
Abstract
BACKGROUND:
Unilateral spatial neglect (USN) is defined as impaired attention to sensory stimuli on one side. The symptoms can exist for near and far spaces combined or independently. Thus, it is important to evaluate both possibilities in a clinical environment.
OBJECTIVE:
To develop a tractable immersive virtual reality (iVR) system that can evaluate both near and far space neglect along with a proof of concept study to determine whether near and far spatial neglect could be described in an actual patient with USN.
METHODS:
An object-detecting task was developed in a three-dimensional virtual reality space. The examiner recorded the positional data of objects that were recognized by the patient with USN using coordinate data.
RESULTS:
The system could be used to detect near and far space neglects in a patient with USN. No side effects such as vertigo were seen during measurement. This patient showed that the angle for recognition was significantly larger for near space than far space, and exhibited a tendency for the angle of recognition to increase with lower height.
CONCLUSIONS:
Our proof of concept study indicated the possibility of applying an evaluation system that separates far and near space neglect using iVR.
Keywords
Introduction
Unilateral spatial neglect (USN) is defined as a failure to report, respond, or orient to novel or meaningful stimuli presented on the side opposite a brain lesion (Heilman, Valenstein, & Watson, 2000). It is one of the most prevalent higher brain dysfunctions. USN occurs in approximately 50% of stroke patients (Bowen, McKenna, & Tallis, 1999; Appelros, Karlsson, Seiger, & Nydevik, 2002; Nijboer, Kollen, & Kwakkel, 2013), and right hemisphere brain damage (e.g., inferior parietal lobe, superior temporal, frontal cortex, and subcortical nuclei) accounts for 90% of patients with USN (Buxbaum et al., 2004). This dysfunction critically interferes in daily life. For example, individuals with USN leave food on the neglected side of their plate and fail to look to the neglected side when crossing the street (Li & Malhotra, 2015).
USN can affect near and far spaces differently (Berti et al., 2002; Van der Stoep et al., 2013; Vuilleumier, Valenza, Mayer, Reverdin, & Landis, 1998; Aimola, Rogers, Kerkhoff, Smith, & Schenk, 2012; Cowey, Small, & Ellis, 1994; Keller, Schindler, Kerkhoff, von Rosen, & Golz, 2005). In actual clinical practice, cases of visual neglect have been observed for both far and near spaces, as well as either far or near space only (Aimola, Schindler, Simone, & Venneri, 2012). In fact, previous research indicates that neural circuits vary depending on space (i.e., inferior parietal cortex processing information in near space; superior and medial temporal cortex processing information in far space) (Previc, 1998). Experimentally induced lesions in monkeys also provide evidence to support neurobiological differences between near and far spaces. Specifically, resection of the frontal eye field impedes responses to stimuli in far space. In contrast, similar lesions in the adjacent prefrontal cortex compromise attention restricted to near space (Adair & Barrett, 2008). Thus, it is crucial to evaluate visual neglect affecting both near and far spaces in the rehabilitation setting.
Conventionally, the Behavioral Inattention Test (BIT) is commonly used to assess visual neglect, and it consists of paper-and-pencil tests (e.g., line cancellation or bisection task). However, such methods of evaluation can only assess neglect symptoms in a theoretical manner. One of the promising methods for USN assessment is virtual reality (VR). A VR system has the advantage of using an artificial environment in virtual space (Laver et al., 2012; Laver, George, Thomas, Deutsch, & Crotty, 2015). VR is essentially classified as either immersive or non-immersive reality (Laver et al., 2015). A 2015 review (Ogourtsova, Souza Silva, Archambault, & Lamontagne, 2015) reported that VR was an effective tool for the assessment of USN, although most existing VR systems have employed non-immersive VR. Two studies used an immersive VR (iVR) system for USN evaluation (Kim et al., 2010; Ogourtsova, Archambault, Sangani, & Lamontagne, 2018). One study demonstrated that the two groups (patients with USN vs. patients without USN) showed differences in several variables analyzed during the street-crossing task: deviation angle, left-to-right reaction time ratio, left visual, auditory cue rates, and left failure rate (Kim et al., 2010). Another study examined the feasibility of an assessment of USN symptoms in a functional shopping activity using iVR (Ogourtsova et al., 2018). The object detection task was performed in both simple and complex environments in patients with USN. Longer detection times, larger mediolateral deviations from ideal paths, and longer navigation times were found in patients with USN compared with stroke (patients without USN) and healthy control groups, particularly in the complex scene. However, these relevant studies were mainly focused on neglect in the far space (i.e., extra-personal space) (Kim et al., 2010; Ogourtsova et al., 2018). Furthermore, these studies could not quantitatively identify the actual neglect area of the patients in three-dimensional space (i.e., it was not possible to digitize symptoms ignoring data such as depth, height, or width). Therefore, the boundary between the neglected region and the recognizable region could not be discriminated, and it was not possible to specify the region to be interposed.
