
Abstract
BACKGROUND:
Robot-assisted gait training (RAGT) can improve walking ability after stroke but the underlying mechanisms are unknown.
OBJECTIVE:
We evaluated the changes in the injured brain after RAGT and compared the effects of early start and late start of RAGT.
METHODS:
Eleven patients with hemiplegia after stroke undergoing inpatient rehabilitation were examined within 3 months of stroke onset and were randomly assigned into two groups. Group 1 started RAGT with conventional physiotherapy immediately after enrollment, whereas Group 2 underwent conventional physiotherapy for 4 weeks before starting RAGT. We acquired diffusion tensor imaging data after enrollment and at 4 and 8 weeks after treatment. Fractional anisotropy (FA) and mean diffusivity (MD) maps were used to analyze the neural changes.
RESULTS:
Repeated measures analysis of variance of the data at 4 weeks after treatment showed a significant interaction between time and groups (RAGT versus control) for the FA and MD values in the non-lesioned hemisphere, indicating that the non-lesioned hemisphere was significantly reorganized by RAGT compared with conventional physiotherapy. Analysis of the data at 8 weeks after treatment showed a significant interaction between time and groups (early and late start of RAGT) for the MD values in the motor-related areas bilaterally, indicating that early start of RAGT significantly accelerated bi-hemispheric reorganization as compared with late start of RAGT.
CONCLUSIONS:
Our findings indicate that RAGT can facilitate reorganization in the intact superior temporal, cingulate, and postcentral gyri. Furthermore, early start of RAGT can accelerate bi-hemispheric reorganization in the motor-related brain regions.
Introduction
Gait recovery after stroke is one of the most important goals of rehabilitation therapy (Faria-Fortini, Polese, Faria, & Teixeira-Salmela, 2019). Repetitive practice of gait is a method for improving gait function that is based on facilitation of neuroplastic changes (Yang et al., 2017). However, patients with hemiplegia after stroke have difficulty performing repetitive ideal gait motion because of the lower limb weakness and spasticity of the hemiplegic side. Robot-assisted gait training (RAGT) can provide a solution to this problem because it enables more supportive ideal gait training (Mehrholz, Elsner, Werner, Kugler, & Pohl, 2013; Seo et al., 2018).
RAGT has been reported to be effective in combination with physiotherapy for achieving independent walking (Mehrholz et al., 2017). However, the mechanism by which RAGT aids gait recovery is still unclear. Previous studies have shown that RAGT can improve gait function, as evaluated by the functional ambulation category (FAC), timed up and go tests and three-dimensional motion analysis (Park & Chung, 2018; Seo et al., 2018). These studies have demonstrated the functional improvement, but the neuroplastic changes in the injured brain after RAGT remain unknown. Yang et al. have reported the changes in the injured brain using diffusion tensor imaging (DTI) obtained before and after RAGT (Yang et al., 2017). However, this study had no control group for comparison with the patients who underwent RAGT.
Thus, the purpose of this study was to identify the neuroplastic changes in the brain after RAGT by DTI data analysis. In addition, we compared the effects of early and late start of RAGT.
Methods
Patients
Seven male patients with stroke were recruited based on the following inclusion criteria: (a) first ever unilateral stroke confirmed by magnetic resonance image (MRI) or computed tomography; (b) supratentorial stroke within the last 3 months; (c) FAC≤3 (FAC 5: ambulates on stairs and inclines; 4: ambulates on level surface; 3: ambulates with one person on standby; 2: requires intermittent support; 1: requires continuous support; 0: cannot ambulate or requires more than one person’s help) (Holden, Gill, & Magliozzi, 1986); (d) at least 18 years of age; and (e) cognitive function sufficient to allow cooperation. The exclusion criteria were: (a) progressive or unstable stroke, or (b) coexisting neurological and/or orthopedic disease that could impair locomotion. Four age- and lesion size-matched male patients who had participated in a previous research on RAGT were also included (Yang et al., 2017).
The study was approved by our Institutional Research Ethics Committee for Human Subjects (approval no. 2017-05-008). Informed consent was obtained from all patients.
