
Abstract
BACKGROUND:
Children with unilateral cerebral palsy (UCP) experience an asymmetrical gait pattern and poor balance capabilities. Effective interventions, therefore, are needed to facilitate remediation of these functional issues.
OBJECTIVE:
This study was set out to investigate the emerging role of stretch-shortening cycle (SSC) exercises on gait-symmetry and balance in children with UCP.
METHODS:
In this randomized controlled trial, 42 children with UCP (age; 8 –12 years) were enrolled and received either standard physical rehabilitation (control group; n = 21) or the SSC exercise program plus physical rehabilitation (SSC group; n = 21). Spatial- and temporal-gait symmetry index (GSI) and specific balance capabilities [reactive balance, directional control, movement synchronization, and sensory organization] were assessed before and after 16 sessions that were carried out twice/week over non-sequential days in an 8-week program.
RESULTS:
Using the pre-treatment scores as covariates, the post-treatment spatial- (P = 0.006;
CONCLUSION:
The evidence from this study suggests that SSC exercises besides standard physical rehabilitation appear to be effective for improving gait symmetry and boosting balance capabilities in children with UCP.
Introduction
Cerebral palsy (CP) is a group of permanent disorders of movement and posture that appears during infancy due to an unprogressive lesion to, or malformation of the developing/immature brain before, during, or immediately after birth (Morris, 2007). The population-based studies from different countries reported prevalence estimates varying between 1–5 /1000 live-births (Stavsky et al., 2017). About 33–39% of children with CP experience paralysis and spasticity of one side of the body that develop after damage to the part that controls movement in the contralateral brain’s hemisphere, which is categorized as unilateral CP (UCP) (Novak, Hines, Goldsmith, & Barclay, 2012).
Most children with UCP have asymmetrical alignment, where bodyweight support takes place preferentially through the non-paretic lower extremity as a compensatory strategy for the muscle weakness in the paretic side (Elnaggar, Elbanna, Mahmoud, & Alqahtani, 2019; Shumway-Cook & Woollacott, 2007). This compensatory strategy, although functional, it could not be efficient, owing to some factors related to increased energy cost and long-term overuse injuries (Jeng, Holt, Fetters, & Certo, 1996; Raja, Joseph, Benjamin, Minocha, & Rana, 2007). The asymmetry in weight-bearing, in addition to other impairment factors such as spasticity, paresis, loss of selectivity, irregular muscle co-activation, and contractures may lead to asymmetric development of walking (spatially and temporally) and reduce children’s balance capabilities (Elnaggar, 2021, 2020a; Gracies, 2005). On that basis, therapeutic interventions that enhance strength, promote wight-shift on the paretic side, and boost balance control, are warranted to enhance the motor functions in children with UCP (Damiano & Abel, 1998; Elnaggar et al., 2019; Ki, Kim, Moon, & Choi, 2015).
Stretch-shortening cycle (SSC) exercises –also referred to as plyometric exercises, is a form of explosive strengthening exercises in which muscles generate maximum force in brief time intervals (De Villarreal, Requena, & Newton, 2010). The SSC is a three-phase muscle contraction involved in dynamic movements, where muscles move rapidly through eccentric, isometric, and concentric phases (Davies, Riemann, & Manske, 2015). In SSC exercises, muscles are pre-loaded with a rapid stretch during the eccentric phase and store elastic energy to elicit enhanced force during the concentric phase (Davies et al., 2015). The use of SSC exercises has been identified as a possible treatment strategy for improving motor functions in children with CP. The SSC exercises have been demonstrated to promote gross motor function, strength, and agility in children with CP (Johnson, Salzberg, MacWilliams, Shuckra, & D’Astous, 2014). Two recent studies concluded that SSC exercises are an effective treatment approach for increasing muscle strength, enabling weight-bearing symmetry, regularizing muscle co-activation, and enhancing postural control in children with UCP (Elnaggar, 2020b; Elnaggar et al., 2019). The SSC exercise has also been found to be effective for increasing bone mass and lean body mass in children with Down’s syndrome (González-Agüero et al., 2011; González-Agüero et al., 2012), and enhancing motor performance in children with neurofibromatosis type-I (Barbara A Johnson, Salzberg, & Stevenson, 2012).