Thus, the objective of the present study was to develop and introduce a tractable system to evaluate USN for near and far space spatial neglect using iVR (near spaces were defined as within arm’s length or 0.5–1.0 m; far spaces were defined as being ≥1.0 m) (Ten Brink, Biesbroek, Oort, Visser-Meily, & Nijboer, 2019). We also performed a proof of concept study with the proposed system to determine whether near and far spatial neglect could be measured in an actual patient with USN.
Materials and methods
System overview
The device included a head-mounted device (HMD) (Oculus Rift, OculusVR, LLC, United States) and a personal computer (PC) (Fig. 1-A) (Yasuda, Muroi, Ohira, & Iwata, 2017; Yasuda, Muroi, Hirano, Saichi, Iwata, 2018). Original VR spaces were developed using software (Unity Technologies, San Francisco, CA, United States). The HMD was equipped (120° field of view, 2160×1280 graphics array resolution, 90 Hz frequency, weight of 440 g, and all peripheral vision blocked with only the virtual environment visible to the participant), the patient observed the room (14×7×3 m) in the virtual space from a first-person perspective, and then the target stimulant sphere appeared (0.11 m) (Fig. 1-B). The sphere appeared at angles at distances of 0.5, 1.0, 2.0, 3.0, 4.0, 5.0, and 6.0 m from the patient. The patient’s area of neglect for each fixed distance was recorded in the system, and the object (sphere) appeared in concentric circles centering on the patient’s head. The sphere was displayed between 36° and 144° (i.e., measured every 18°) (Fig. 1-C). To render neglect in three-dimensional terms, three levels of height were established on the basis of the height of the patient’s eye line. The line-of-sight height was set at 1.2 m above the ground, looking 6 m ahead. On the basis of the line of sight, height was set within the range of 1.6 m (–40 cm; high) and 0.8 m (–40 cm; low) at a height of ±4° from the patient’s line of sight (Fig. 1-D). The symptoms of neglect were recorded as angles for each distance and height based on whether the patient recognized the sphere that appeared within the virtual space, and a visual depiction was made based on that data.