Study design
This study was designed as a prospective, single-blind, randomized controlled study (Fig. 1). Patients were recruited from an inpatient rehabilitation center at the Veterans Health Service Medical Center between July 2017 and September 2019. Those who met the eligibility criteria were randomly assigned to Group 1 or Group 2 through a stratified randomization approach. Group 1 started RAGT immediately after enrollment, whereas Group 2 started RAGT 4 weeks after enrollment. RAGT consisted of 20 sessions of 45 minutes of gait training with Walkbot (P&S Mechanics, Seoul, South Korea), 5 days per week. The patients’ clinical status was evaluated after enrollment using the Fugl-Meyer motor assessment of lower extremity (FMLE) scale, Motricity index (MI) of lower extremity, FAC, and trunk control (TCT) tests. MRI data were acquired immediately after enrollment, 4 weeks after enrollment (Group 1: after 20 RAGT sessions, Group 2: before RAGT), and 8 weeks after enrollment (Group 2: after RAGT). The patients from the previous research only had two MRI data, before and after RAGT.
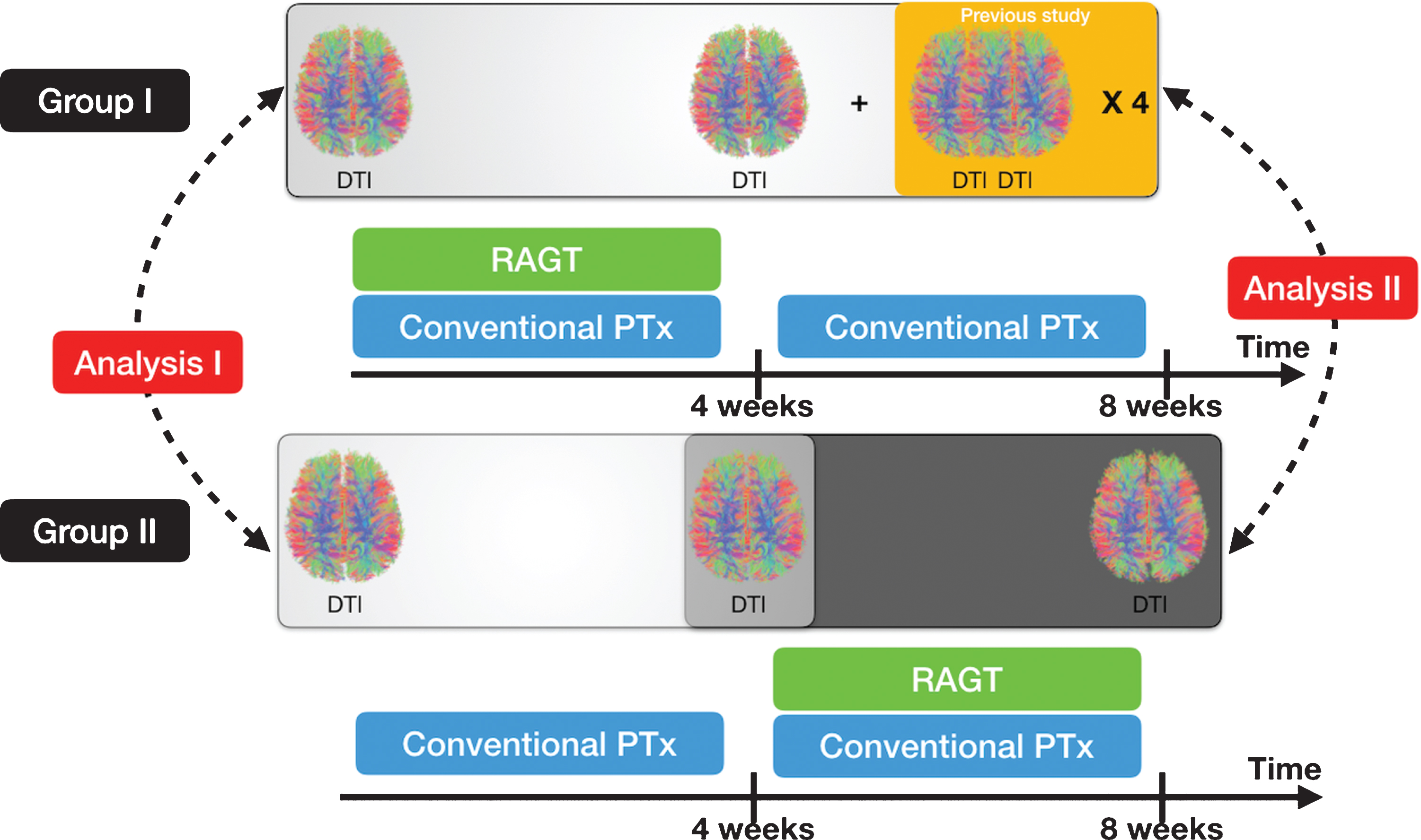
A simplified version of the study design. The figure demonstrates the schedule for magnetic resonance imaging and the comparison of Analyses I and II.
