
Abstract
BACKGROUND:
Pusher behavior (PB) is a posture disorder due to a subjective bias in verticality perception. However, muscle activity characteristics in this disorder and the effective treatments are not known.
OBJECTIVE:
To investigate electromyographic (EMG) activity and the effect of electrical stimulation (ES) in PB.
METHODS:
Two PB patients were enrolled. The EMG activity was measured over the upper and lower limb muscles on the non-paretic side, and over the trunk muscles on both sides during sitting. We used a modified ABA single-case design consisting of consecutive baseline, intervention, and follow-up, each phase lasting 2 d. During the intervention, together with conventional treatment, the patient received ES for 5 min/d on the muscle antagonist to the muscle where excessive activity was observed. PB was assessed before and after each phase using the scale for contraversive pushing and the Burke lateropulsion scale. Truncal balance was evaluated using the trunk control test.
RESULTS:
In both patients, electromyography of the non-paretic triceps brachii muscle revealed excessive activity. To inhibit the excessive activity, ES was applied to the non-paretic biceps muscle. All scores improved after the intervention and follow-up phases.
CONCLUSION:
ES based on EMG activity is therapeutic for PB.
Introduction
Some stroke patients exhibit a symptom called pusher behavior (PB). This behavior is a unique sign in which the patient collapses toward the weak side and strongly resists passive attempts to return him or her to an upright position.
With respect to the processing mechanism of PB, Karnath, Ferber & Dichgans (2000) have reported the verticality perception disorder involving some direction and degree of deviation of the vertical axis of the body from true vertical as well as uncertainty (and thus instability) in the patient’s verticality. Under the assumption of a verticality perception disorder, treatment strategies for PB have focused on the visual, somatosensory, and vestibular sensory organs that support a sense of verticality.
However, the authors have previously shown that prone-position therapy immediately and significantly improves acute-phase and subacute-phase PB (Fujino et al., 2016). While the mechanism of prone-position therapy is unknown, the fact that this therapy improves PB suggests that PB is not only a disorder of perception of verticality, but also partly a pathology of motor