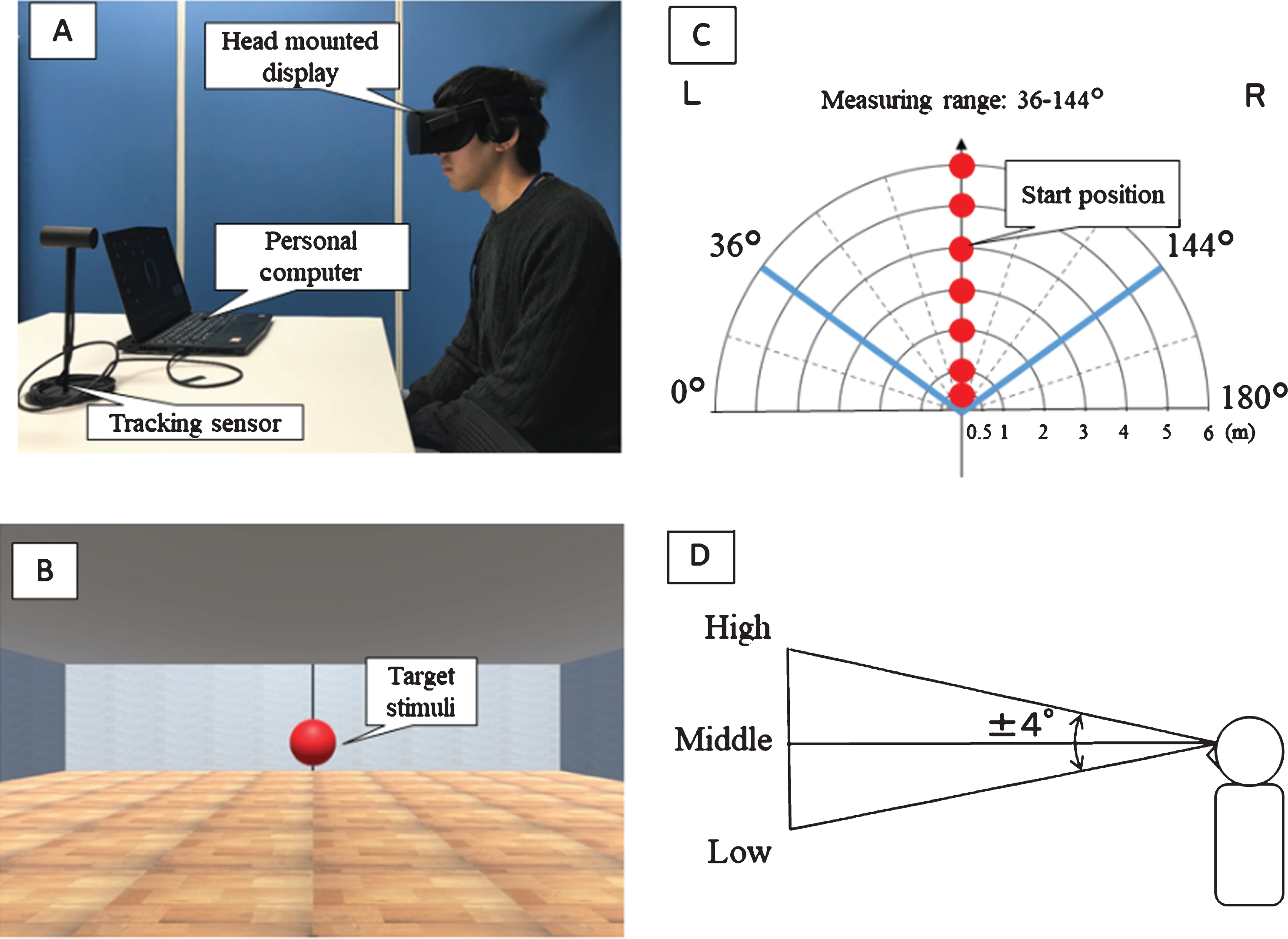
System overview: (A) The participant observed a VR space from a first-person perspective in a seated position with his head maintained at the exact middle. Written informed consent was obtained from the depicted individual for the publication of this image. (B) A sphere (0.11 m) appeared in the room (14×7×3 m) located within the VR spaces. The sphere appeared at angles at distances of 0.5, 1.0, 2.0, 3.0, 4.0, 5.0, and 6.0 m from the patient. (C) An object (sphere) appeared in concentric circles centering on the patient’s head. The sphere was displayed between 36° and 144° (measured every 18°). (D) Based on the height of the patient’s view, three stages of height were set (angles of±4° with the eye as the basis).