Walkbot (P&S Mechanics, Seoul, South Korea) is a robotic-driven gait orthosis for control of posture, a body-weight support system, and a treadmill. A suspension vest and harness connected to a counterweight system provide lumbopelvic stability and body weight support. These were placed on the patient and the patient’s hip, knee, and ankle joint axes were consistently positioned with the exoskeletal orthosis for adjustment of joint movements at individualized gait speeds. As function improved, the treadmill speed was increased to a maximum of 2.2 km/h, with the level of assistance by the exoskeletal orthosis maintained at 100% throughout all sessions.
MRI acquisition and preprocessing
All images were acquired with a 3 T clinical whole-body MR scanner (Siemens, Erlangen, Germany) using a 20-channel head coil. The 3D T1-weighted image parameters were: TR/TE = 1900/2.57 ms, matrix = 256×256, field of view = 230×230 mm2, flip angle = 9, and slice thickness = 1 mm. DTI parameters were: TR/TE = 9700/92.0 ms, matrix = 112×112, field of view = 224×224 mm2, NEX = 1, 30 directions, b = 1000 s/mm2, and slice thickness = 2 mm. MRIs from 2 patients with left hemispheric lesions were flipped to identify the corresponding lesion area in the right hemisphere for further analysis. After flipping, the DTIs were registered to the corresponding b = 0 images with an affine transformation to correct distortions due to eddy current using the FMRIB Software Library 5.0.10 (http://www.fmrib.ox.ac.uk/fsl). The fractional anisotropy (FA) and mean diffusivity (MD) maps were constructed in native space and registered to the standard Montreal neurological institute template, provided by Statistical Parametric Mapping 12 (http://www.fil.ion.ucl.ac.uk/spm). The registered FA and MD maps of all patients were then averaged and smoothed with a Gaussian kernel of 4 mm full-width at half-maximum. The smoothed images were used for further statistical analysis.
Statistical analysis
We evaluated the effects of RAGT on the brain structure by repeated measures analysis of variance (RM-ANOVA) using Multivariate and Repeated Measures toolbox version 1.1 (http://www.click2go.umip.com/i/software/mrm.html) (McFarquhar et al., 2016). We evaluated the effects of time and intervention through two analyses. First, we analyzed the MRI data taken at enrollment and 4 weeks after enrollment, that is, before and after RAGT in Group 1, and before and after conventional physiotherapy in Group 2 (Analysis I in Fig. 1). Thus, Analysis I is a comparison between RAGT and control, as patients in Group 2 had undergone only conventional physiotherapy. Second, we analyzed the MRI data taken before and after RAGT in both groups (Analysis II in Fig. 1). Thus, Analysis II is a comparison of the effect of early start of RAGT with that of late start of RAGT. The significance level for RM-ANOVA was uncorrected p < 0.0001 (McFarquhar et al., 2016). Wilcoxon’s signed rank test with post-hoc was performed to compare the significant FA and MD voxels between the groups. Wilcoxon’s rank sum test was performed to compare the baseline characteristics of both groups, including age, lesion volume, days after stroke, and FMLE, FAC, MI, and TCT scores. The significance level was set at p < 0.05.
Results
Patients’ characteristics
The mean age of the patients was 74.5±8.4 years in Group 1 and 72.8±0.4 years in Group 2. Enrollment time since stroke was 41.5±25.6 days in Group 1 and 43.6±2.5 days in Group 2. Ten patients had an ischemic stroke and one patient had a hemorrhagic stroke. Nine lesions were in the right hemisphere and two were in the left hemisphere. There was no statistically significant difference in the baseline characteristics between the two groups. Table 1 summarizes the general and clinical characteristics of all patients and Fig. 1 summarizes the lesion data.
Patients’ general and clinical characteristics
Patients’ general and clinical characteristics
RM-ANOVA showed a significant interaction between time (pre, post) and group with an FA value of the superior temporal gyrus of F = 54.82 and MD values of the cingulate and postcentral gyri of F = 117.59 and F = 48.71, respectively, in the non-lesioned hemisphere. The post-hoc comparisons with the baseline values showed that the FA value of the superior temporal gyrus and the MD values of the postcentral gyrus were significantly increased after RAGT (Fig. 2 and Table 2).
