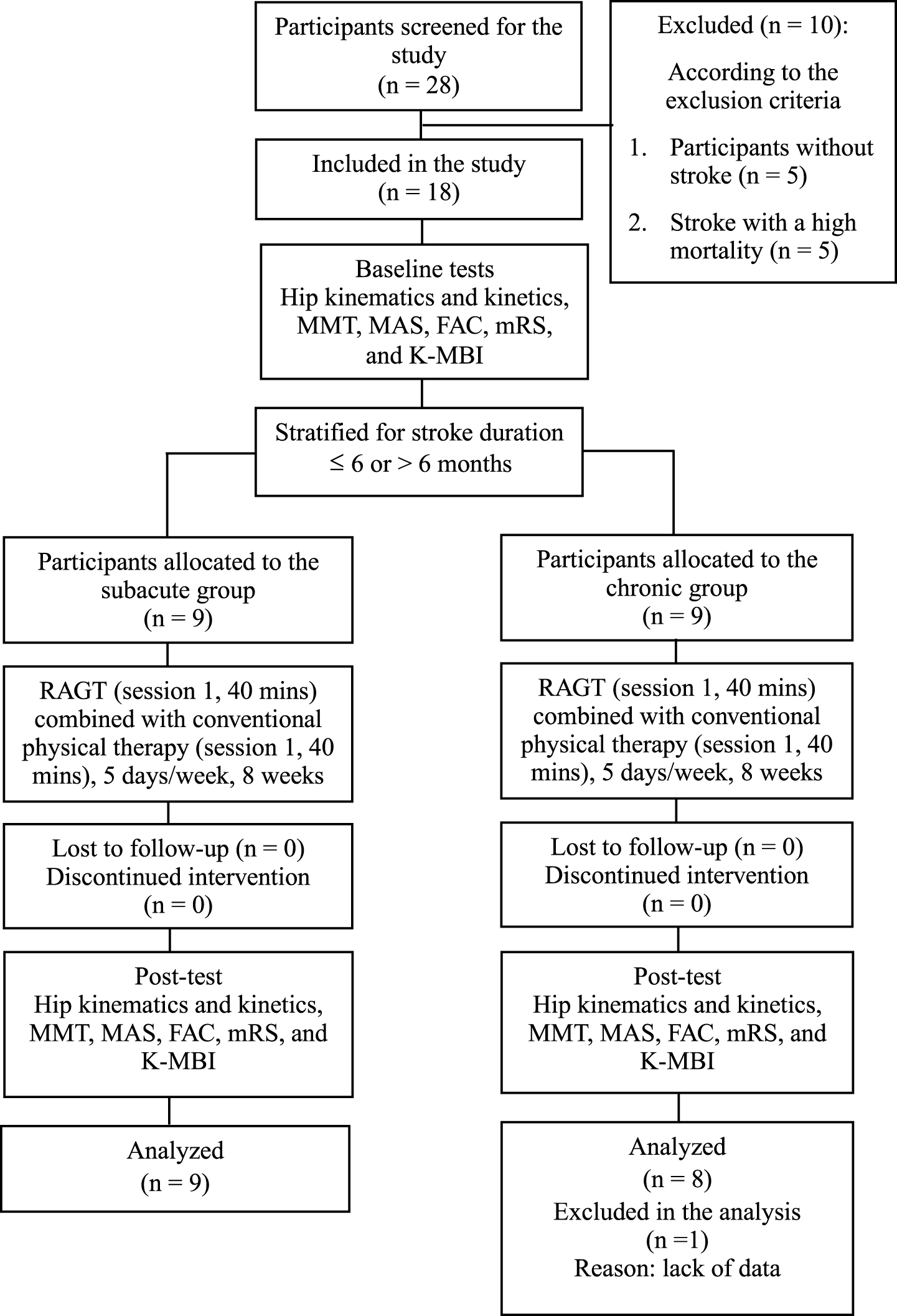
Flow diagram of the study. MMT: manual muscle testing; MAS: modified Ashworth scale; FAC: functional ambulation category; mRS: modified Rankin scale; K-MBI: Korean version of the modified Barthel index.