output and adjustment. However, currently quantitative assessment of PB remains a symptomatologic analysis focusing on factors such as the degree of resistance to correction. A qualitative analysis with a focus on the motor aspects of PB is lacking. Therefore, this study investigated muscular activity in PB patients maintaining a sitting position and the effect of an electrical stimulation (ES) treatment guided by the observed pattern of electromyographic (EMG) activity.
Participants
We enrolled two PB patients who had been diagnosed with cardiogenic cerebral embolism in the right middle cerebral artery area (Fig. 1). Both patients also suffered from motor paralysis, sensory loss, and unilateral spatial neglect (Table 1). Both patients showed severe PB as shown in Table 2. The patients received an explanation about the purpose of the study and provided their consent in writing.
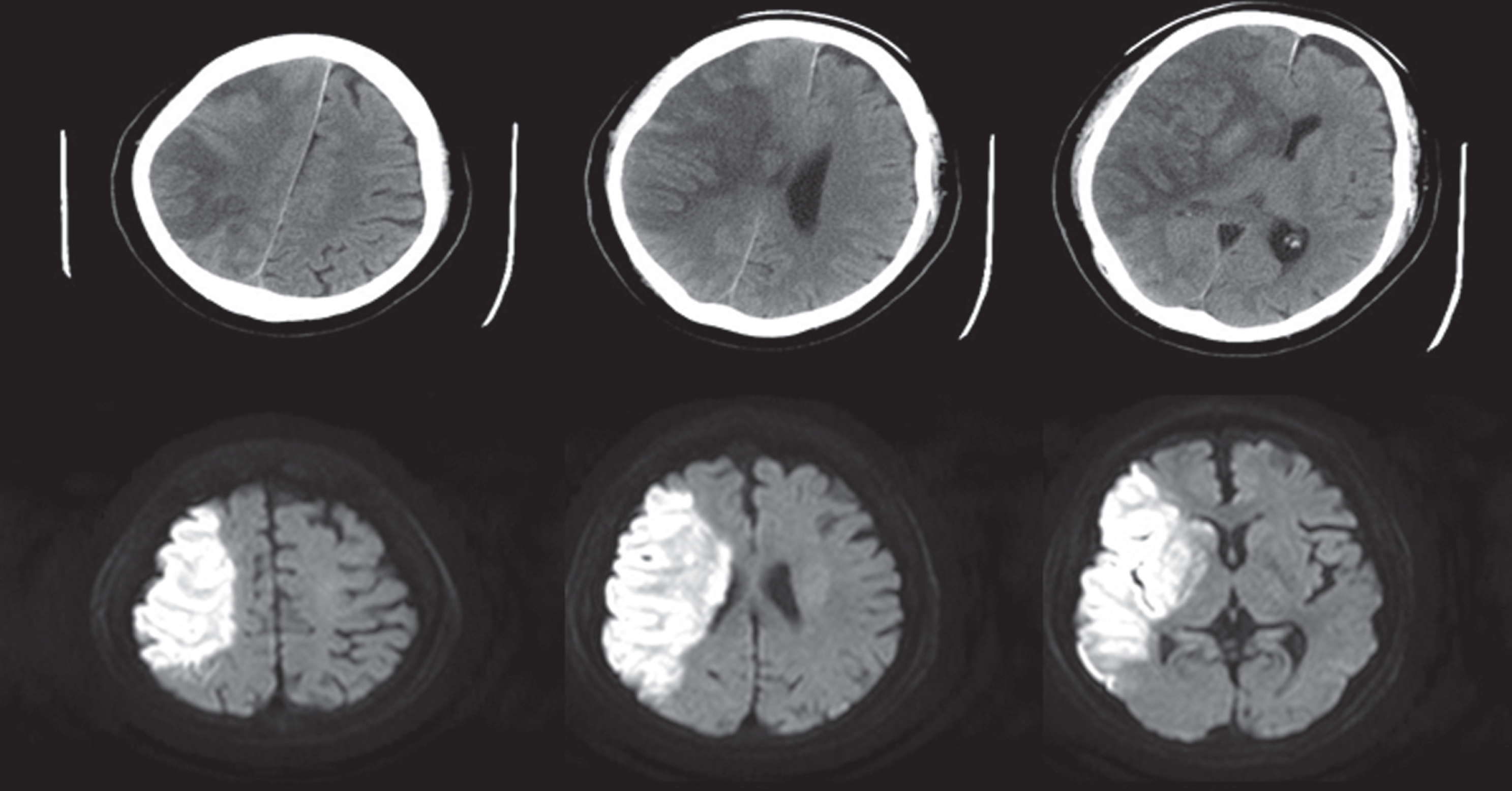
The head computed tomography scans for Case 1 are presented in the upper row, and the head diffusion-weighted magnetic resonance imaging (MRI) scans for Case 2 are presented in the lower row. A slight hemorrhagic infarction is observed in Case 1. In both cases, the images show right middle-cerebral artery embolism due to cardiogenic cerebral infarction (M1 occlusion).
Patient demographic and other characteristics
Abbreviations: BRS, Brunnstrom recovery stage; MMSE, Mini mental state examination; M, male. #BRS, Upper extremity/finger/lower extremity. *Evaluated by stroke impairment assessment set. †Score has a total 30 points (cut-off is 23 points).
Changes in clinical and outcome scores
Format for scale for contraversive pushing results = Sitting/Standing.
Electromyographic measurements
Target muscles in EMG measurements were the biceps brachii, triceps brachii, vastus lateralis, and biceps femoris muscles on the non-paretic side, and the rectus abdominis and erector spinae muscles bilaterally. A pair of disk electrodes of diameter 10 mm were placed on each muscle 20 mm apart for recording the EMG activity. Before the electrodes were placed, the skin was degreased with an alcohol swab and a layer of cuticle was then removed with a skin pretreatment agent to reduce the electrical resistance of the skin. The EMG signals were recorded using a Neuropack MEB-4208 (Nihon Kohden, Tokyo, Japan). The low-pass filter was set at 20 Hz, the hi-pass filter was set at 3 kHz, and the data were sampled at 20 kHz.