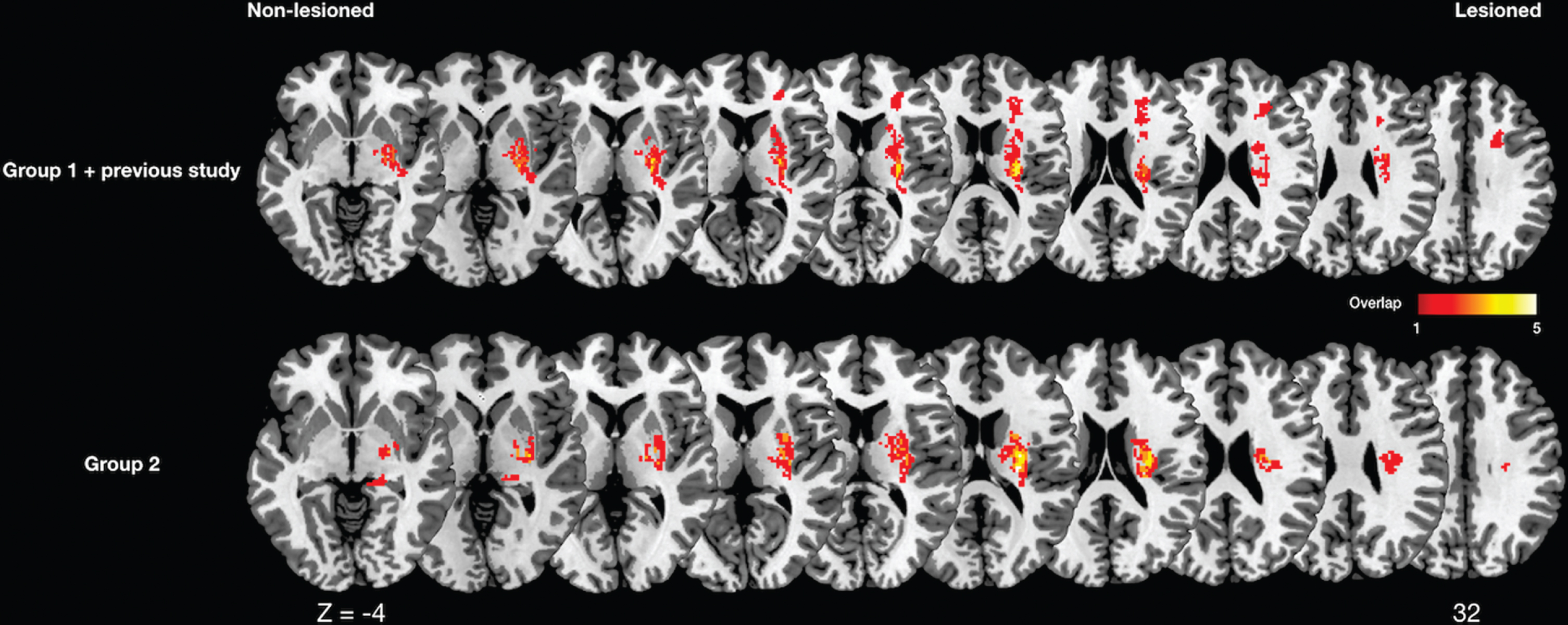
Lesion overlapping maps. A T1-weighted template was used to demarcate lesions for every patient. The color scale indicates the percentage of overlapping lesions across patients. Group 1 started robot-assisted gait training immediately after enrollment and Group 2 started robot-assisted gait training 4 weeks after enrollment.
Changes in fractional anisotropy and mean diffusivity maps
Days, duration after stroke; FMLE, Fugl-Meyer motor assessment for lower extremity; FAC, functional ambulation category; MI, motricity index; TCT, trunk control test; L, left; R, right; CR, corona radiata; MCA, middle cerebral arterynon-lesioned, non-lesioned hemisphere; lesioned, lesioned hemisphere; FA, fractional anisotropy; MD, mean diffusivity. The threshold was set at uncorrected p value <0.0001.