Except for the months from stroke to RAGT, no significant differences in baseline characteristics were observed between the two groups (Table 1).
Summary of the participants’ characteristics (n = 17)a
aMean (SD) or numbers (%). RAGT, robotic-assisted gait training. *p < 0.05 by Mann-Whitney U test for continuous variables and Fisher’s exact test for categorical variables between the two groups.
The experimental study protocol was approved by the institutional review board of the national university hospital. All participants provided informed consent and performed progressive RAGT (session 1, 40 min) combined with conventional physical therapy (session 1, 40 min) 5 days per week for an average of 86 sessions over 8 weeks. Conventional physical therapy included early mobilization, balance, and transfer during sit-to-stand, and gradual progression to overground gait training with or without assistive devices for 40 min (Veerbeek et al., 2014). In addition to conventional physical therapy, RAGT was added for another 40 min. Anthropometric data (height, weight, foot size, thigh length, shank length, and ankle height) were entered into the computer and the robotic system adjusted itself to these data. The exoskeleton legs lengthened or shortened based on the participant’s leg length and system automatically set the spatiotemporal values based on these data. The spatiotemporal (stride length, gait velocity, and gait cycle) values were changed if necessary before RAGT. Each participant wore a suspension harness connected to a counterweight system aligned with the exoskeletal system’s actuators (hip, knee, and ankle joints), and secured with elastic straps. Depending on the patient’s clinical conditions (e.g., pain, muscle weakness, spasticity, tolerance, fatigue, or endurance), approximately 40–60% (adjustable range, 0–100%) of the total body weight was sustained at the first session and then gradually decreased in 5–10% increments per session. Stride length was initially adjusted at 1.0–1.6 m/cycle and walking velocity started at 1.00–1.20 km/h and gradually increased by 0.1 km/h every 5 min as tolerated to 2.40–2.60 km/h (maximally adjustable to 3.00 km/h) (Kim et al., 2015).
The RAGT system was set to an assist-training strategy, which effectively controls the amount of force the system provides. If the participant’s walking ability improved to the level at which they could adjust the magnitude of their leg movements to reduce kinematic trajectory errors, they could alter the kinematic trajectory using active torque. At this time, the force was reduced in the robotic system, which offers maximal assistance at 100% force for the more affected leg. At 0% force, the system only compensates for the weight, resistance, and inertia in accomplishing symmetrical, optimal gait patterns. A monitor located in front of the participants provided them with biofeedback of their gait kinematics (joint angles of the lower limb and vertical displacement of the center of mass), and torques of the hip, knee, and ankle joints to reduce error signals in the kinematic trajectory. During RAGT, the participants were provided with constant verbal encouragement using the knowledge of performance. Furthermore, a subcortical locomotor relearning paradigm was used as the participants kicked the ball automatically presented rather than consciously making an accurate step. Heart rate was monitored to maintain it below 80% of the age-appropriate level and blood pressure was checked in real-time during RAGT. Finally, inter-training rest was provided if necessary.
Outcome measures
Hip joint kinematic and stiffness measurements
The robotic system-STIFF measurement was used to examine hip joint stiffness associated with RAGT. The graphical output data were recorded at a maximal sampling rate of 72 Hz (gait cycle varies with the individual walking velocity; frequency range 28–72 Hz in the 1.00–2.60 km/h) with a moving averaging filter. The stiffness, k, of a hip joint segment measures the resistance offered by an elastic body segment to deformation. For a hip joint segment with a single degree of freedom (e.g., stretching or compression of a hip segment), the resistive stiffness is defined as follows:
where F is the resistive force acting on the hip joint and θ is the angular displacement produced by the force acting on the hip joint. The hip joint torque data were obtained by the servomotors that modulate the bilateral hip, knee, and ankle joint kinematics and kinetics using encoders. Each encoder determines the joint angle, angular velocity, and acceleration data, which are then used to compute for the moment or torque associated with the active and resistive forces of the body segment acting on the hip joint as the participant walks. Active torque was defined as the moment that rotates with a certain hip joint angular displacement in the same direction, whereas resistive torque was defined as the moment that rotates in the opposite direction. Hence, greater active torque represents greater voluntary strength recovery in the paretic limb during gait, while greater resistive torque represents greater stiffness, which constrains voluntary hip joint movement. Peak angular displacement and averaged force values were obtained from 10 gait cycles of each stable state that was longer than 5 min. These data were divided into the movement directions (hip flexion/extension). Knowing the thigh lever arm acting at the robot system, the recorded force data can be transformed into hip joint torques that act between the robotic system and participant’s leg. Based on the hip joint angular displacement and resistive torque data, the hip joint stiffness was calculated from the slope of the linear regression in the torque-angular displacement curve during the gait cycle (Padua et al., 2006). Hip joint torque and stiffness were performed offline using the Matlab platform ver. 9.0.0 (MathWorks, Natick, MA, USA).