Participants sat in a seat that was adjusted to a height at which the knee joint was flexed at 90° and the soles of the feet were flat on the floor. Two measurement conditions were used: a trunk-upright condition with the hand on the non-paretic side resting on the seat 15 cm from the outside of the thigh, and a trunk-lateral bending condition in which the trunk was tilted 10° toward the non-paretic side with the hand on the non-paretic side resting on the seat 30 cm from the outside of the thigh. Because of the severity of the PB symptom, the positions of the measured extremities were configured by an assistant. Participants were asked to maintain their posture at a predefined position as well as possible while measurements were being made. Measurements were taken in 3 times for each condition. Since patients with PB resist correction of their posture, support by the assistant was minimized to avoid correcting the posture when measuring and recording the EMG activity. The EMG activity was measured 17 days after the onset of the symptom in Case 1, and 14 days after the onset of the symptom in Case 2.
Intervention
The effect of ES on PB was validated by a case-study ABA design, and trials began the day after EMG measurements were taken for both cases. A1 (baseline), B (intervention), and A2 (follow-up) were 2 days each, and for 1 hour/day during each phase, a conventional physical therapy for PB was administered (a balance exercise in a sitting position, an exercise in standing up with a verticality indicator, and a walking exercise using a knee-ankle-foot orthosis, among others). In phase B, an additional five-min ES was administered. The Torio 300 stimulator (Ito Co., Ltd., Tokyo, Japan) was used for delivering the ES. An array of two electrodes 5 cm apart was placed so as to be centered on the muscle belly of the biceps brachii as illustrated in Fig. 2, and the stimulus intensity was set to a value above motor threshold (25 mA intensity, 100 Hz frequency, and 300μs pulse width). ES was applied during sitting with the trunk-upright position, maintained with assistance from a therapist.

In preparation for electrical stimulation therapy, two electrodes separated by 5 cm are placed over the muscle belly of the biceps brachii.
Patients were evaluated using the stroke impairment assessment set (SIAS; Tsuji, Liu, Sonoda, Domen & Chino, 2000), a standardized measure of stroke impairment consisting of the subcategories: motor function, muscle tone, sensory function, range of motion, pain, trunk function, visuospatial function, speech, and unaffected-side function (see Appendix 1). PB was evaluated using the Scale for contraversive pushing (SCP; Karnath et al., 2002) and the Burke lateropulsion scale (BLS; D’Aquila, et al., 2004) (see Appendices 2 and 3). Patients were considered to have PB if they scored >0 points on any of the SCP subscales, and PB was considered most severe if the total score was 6 points. The minimum score on the BLS is 0 and the maximum is 17, and greater scores represent more severe PB. The trunk control test (TCT; Collin & Wade, 1990) was used to evaluate trunk performance. The TCT examines four axial movements: rolling from a supine position to the paretic side and to the non-paretic side, sitting up from a lying-down position, and sitting in a balanced position on the edge of the bed with the feet off the ground for 30 s. The scoring is as follows: 0, unable to perform the movement without assistance; 12, able to perform the movement but in an abnormal manner; and 25, able to complete the movement normally (total score range, 0 to 100). These assessments were performed by one of the authors who was not involved in administering the intervention.
Results
Characteristics of muscle activity
In the trunk-upright condition, EMG analysis showed greater muscular activity in the triceps brachii on the non-paretic side in both cases. In addition, the excessive muscle activity of the triceps was more significant in the trunk-lateral bending condition (Fig. 3).