Even though SSC exercises showed positive effects on some aspects of motor function, further studies are needed to substantiate its effect on balance control in children with UCP. To our knowledge, the effect of SSC exercises on the spatial and temporal gait-symmetry has not been appraised in earlier investigations. The main objective of this study was, therefore, to assess the effect of SSC exercises on gait-symmetry and balance in children with UCP.
Methods
Study design
This prospective, randomized clinical trial was undertaken in the Physical Rehabilitation Center of Prince Sattam bin Abdulaziz University (PSAU) between October 2018 and November 2019. A single-blind protocol was implemented. The researcher who collected the data remained blinded to the treatment allocation. Before enrollment, children and their caregivers were informed about the study procedure and they have signed a consent form to authorize the participation. The study protocol was approved by the Ethics Review Board at the university (No: RHPT/0018/0078). The study procedures followed the code of conduct governing the ethical aspects of human research as stated in the 1975 Declaration of Helsinki. The study was also registered at ClinicalTrials.gov (Identification code: NCT04892576).
Participants
The study enrolled 42 children with CP from Physical Rehabilitation Center and University Hospital at PSAU and King Khalid Hospital, Al-Kharj, Saudi Arabia. Participants were included if they aged between 8 and 12 years, had an established diagnosis of UCP (Rosenbaum et al., 2007), had spasticity grade 1 or 1 + per the modified Ashworth scale (Ansari, Naghdi, Arab, & Jalaie, 2008), and if they had a motor function ability of level I or II as determined by the Gross Motor Function Classification System (Palisano et al., 1997). Exclusion criteria were fixed contractures, botulinum neurotoxin-A injections during the past six months, history of orthopedic or neurosurgery in the past year, attentional neglect, and cardio-respiratory comorbidities prohibiting involvement in explosive activities, and inability to attend for treatment twice per week through 12 weeks.
Sample size estimation
To determine the sample size needed to detect a clinically relevant treatment effect, we conducted a priori power analysis using G-Power software, version 3.1.9.7 (Neu-Isenburg, Germany). Estimates of the mean difference (μ1 - μ2 = 0.37 –0.28 = 0.09) and pooled standard deviation (SDpooled = 0.08) for the spatial symmetry index were collected from a pilot study. In a two-sided, two-sample equal-variance t-test with an alpha level of (α=0.05), a total of 36 children (i.e., a group sample-size of 18 children) was required to achieve a power of (1 –β= 90.63%) to reject the null hypothesis of equal means (i.e., H1: μ1 - μ2¬ =0). We expected a dropout of 10–15%, and therefore inflated the sample-size to 42 children (21 for each group).
Randomization and allocation
To assign eligible participants into two equal-size groups, we implemented a simple randomization procedure. An independent off-site researcher who was not a part of this study used a concealed allocation method. Participants were assigned a number from 1 to 42 on the order in which they were recruited. An online randomizer tool (GraphPad®, QuikCalcs, La Jolla, CA, USA) was used to randomly scramble an equal number of participants among two intervention slots as follows: The standard physical rehabilitation (control group; n = 21) or SSC exercises plus standard physical rehabilitation (SSC group; n = 21).
Outcome measures
Gait-symmetry indices
Gait analysis was performed through the Vicon 3D motion analysis system (Vicon 612, Vicon Motion Systems Ltd., Oxford, UK). The system uses passive light-reflective markers that are automatically traced during movement by 12 infrared-cameras placed around the laboratory’s perimeter at a sampling rate of 1200 Hz. Before any measurements were obtained, the system was calibrated, and the projection volume was adjusted such that the walking-path was within the cameras’ viewing field. During measurement, 17 retroreflective markers were attached to the skin overlying specific landmarks on the pelvis and lower limbs per the user manual and as described in previous studies (Elnaggar & Abd-Elmonem, 2019; Elnaggar & Elbanna, 2019). Participants were then asked to walk barefooted across a 10-meter walking-path with a comfortable walking pace. Two pre-test trial were dedicated before three testing trials to familiarize them with the procedure. Three complete gait cycles were selected from the middle of the walking-path from each testing trial to analyze the spatiotemporal features. We selected the middle three gait cycles to avoid possible influences of gait acceleration and deceleration at the start and the end of the walking-path. The average data of the three testing trials were computed and used for the analysis.