Clinical function tests
Standardized clinical tests included FAC, mRS, K-MBI, and MAS, which were performed before and after the intervention. The FAC is designed to examine the levels of assistance needed for a 15-m walk with a scoring scale ranging from 0 (non-ambulatory) to 5 (normal) (Mehrholz et al., 2007). The mRS assesses the severity of disability associated with ambulation in patients with hemiparetic stroke with a grading score ranging from 0 (no symptoms at all) to 6 (death) (Banks & Marotta, 2007). The K-MBI is a widely-used assessment tool that measures the levels of assistance or dependence in performing functional activities of daily living with a scoring scale from 1 (total dependent) to 5 (independent) (Jung, Park, Shin, Kang, Pyun, Paik & Han, 2007). The lower leg MAS measures the sum of the scores at the knee and ankle flexors to estimate abnormal muscle tone in the lower extremity with a grading scale of 0 (no increase in muscle tone) to 4 (rigidity) (Morone et al., 2011), and scores of 1+, 2, 3, and 4 were changed to 2, 3, 4, and 5 for statistical analysis, respectively (Lim et al., 2016). The reliability and validity of the FAC, mRS, K-MBI, and MAS are well established (Banks & Marotta, 2007; Blackburn et al., 2002; Jung et al., 2007).
Statistical analysis
All continuous variables were analyzed to ensure the assumption of a normal distribution using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to evaluate group differences in the baseline characteristics and hip kinematics and kinetics. Fisher’s exact test for categorical variables was used to evaluate group differences in baseline characteristics. In addition, the effect size (Cohen’s d) was used to calculate the magnitude of the differences and practical significance in these variables between the two groups. The Mann-Whitney U test values were transformed to effect sizes for the non-parametric variables via the normal distribution approximation. A statistical package was used to acquire appropriate z values in addition to the U values to calculate the Eta squared value (η∧2 = z2/N) (Fritz et al., 2012). The strength of the effect sizes was interpreted as small (d < 0.4), moderate (0.4≤d < 0.8), or large (d ≥ 0.8) (Cohen, 1988). The pre- and post- intervention changes within each group were analyzed using the Wilcoxon signed rank test. SPSS for Windows (version 21.0, Chicago, IL, USA) was used with statistical significance set at p < 0.05.
Results
Kinetic data
The mean change in active torque, resistive torque, and stiffness in the paretic hip joint did not differ significantly between the two groups (Table 2). However, Cohen’s effect size suggested a moderate difference between the groups in the hip flexion phase (d = 0.58, d = 0.70, and d = 0.70, respectively) (Table 2).
Change in the paretic hip joint kinematics and kinetics at 8 weeks (n = 17)a
Change in the paretic hip joint kinematics and kinetics at 8 weeks (n = 17)a
aMean (SD). bEffect sizes are based on the standard deviation of the mean change in the chronic group (a negative effect size denotes an increase in the maximal angle and active torque in the chronic group and a positive effect size in resistive torque and stiffness indicates an increase in the mean change in the chronic group). *Wilcoxon signed rank test for the within-group analysis, p < 0.05. †Mann-Whitney U test between the two groups, p < 0.05
The mean change in maximal paretic hip flexion in the chronic group was significantly greater than that in the subacute group (p = 0.04, d = –0.70) (Table 2). Although the mean change in maximal paretic hip extension in the chronic group was greater than that in the subacute group, the difference did not reach statistical significance (p = 0.29). However, the effect size statistics indicated a moderate difference in maximal extension of the paretic hip joint between the groups (d = –0.68) (Table 2).