Assessments were conducted to ascertain the presence of neglect in both near and far spaces. The authors were especially interested in test performance related to spatial distance. To quantify the area of neglect in the virtual space, the height φ, distance r, and angle θ were set as coordinates. Regarding height, based on the height of the patient’s eye line, three levels of height were set. Figure 1-C shows a plane view of the positions in which the stimulus appears at each height. With this system, near spaces were those that were within arm’s length (0.5–1.0 m) and far spaces were defined as being ≥1.0 m (Ten Brink et al., 2019). The object appeared at distances of 0.5, 1.0, 2.0, 3.0, 4.0, 5.0, and 6.0 m from the patient. In addition, the sphere was displayed between 36° and 144°, centered on the patient’s head for the purpose of evaluation, and the area of neglect was recorded every 18° (Fig. 1-C). The evaluation was started from the median plane (i.e., 90°). To eliminate the effect of order, the object was displayed randomly at positions of 0.5, 1.0, 2.0, 3.0, 4.0, 5.0, and 6.0 m. When the object in each location was recognized, the location of appearance was shifted toward the side of neglect (i.e., left side) to detect the boundary of spatial neglect. Conversely, when the object was not recognized, the location of appearance was shifted toward the side of non-neglect. The examiner pressed a key to record in a PC whether the patient was able to recognize the object using coordinate data. For symptoms of neglect, the angles of the positions that were not recognized in the six distances were calculated, and the area of neglect was consequently visualized (Fig. 2).
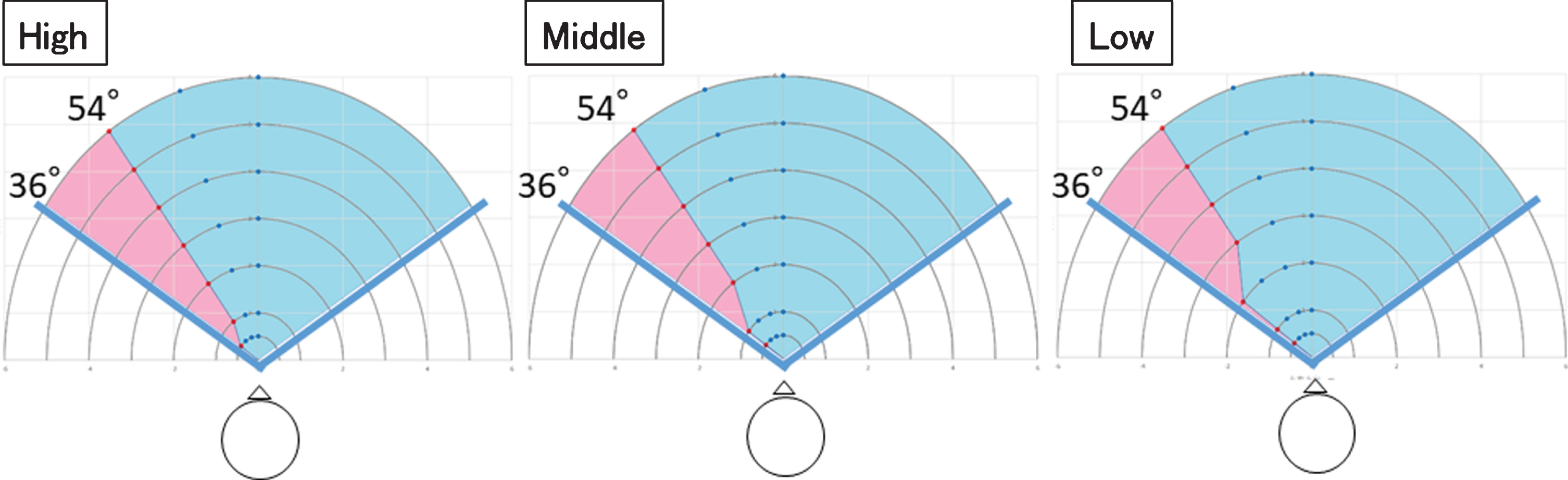
Patient neglect area. The range in blue is the area that was recognized and the range in red is the area that was neglected. (A; high, B; middle, C; low).