For this study, measurements of the step length of the paretic side (SLparetic) and non-paretic (SLnon - paretic) sides were used to estimate the spatial gait-symmetry index (spatial-GSI) and the single-limb support time of the paretic side (SLSTparetic) and non-paretic side (SLSTnon - paretic) were used to calculate the temporal gait-symmetry index (temporal-GSI) as follows: the spatial-GSI =[1 – (SLparetic/SLnon - paretic)], and the temporal-GSI =[1 – (SLSTparetic/SLSTnon - paretic)]. Lower values of these indices suggest more symmetry (Elnaggar, 2020a; Elnaggar, 2021).
Balance capabilities
Balance capabilities were quantified using a PRO Balance Master (NeuroCom® International Inc., Clackamas, OR, USA). The system comprises a square force platform (46×46 cm) that can rotate around a single axis. Measurements were carried out while participants standing barefoot on the platform with lateral border of their feet appropriately aligned to one of 3 marks on the platform surface, which was determined by the participant’s height. The reactive balance test, rhythmic weight shift test, and modified sensory organization test (mSOT) were the specifically investigated aspects of balance. Testing details are demonstrated below.
The reactive balance test determined the ability of the participants to preserve a stable upright posture following an unexpected perturbation. This was tested by measuring the latency in response to external disturbance in the lower leg musculature. Postural perturbations were triggered by rotating the force platform in the sagittal plane (i.e., upward, and downward). Six perturbations (3 trials for each direction) were investigated over a period of 800 milliseconds at an amplitude of 8 degrees, which were the maximum ranges of the PRO Balance Master at a sampling rate of 1 kHz. To reduce the anticipatory responses, the perturbations’ order was randomized for each participant, and each testing occasion. Surface electromyography (EMG) electrodes (Trigno™, Delsys, MA, USA) were attached to the gastrocnemius and tibialis anterior muscles. While this study included children with UCP, we only collected the EMG data from the paretic side. The EMG signal was sampled to a frequency of 1 kHz over an overall sampling duration of 1 second. The recording started 100 milliseconds before the onset of the perturbation to measure the baseline activities. The EMG signals were full-wave rectified at 0.01 kHz and high-pass filtered between a bandwidth of 0.06 kHz and 0.6 kHz. The mean value of the baseline activities was calculated for each muscle and subtracted from the EMG signal. The onset-latency for each muscle was detected through a computer algorithm and was determined when the processed EMG signals were two standard deviation above the baseline activities of that muscle for more than 50 milliseconds. Since children with CP are known to have a delayed muscle response on exposure to external perturbation (Woollacott et al., 2005), the significant reduction in the onset latency implies enhancement of the children’s performance.
The rhythmic weight shift test gave insights concerning the directional control and synchronization of movement. For testing, participants shifted their bodyweight front-to-back or side-to-side to control the position and movement of the center of pressure (CoP), which was represented by a cursor displayed on a computer interface. They were asked to match the position and timing of a target moving straightly between two end-points. A pre-practice session was dedicated to participants to ensure that they understood the procedure. Then, three testing trials were performed at slow, medium, and fast velocities (i.e., at 3 seconds, 2 seconds, and 1 second between the two end-points respectively). The target position was maintained consistently across all testing occasions. The values of directional control were analyzed by the NeuroCom software and defined as the extent to which the CoP was controlled during the excursion (i.e., the percentage of the on-axis/off-axis of the traveled distance) (Alsalaheen, Haines, Yorke, & Broglio, 2015).
The mSOT provided a global indication of the ability to maintain balance. During the mSOT, participants were instructed to stand with their upper limbs at their sides, look straight forward, and stand as still as possible for a period of 20 seconds while they were subjected to four testing conditions; 1) stable platform –eyes open, 2) stable platform –eyes closed, 3) sway referenced platform –eyes open, and 4) sway referenced platform –eyes closed. Three trials were permitted for each sensory condition and data were averaged across the three trials. The balance score was created by calculating the CoP velocity under each of the four testing conditions. A significant reduction in the mean CoP velocity indicates an improved performance. Additionally, the mSOT data were analyzed to identify the aggregate CoP displacements in the anterior/posterior (AP) and medial/lateral (ML) directions (Ramstrand & Lygnegård, 2012).
Interventions
Standard physical rehabilitation
Children in the control and SSC groups underwent 45-minute physical rehabilitation sessions, repeated twice per week for eight consecutive weeks under a strict control of a senior pediatric physical therapist. The program was customized to address the physical limitations of each child and generally intended to optimize physical functioning levels, enhance muscle strength, reinforce child’s stability and position, improve mobility, minimize the compensatory movement patterns, and promote normal walking patten. The program included a combination of strength training exercises, muscle relaxation techniques, postural and flexibility exercises, advanced balance training, and gait training exercises (Tecklin, 2015; Elshazly & Elnaggar, 2016).