Clinical function tests
The mean change in clinical function test results between the groups was not statistically significant. However, both groups showed significantly improved FAC, mRS, and K-MBI scores (Table 3).
Changes in clinical outcomes at 8 weeks (n = 17)a
Changes in clinical outcomes at 8 weeks (n = 17)a
aMean (SD). MMT, manual muscle testing; MAS, modified Ashworth scale; FAC, functional ambulation category; mRS, modified Rankin scale; K-MBI, Korean version of the modified Barthel index. bIn this scale, a reduction in the score indicates an improvement in the condition being evaluated. *Wilcoxon signed rank test for the within-group analysis, p < 0.05.
This study is the first clinical trial to demonstrate the effects of RAGT combined with conventional physical therapy on hip joint kinematics, kinetics, and clinical function characteristics between patients with subacute and chronic hemiparetic stroke. Most importantly, differences in the maximal flexion angular displacement of the paretic hip joint were observed between the subacute and chronic groups (p = 0.04). Although our findings showed no statistically significant differences in active torque, resistive torque, and stiffness in the paretic hip joint tested using the Mann-Whitney U test, the effect size (Cohen’s d) indicated a practical significance for these variables between the groups. In fact, a moderate effect size demonstrated a practical significance in the mean differences in active torque (d = 0.58), resistive torque (d = 0.70), and stiffness (d = 0.70) between the groups in the hip flexion phase.
With respect to hip joint kinetics, the patients in the chronic group demonstrated greater improvements in hip resistive torque (d = 0.70) and stiffness (d = 0.70) in the paretic hip flexion phase than those in the subacute group. An increased active torque as well as maximal extension angular displacement resulting in a decreased resistive torque (elongated hip flexor) and subsequent changes in the length-tension curve are thus conceivable, which may decrease stiffness in the paretic hip flexion phase in the chronic group. Neuromechanically, intensive, repetitive, symmetrical, and active-assisted RAGT may have contributed to neural plasticity and synaptogenic efficacy or to the unmasking of the underutilized neural circuits or utilization of the alternative neuronal pathways (e.g., ipsilateral corticospinal tracts, supplementary motor areas and premotor cortex areas) implicated in locomotor control (Diserens et al., 2007; Shimodozono et al., 2013). In addition to the neuronal component, non-neural adaptive changes, such as changes in the stiffness of the muscle fibers, collagen tissues, and tendons, and mechanical muscle-fiber property changes may contribute to the mechanical resistance to passive movement (Dietz et al., 1991).
Although the mean change in active torque in hip flexion was greater in the subacute group (1.05 Nm) than in the chronic group (0.69 Nm), this mean change did not improve the hip flexion kinematics in the subacute group. Improvements in active torque in the subacute group were insufficient to counterbalance the strong resistive torque induced by the hip extensors, which consequently did not to improve the hip flexion kinematics in this group. It is conceivable that an antagonist (hip extensor) is not inhibited reflexively when its agonist (hip flexor) is activated. Physiologically, this is an important finding because it explains the result of neuroreflexive changes, which may exhibit delayed activation in hip flexion. Given that the greatest motor recovery occurs in the first 3 months after stroke, we believe that the subacute group (mean onset duration <2 months) was still undergoing neurologic recovery. For these reasons, evidence of the beneficial effect of RAGT combined with conventional physical therapy has been found in chronic stroke in motor control, strength, mobility, and functional gait ability (Bae et al., 2014; Liepert et al., 2000; Teixeira-Salmela et al., 2001).
Contrary to the greater amount of hip flexion improvement, we did not find group differences in the kinematics and kinetics in the hip extension phase. One explanation for the lack of hip extension improvements may be related to the fact that patients after stroke could not generate voluntary torque without generating joint torques in other directions and joints (Dewald & Beer, 2001). To minimize the asymmetrical gait pattern, the patients were fitted with hip, knee, and ankle exoskeletons of revolute joints so that corrective alignment could be provided via enriched proprioceptive stimuli within the robotic system. Therefore, it might be difficult to generate voluntary hip extension torque selectively without employing abnormal synergy torque in other joints. This scenario is supported by the study by Sakuma et al. (2014) who reported that the ability to generated torque using abnormal synergy may help in the locomotor improvement of patients with stroke.