RM-ANOVA showed a significant interaction between time (pre, post) and group with MD values of the extranuclear and cingulate gyri of F = 109.47 and F = 89.21, respectively, in the non-lesioned hemisphere, and an MD value of the precentral gyrus of F = 73.45 in the lesioned hemisphere. The post-hoc comparisons with the baseline values showed that the MD value of the precentral gyrus was significantly increased after early start of RAGT (Fig. 3 and Table 2).
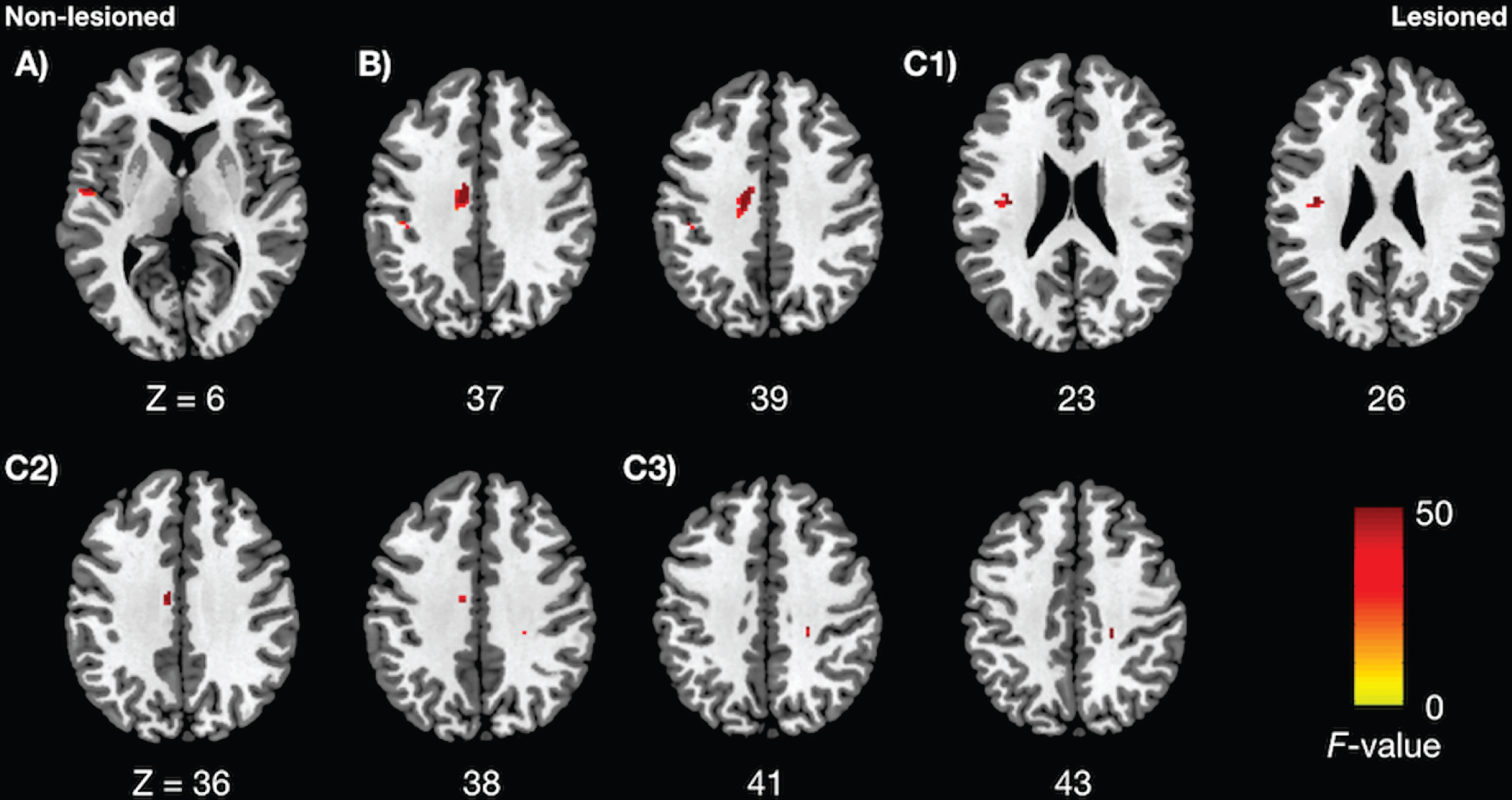
Changes in fractional anisotropy (FA) or mean diffusivity (MD) (uncorrected p < 0.0001). A) Significantly increased FA in robot-assisted gait training compared with control; B) Significantly increased MD in robot-assisted gait training compared with control; C1-3) Significantly increased MD in early start compared with later start of robot-assisted gait training.