Stretch-shortening cycle exercises
Besides the standard physical rehabilitation, children in the SSC group received a 30-minutes of SSC exercises in keeping with the guidelines stated by the National Strength and Conditioning Association (Faigenbaum et al., 2009) and safety standards issued by the (American Academy of Pediatrics, 1999). The SSC sessions were conducted twice weekly in non-sequential days over eight consecutive weeks on the same days they attended for standard care sessions with a minimum of 30 minutes rest-intervals. The training was supervised by a licensed pediatric physical therapist with a 1 : 1 therapist-to-child proportion. The SSC exercise program was adopted from a previous study in children with UCP (Elnaggar et al., 2019) –detailed information about the program is outlined in Supplementary Table 1. The program comprised 10 explosive exercises, which were basically focusing on lower limb strength training. The SSC exercises included a range of unilateral and bilateral jumping, hopping, and bounding variations, which were horizontally and vertically-oriented. The training progression was achieved by increasing the number of repetitions in two blocks, each block lasted for four weeks. The number of repetitions that children began with in the first block has been identified from a preliminary test of the children’s performance. A pre-training session was devoted to learning children about the proper excursion of each exercise. To optimize children’s performance a pre-training warm-up was applied for five minutes by way of stretching exercises and low-intense aerobic exercises on a stationary bicycle or a treadmill per children’s preference. Also, the training was ended with a 5-minute cool-down through low-intense SSC and stretching exercises. All exercises were performed on a rubber ground while participants were using footwear with plenty of cushioning.
Statistical analysis
The statistical software Stata version 15.1 (Stata Corp, College Station, TX, USA) was used for the data analysis. Skewness and kurtosis test for normality was performed and symmetry plots were created to determine whether data sets were symmetric about the mean. The intention-to-treat principle was applied for analyzing data. The multiple regression imputation was applied to substitute the missing data. The analysis of covariance (ANCOVA) test was used to compute the post-treatment difference in gait and balance variables between the control and SSC groups using the pre-treatment values as covariates. The partial eta-squared formula (
Results
Participants’ flow and retention