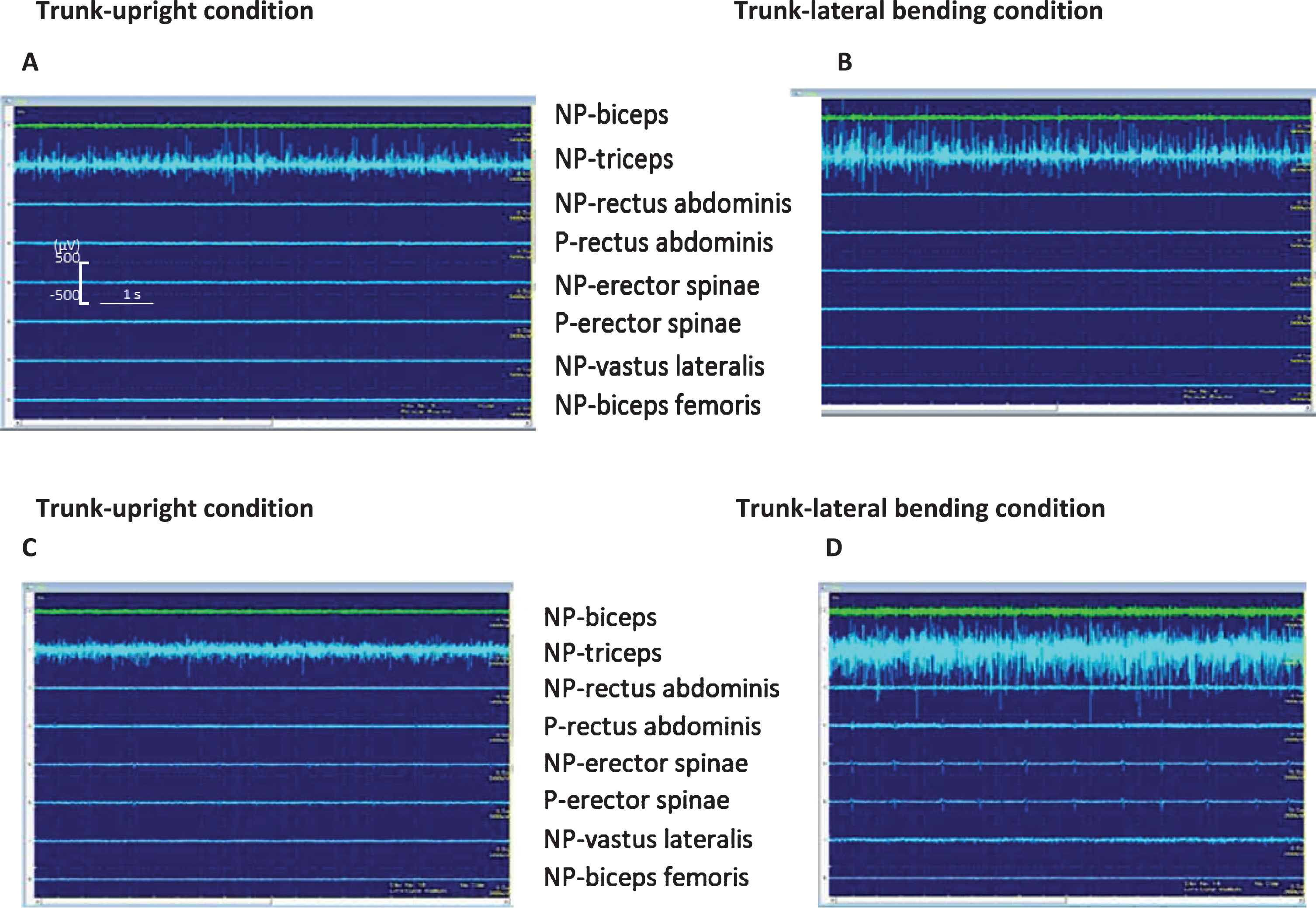
Electromyographic findings recorded with the participant sustaining a sitting position; A and B are the voltage traces for Case 1, and C and D are the traces for Case 2. In the trunk-upright condition, significant muscular activities are observed in the triceps in both cases. This tendency is even more significant in the trunk-lateral (sideways-leaning) condition. The scale bars shown in A apply to all four panels. NP, non-paretic side; P, paretic side.