In this study, we found that RAGT facilitated microstructural reorganization mainly of the non-lesioned hemisphere, including the superior temporal, cingulate, and postcentral gyri. Furthermore, early start of RAGT facilitated reorganization of the motor-associated brain regions in the bilateral hemispheres. The FA value measures the uniformity in the movement of water molecules along the white matter tracts; increased FA values indicate increased structural connectivity (S. H. Lee, Kyeong, Kang, Kyeong, & Kim, 2019). The MD value, a quantitative measure of the mean motion of water, describes the microstructural diffusion properties (Kwon, Park, Seo, Na, & Lee, 2015). The increase in diffusion properties is likely to be manifested as an enhancement of tissue organization resulting from neuronal or glial alteration (Sagi et al., 2012; Umarova et al., 2017).
Reorganization was mainly facilitated in the non-lesioned hemisphere after RAGT. Non-lesioned hemisphere facilitation has been correlated with worse outcomes in upper limb function (Askim, Indredavik, Vangberg, & Haberg, 2009; Marshall et al., 2009). However, conflicting results have been reported on the role of the non-lesioned hemisphere for lower limb function and gait (Enzinger et al., 2008; Yang et al., 2017). The non-lesioned hemisphere has the capacity to contribute to the function of the affected limb, but does not make any significant contribution in healthy subjects (Carey, 2017; Jankowska & Edgley, 2006). The bilateral innervation for some lower limb functions may account for a different role of the non-lesioned hemisphere in lower limb function compared with that in upper limb function. Namely, some functions, such as language and fine motor control of the upper limbs, are lateralized to the left or right hemispheres (Kyeong, Kang, Kyeong, & Kim, 2019; Price, 2010). Gait, however, is associated with bilateral activation of both the primary and the supplementary motor cortices in a normal person (Chieffo, Comi, & Leocani, 2016). RAGT in this study involved repetitive gait motion in patients after unilateral stroke and facilitated rearrangement of the non-lesioned hemisphere, which had a better recovery potential than that of the lesioned hemisphere.
The early start of RAGT facilitated reorganization in both the lesioned and non-lesioned hemispheres. In the subacute phase after stroke, perilesional activation has been observed, particularly near the motor cortical area (Carey, 2017; Kleiser, Wittsack, Butefisch, Jorgens, & Seitz, 2005). The enhanced perilesional excitability transmitted to the intact brain regions that can cover the injured function (gait in this study) (Butefisch et al., 2005; Carey, 2017). It was found that the early start of repetitive gait training using RAGT may bilaterally activate the lower limb representing areas in the brain (D. H. Lee, Hong, & Han, 2014). Furthermore, previous studies have reported that early intensive rehabilitation appears to determine motor improvement (Boake et al., 2007; Kwakkel, Wagenaar, Twisk, Lankhorst, & Koetsier, 1999). Therefore, repetitive training using RAGT, which involves bilateral lower limb activity, may induce bi-hemispheric changes only in the early stage after stroke. There is no significant correlation between bi-hemispheric changes and clinical improvement, but early activation and reorganization may be correlated with long-term improvement after stroke.
There were limitations in this study that should be considered when interpreting the results. First, this study had a relatively small sample size with heterogeneity in stroke etiology. Second, the left hemisphere lesions were flipped to the right side; thus, the contribution of laterality to right or left hemisphere in gait function is unclear. Third, this study only included male patients because of our institutional characteristics. Because the gait characteristics and recovery process after stroke between men and women are different, our findings may not be generalizable to all populations. Despite these limitations, this is the first study to show the effect of RAGT compared with a control group. Furthermore, we also investigated the difference between early and late start of RAGT after stroke. A longitudinal study with a large sample is required to evaluate the association with clinical improvement.
In conclusion, RAGT facilitates gait recovery by activating multiple brain areas of the non-lesioned hemisphere. The early start of RAGT may have an additional beneficial effect to the perilesional brain areas in the lesioned hemisphere. Therefore, repetitive training using RAGT may induce bi-hemispheric changes only in the early stage after stroke.
Conflict of interest
The authors declare no conflicts of interest.
Funding
The study was supported by a grant from the National Research Foundation of Korea, funded by the Ministry of Science and ICT, Government of Korea (No. 2017R1C1B1003132).