A flowchart depicting participants’ recruitment and retention through phases of the study is demonstrated in Fig. 1 Sixty-eight children were initially screened for eligibility. Of them, 42 children satisfied the criteria for inclusion and were randomized into the study groups. Four children (9.5%) have been lost during the study (three children from the control group and one from the SSC group did not complete either for unknown reasons or moved from the working area). However, the intention-to-treat analysis preserved the data of lost children.
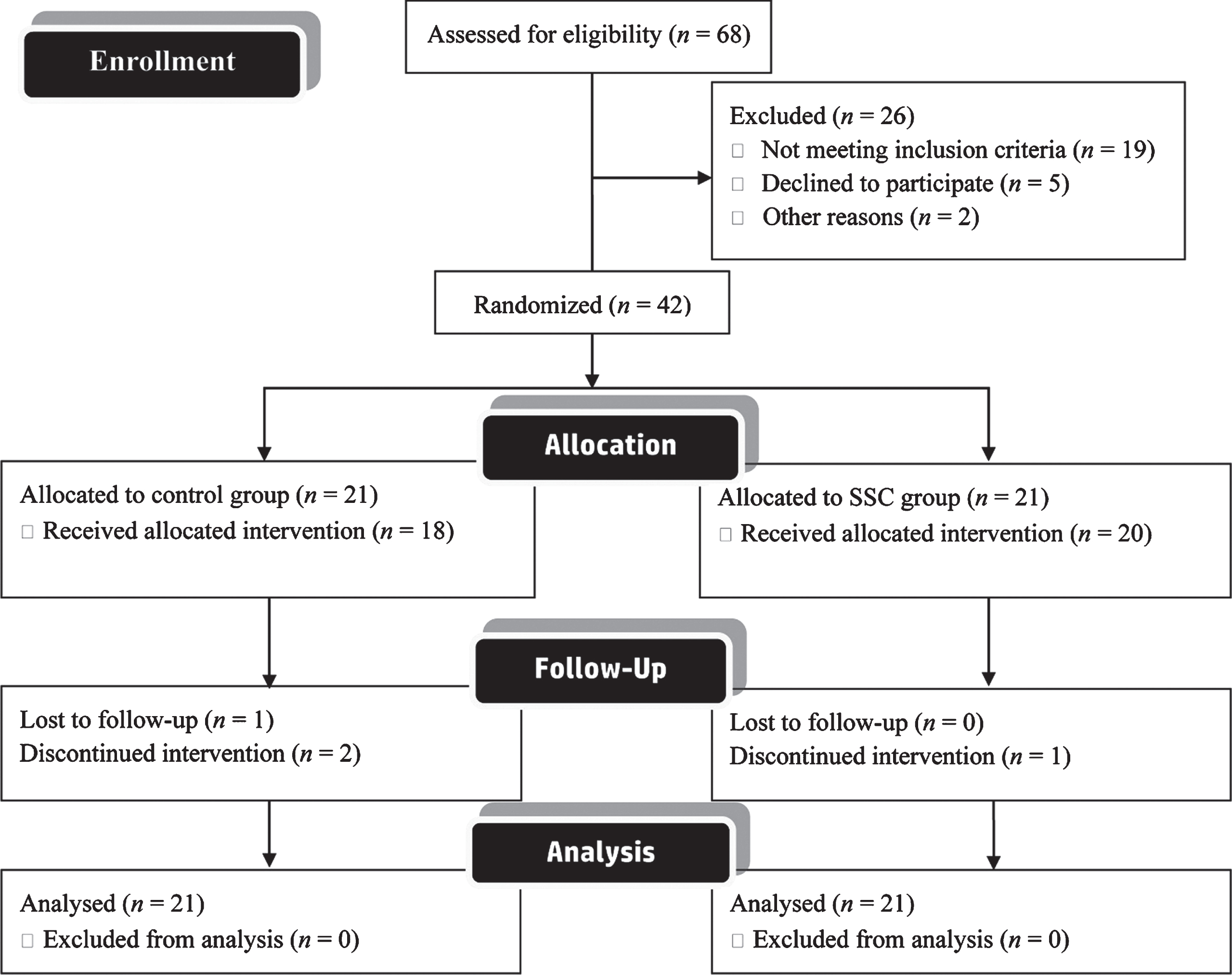
A flowchart depicting participants’ recruitment and retention through phases of the study.
Table 1 presents the participants’ demographic and clinical characteristics and group comparison regarding dependent variables at the baseline. The participants’ age, anthropometrics (weight, height, and BMI), and clinical (spasticity grade, motor function level, and paretic side) characteristics were homogenous among the study groups (P > .05). Additionally, dependent variables (i.e., gait-symmetry and balance variables) in both groups were comparable at the baseline (P > .05).
The baseline characteristics of the participating children
The baseline characteristics of the participating children
SSC: stretch-shortening cycle, b/g: boys/girls, BMI: body mass index, GMFCS: gross motor function classification system, MAS: modified Ashworth scale, SLparetic, step length of paretic side, SLnon - paretic, step length of non-paretic side, SLSTparetic: single-limb support time of the paretic side, SLSTnon - paretic: single-limb support time of the non-paretic side, GSI: gait symmetry index, AP: anterior/posterior, ML: medial/lateral, mSOT: modified sensory organization test.
The between-group differences in gait-symmetry as per the ANCOVA analysis are depicted in Table 2. There were statistically significant between-group differences in SLparetic [F (1,39) = 27.81, P < 0.001], SLnon - paretic [F (1,39) = 9.68, P = 0.003], and SLSTparetic [F (1,39) = 16.95, P < 0.001] when adjusted to the pre-treatment values, where the SSC group showed preferable changes as compared to the control group. However, there was no significant between-group difference with respect to the SLSTnon - paretic [F (1,39) = 2.09, P = 0.16]. Regarding gait-symmetry, there were significant between-group differences in spatial-GSI [F (1,39) = 8.50, P = 0.006] and temporal-GSI [F (1,39) = 32.84, P < 0.001] controlled for the pre-treatment scores. The SSC group showed lesser symmetry indices than the control group suggesting favorable improvements.