Facilitating contraction of the biceps brachii muscle suppresses contraction of the antagonist muscle, which is the triceps brachii, by a spinal reflex. The triceps brachii muscle on the non-paretic side was identified in EMG measurements as a target for such indirect activity modification by electrical stimulation. Table 2 shows the results of applying ES to the biceps to suppress muscular activity in the triceps.
The SIAS score, the comprehensive evaluation for stroke, was low for both cases and no significant changes were observed after the intervention. In the SCP, PB scored as very severe for both cases. Both the SCP and BLS scores were reduced immediately by ES. In both cases, the SCP and BLS scores worsened slightly during the follow-up phase, but the PB during follow-up was nonetheless milder than during the baseline phase. The TCT score was poor during the baseline phase for both cases; however, this score improved after the intervention phase, with the result that both participants could sit independently.
Discussion
This is the first report on the characteristics of muscular activity and the effect of ES in patients with PB during sitting. Consequently, the present study was quite interesting in that it showed an instantaneous and significant treatment effect resulting from an intervention completely different from previous best practice. Previous best practice focused on manipulation of the sensory modalities used to perceive verticality.
Paci & Nannetti (2004) reported that treatment using visual or auditory feedback resulted in immediate positive effects for a sub-acute stroke patient. Their patients underwent physiotherapy over a 3-week period, and the SCP score improved from 4.75 points to 2.75 points. Krewer et al. (2013) compared the immediate after-effects of three different interventions (20 min per session) for PB in a cross-over trial. Their results showed that the reduction in PB was significantly greater with machine-supported gait training than with physiotherapy involving visual feedback components. The immediate benefits were noted only on the BLS, which can detect smaller changes than the SCP. Yang et al. (2015) tested the effect of a computer-generated interactive visual feedback training program in a randomized, controlled trial, and reported that the SCP for the intervention group improved by 4.0±1.1 points while that for the control group improved by 1.4±1.0 points after treating patients three times a week for three weeks. Although previous studies showed that these interventions had a certain level of effect, the time course of PB needs to be considered. Abe et al. (2012) reported on the length of recovery from PB and showed that PB spontaneously resolves after approximately two months even for severe cases. In the present study, the element of natural recovery was quite limited since the intervention lasted only 2 days, which suggests that the observed recovery was due to ES.
The ability of ES to suppress hyperactivity of the triceps brachii was as expected. A neural impulse originating from a muscle spindle of an agonist muscle propagates through the 1a nerve fiber, activating alpha motor neurons of the same agonist muscle while at the same time deactivating the motor neurons of the antagonist muscle via a spinal inhibitory interneuron. Deactivation by this mechanism is known as reciprocal inhibition. PB is abnormal movement in the “non-paretic side” of upper and lower limbs (ipsilateral hemisphere) and is not caused by brain damage as is the case for spasticity (contralateral hemisphere). Therefore, we conjectured that ES acts on the spinal reflex pathway.
However, it remains unclear why changes in local muscle activity improved balance ability. Wolpert et al. proposed a comparator model in which changes in the external world that accompany an exercise are detected by somatic and visual senses and are then fed back to the brain where a sensory prediction and the actual sensation are compared (error detection) (Wolpert, Ghahramani & Jordan, 1995). It has been shown that error learning takes place to correct this error (Imamizu et al., 2000). In other words, PB is considered to stem from impairment of error learning that normally corrects movements that are erroneous due to vertical misperception. The results of the present study may be attributed to suppression of erroneous movements by electrical stimulation, which reduced the discrepancy between sensory prediction and actual sensation per the comparator model. We conclude that ES based on EMG analysis may be effective for improvement of PB.
This study has a few limitations. First, the study is a case series, and validation is needed from cases with different severities and post-onset periods. Second, EMG evaluation was not performed after ES. Third, although we established that the EMG findings could be different between the sitting lateral and upright postures, the EMG status was not investigated for a standing posture because of the difficulty of maintaining our participants standing due to severe PB. Fourth, the EMG findings suggested that, in the sitting position, the triceps brachii muscle on the non-paretic side may induce PB, but the reason could not be shown. Many questions remain regarding the mechanism, effective treatment, etc., of PB, which merit further research.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.