Diagnosis and clinical course
An 80-year-old right-handed man had been diagnosed with subcortical cerebral hemorrhage. At onset, computed tomography of the head revealed a 50 mL hematoma in the right parietal lobe. Conservative treatment was implemented, but the hematoma increased in size and the patient’s consciousness level decreased. Therefore, craniotomy was performed to remove the hematoma. Upon admission, the patient initially exhibited severe motor paralysis and higher brain dysfunction (USN, agnosia, and disturbance of attention), requiring assistance for all daily tasks.
Neurological and neuropsychological findings
Table 1 shows the clinical evaluation results of the patient (PJ). The motor paralysis was severe left hemiplegia. Brunnstrom stage was 2 for the upper limbs, 2 for the fingers, and 2 for the lower limbs. Sensory examination revealed severe torpor in both superficial sensation (tactile and pain sensation) and deep sensation (positional sensation and motor sensation). The patient had a normal range of vision. During testing, he could engage in simple communication. His mini-mental state examination (MMSE) score was 16 points. General disturbance of attention and unilateral spatial neglect were observed. His posture deviated toward the right in daily life. He could not engage in searching motions on the left side, and he had little control over his left lower body. He experienced difficulty performing the trail making test (TMT) and the BIT.
Participant characteristics
Participant characteristics
USN: unilateral spatial neglect, BRS: Brunnstrom’s Recovery Stage, FIM: Functional Independence Measure, FMA: Fugl-Meyer Assessment, FBS: Functional Balance Scale, TMT: Trail Making Test, BIT: Behavioral Inattention Test, MMSE: Mini-Mental State Examination.
All procedures were approved by Waseda University (approval number: 2015-251) and Sonoda Rehabilitation Hospital Ethics Committee for Human Research. After a complete description of the procedures and purpose of the study, written informed consent was obtained from the patient. This study was registered in the University Hospital Medical Information Network (UMIN) clinical trial registry (ID: UMIN000028356).
Procedure
The experiment was conducted in a noise-free rehabilitation room. The patient wore the HMD, and his head was kept at the exact middle point (0° rotation, 0° bend) in a seated position. The patient’s head was immobilized during the examination to prevent movement impacting the test reproducibility. During the experiment, the therapist immobilized the patient’s head by holding the head on both sides with their hands in the exact middle point to eliminate head movement. After the patient’s head was immobilized, it was confirmed that the center of the HMD matched the center of the VR space. A spherical object was displayed within the VR space, and the patient responded when he recognized the sphere. The examiner instructed the patient as follows: “If a red sphere appears within the space, say there is a sphere.” To confirm that there were no untruths in the patient’s responses, the reply included both the timing of the appearance of the sphere and its position. The time limit from ball appearance until patient response was set at approximately 30 s. Examiners recorded in the PC the positional information of spheres that were recognized.
Severe dizziness, nausea, epileptic attacks, fainting, etc., may occur because of motion sickness in VR environments (Zhang et al., 2016). Therefore, we confirmed with the patient whether he had experienced any of these symptoms after each experimental series.
Analysis
To compare the differences in the angles that were recognized in near and far spaces, the recognized angles were calculated for near spaces of 0.5 m and 1.0 m (arm’s length range) and far spaces of 5.0 and 6.0 m (i.e., the angle of near and far spaces in high/middle/low positions). Non-parametric analyses were performed due to the small sample size (Altman & Bland, 2009). The angles recognized in near spaces (three heights at 0.5 and 1.0 m: total of six data items) and the angles recognized in far spaces (three heights at 5 and 6 m: total of six data items) were compared using a Wilcoxon signed rank test. The significance level was set at ≤5%. Furthermore, we observed the recognized angles in high, medium, and low levels in both the near and far spaces. We also recorded general malaise during the experiment.
Results
No harmful effects such as dizziness or nausea were observed during the use of VR. Figure 2 shows the neglect areas for each height (see appendix, supplementary video for three-dimensional mapping of the neglected space). The range in blue is the area that was recognized, and the range in red is the area that was neglected. Results of the Wilcoxon signed rank test showed large values for the angles that were significantly recognized in near spaces (p = 0.0431). Furthermore, regarding near space, the patient exhibited a tendency for the angle of recognition to increase with lower height (Fig. 2).