Improvement in active torque of the hip flexors may be a result of the reciprocal inhibition of the resistive torque of the hip extensors, which in turn failed to induce statistically significant active torque of the hip extensors from the terminal stance to the pre-swing phases. Ideally, the hypertonic hip flexor muscles are deactivated while reciprocally facilitating the hip extensors, thereby reducing excessive hip flexion stiffness. Our finding of greater hip flexion kinematics, which resulted from the decreased resistive torque of the hip flexors, is in contrast to the result of a previous study by Kim et al. (2013). The authors reported improved knee flexion stiffness and associated knee extension kinematics instead of knee flexion kinematics. Similarly, Schmartz et al. (2011) also reported a significant reduction of resistive hip flexion stiffness for hip extension movements during passive leg movements in children with cerebral palsy after a single session of RAGT. Reciprocal-improved stiffness control results in the proper advancement of the reciprocal locomotor movement pattern and increased stride length and velocity of the paretic limb in spastic hemiparetic stroke (Macko, 2013).
Clinically, these neuromechanical improvements were associated with functional ambulation and independent motor performance in daily activities of living. Although the mean change in the clinical function test results between the groups was not statistically significant, practical significance was found in the manual muscle testing (d = 1.02) and MAS (d = 0.49) scores. Furthermore, both groups showed significantly improved FAC, mRS, and K-MBI scores, suggesting that RAGT combined with conventional physical therapy caused improvements in ambulation, level of assistance during ambulation, and daily activity function. These findings are consistent with those of previous studies, which reported positive clinical outcomes in the functional ambulation measures for individuals with hemiparetic stroke and spinal cord injury as well as children with cerebral palsy (Patritti et al., 2010; Schwartz et al., 2009; Schwartz et al., 2011). In the present study, increased active torque and decreased resistive stiffness were not consistent with clinical spasticity measurement, which is not thought to quantify subtle changes in muscle tone objectively due to its controversial intra- and inter-rater reliability (Blackburn et al., 2002; Ghotbi et al., 2011). Conversely, the robotic system-STIFF measurement is safe and sensitive enough to record such minute changes in reflex-mediated stiffness or passive movement because it utilizes a low threshold of torque sensors for resistive stiffness (Jung et al., 2009).
Several limitations in the present study should be considered in future research endeavors. First, the small sample size may explain the lack of statistically significant differences between the two groups. Further studies with larger numbers of patients are needed. Second, the concurrent measurement of muscle activity using electromyography may help to ascertain different confounding attributes that contribute to overall hip joint stiffness. Third, it is difficult to generalize our results to infratentorial lesions since the participants had lesions in the supratentorial region of the brain.
Conclusion
RAGT combined with conventional physical therapy is a promising locomotor retraining paradigm for patients with chronic hemiparetic stroke who reach a plateau in maximum locomotor recovery after conventional neurorehabilitation, which is conducive to improvements in hip active torque, resistive torque, and stiffness of the hip flexion phase. In addition, RAGT combined with conventional physical therapy is an important additional treatment for improving walking ability and daily activities in patients with hemiparetic stroke.
Conflict of interest
No conflicts of interest have been reported by the authors or by any individual in control of the content of this manuscript.
Funding
This research received financial and administrative supports from the Brain Korea 21 PLUS Project (grant no. 2016-51-0009) and the Basic Science Research Program (grant no. 2017-51-0187) sponsored by the Korean Research Foundation for the Department of Physical Therapy in Graduate School, Yonsei University. This manuscript has been submitted solely to this journal and has not been published, or submitted elsewhere.
Footnotes
Acknowledgments
We thank Kyung-hwan Lee for technical support. This research received financial and administrative supports from the “Brain Korea 21 PLUS Project (grant no. 2016-51-0009) and the Basic Science Research Program (grant no. 2017-51-0187)” sponsored by the Korean Research Foundation for the Department of Physical Therapy in Graduate School, Yonsei University.