Discussion
To quantify and demonstrate the areas of neglect in patients with USN in near and far spaces, an evaluation system was developed using iVR environment. In addition, a proof of concept study was performed by evaluating a patient with USN. The evaluation specified the neglected areas at six different near and far distances in a VR space, and it was performed without any negative effects. Notably, there were significant differences in the areas of recognition between near and far spaces (i.e., the angle for recognition was significantly larger for near space than far space), and the patient exhibited a tendency for the angle of recognition to increase with lower height. Despite the patient having a low level of physical function (Table 1) and inability to complete a paper-and-pencil test, the iVR system was able to delineate neglect regions in three-dimensional terms during evaluation. Therefore, these results confirm the possibility of applying a clinical evaluation system that separates far and near space neglect using iVR.
As stated in the introduction, there are patients with different symptoms of USN depending on far or near spaces (Berti et al., 2002; Van der Stoep et al., 2013; Vuilleumier et al., 1998 Aimola et al., 2012; Cowey et al., 1994; Keller, 2005). Currently, a paper-and-pencil test (i.e., BIT) is used in the clinical setting (Hartman-Maeir A & Katz, 1995). This conventional evaluation includes a line bisection and line cancellation test (Azouvi et al., 2002; Schenkenberg, Bradford DC, & Ajax, 1980), a star cancellation test (Halligan, Wilson, & Cockburn, 1990), and a letter cancellation test (Rorden & Karnath, 2010). In addition, in prior research using iVR, the focus had only been on far spaces (Kim et al., 2010; Ogourtsova et al., 2018), and there were no proposals for a small and tractable platform to systematically test near and far spaces. As evaluation with the device can be used to safely assess patients who cannot be evaluated by conventional paper-and-pencil testing (i.e., BIT or TMT) (Table 1), clinical application of this device may be possible in the future. It is essential to quantify and describe the neglect symptom as close to real-life situations as possible. This will support independent living for patients. To achieve this, we devised a system that could easily quantify an ignorable region in three-dimensional space and described the difference of ignorance region by depth or height. Using this system for evaluation, intervention corresponding to the neglected area that is truly problematic in real-life space could be possible and may contribute toward supporting independent living in the future.
In this report, a system is developed that records and visualizes the angle information of neglected areas by calculating the differences in distances from the patient based on iVR. Furthermore, the recognition of different angles in near and far spaces demonstrate different USN examples. This tendency agrees with previous research showing that the extent of neglect in near and far spaces is different depending on the patient (Cowey et al., 1994). Interestingly, a tendency was observed in this patient for wider regions to be recognized in a lower near space position. This demonstrates that differences in neglect may arise from small differences in height in near space. We believe that this needs to be further verified in the future.
In terms of the limitations of the experiment, although the patient’s head was maintained in a fixed position during the experiment, this fixed position is different than the actions of a patient in the actual living space. In the future, by using an evaluation in which the patient’s head moves freely, consideration can be given to specifying the areas of neglect that are close to actual living spaces. Furthermore, it is necessary to evaluate the reliability and validity of the equipment.
Conclusion
In conclusion, using the characteristics of immersive iVR environment, a USN evaluation system has been developed that enables the recoding and visualization of space neglect in both near and far spaces. When applying this to a patient with USN, we found that the angle for recognition is significantly larger for near space than far space, and this patient exhibits a tendency for the angle of recognition to increase with lower height. Thus, the applicability of an evaluation system using iVR system is shown; however, the reliability and validity must be confirmed for multiple examinees, and proof of clinical usefulness must be established.
Conflict of interest
The authors report no conflicts of interest.
Funding
This study was supported by the Tateisi Science and Technology Foundation, Grant-in-Aid for Junior Researchers (Technological Research Section: 18C13), Research Institute for Science and Engineering, Waseda University.