ANCOVA results of the post-treatment difference in gait-symmetry between the control and SSC groups controlled for the pre-treatment values
ANCOVA results of the post-treatment difference in gait-symmetry between the control and SSC groups controlled for the pre-treatment values
SSC: stretch-shortening cycle, SLparetic, step length of paretic side, SLnon - paretic, step length of non-paretic side, SLSTparetic: single-limb support time of the paretic side, SLSTnon - paretic: single-limb support time of the non-paretic side, GSI: gait symmetry index,
The between-group differences in balance measures are presented in Table 3. When adjusted to the pre-treatment scores, the average onset latency of gastrocnemius and tibialis anterior muscle decreased significantly in the SSC group as compared to the control group following perturbations in the upward [F (1,39) = 5.47; P = 0.025 and F (1,39) = 7.69; P = 0.008 respectively] and downward [F (1,39) = 6.60; P =0.014 and F (1,39) = 4.98; P = 0.032 respectively] directions. Also, the directional control increased significantly in the SSC group in both the AP [F (1,39) = 7.54, P = 0.009] and ML [F (1,39) = 9.46, P = 0.004] directions when compared to the control group. Further, the CoP velocity and the total CoP displacement either in the AP or ML directions decreased significantly in the SSC group as compared to the control group during the four sensory conditions (all P values < 0.05).
Post-treatment difference in balance variables between the control and SSC groups adjusted to the pre-treatment values
SSC: stretch-shortening cycle, AP: anterior/posterior, ML: medial/lateral, mSOT: modified sensory organization test,
The initial objective of the study was to determine the effect of SSC exercises on gait-symmetry and balance capabilities in children with UCP. The findings of this study indicate that using SSC exercises for 30 minutes, twice weekly over eight weeks besides the standard physical rehabilitation is more effective than using the physical rehabilitation alone for optimizing the gait symmetry and balance capabilities in children with UCP. The SSC exercises led to improved gait-symmetry, as reflected by the significant decreases in the spatial- and temporal-GSI of the paretic limb. Also, the SSC resulted in enhanced balance control, which was evidenced by the significant decreases in average onset latency of the leg muscle following external perturbations, CoP velocity, and total CoP displacement in different sensory conditions and the significant increase in the directional control during the movement excursion.
To date, the effect of SSC exercises on gait-symmetry in children with UCP has received scant attention in the published literature, which may clear up the significance of the results from the current study. The most important clinically relevant finding to emerge from this study was that SSC exercises improved both distance- and time-related gait symmetry. As previously mentioned, the paretic versus non-paretic side discrepancies concerning the spatial/temporal parameters of gait in children with UCP are related to the unilateral involvement and reluctance to transfer and support full body weight on the paretic side (Elnaggar et al, 2019; Shumway-Cook & Woollacott, 2007), abnormal muscle activities, and abnormal postural mechanisms (Elnaggar, 2020b). The SSC exercise protocol employed herein has been geared toward bilateral training and targeted the side-to-side weight-bearing differences. Although not a measurement-based, the distinctive effect of SSC on spatial- and temporal gait-symmetry can be explained by the potential increase in weight dissemination on the paretic side, which may have led to improved postural control and decreased inter-limb differences with respect to the step length and support time. Supporting this claim, a previous clinical trial reported that the SSC exercises for 45 minutes have the potential to increase the weight-support on the paretic side and improve some aspects of gait performance (such as the proportion of single-limb support, step time, stride length, and walking velocity) in children with UCP as applied twice per week for eight consecutive weeks (Elnaggar et al., 2019). Another explanation for the improvement in gait symmetry is that SSC exercises increased the muscle strength in the paretic side and enhanced postural control (De Villarreal et al., 2010; Elnaggar, 2020b; Elnaggar et al., 2019). As a result, the propulsive force generated by the paretic side, hip extension, and foot dorsiflexion might have been increased during paretic-limb support, and thus reduced the difference between paretic and non-paretic forward foot placement relative to the trunk during initial contact (i.e., decreased the variations observed in step-length asymmetry) and allowed a greater percentage of weight-bearing on the paretic side during stance phase (i.e., increased the single-limb support time on the paretic side) (Roerdink & Beek, 2011).
The current study found also that SSC exercises improved reactive balance, directional control, and sensory organization. The leg muscles’ response-latency, CoP velocity, and total CoP displacement decreased following destabilizing perturbations, whereas the on-axis/off-axis ratio and synchronization during movement excursion increased, implying that SSC exercises may be beneficial to improve various aspects of postural control. These results accord those of a recent study which investigated the effect of a progressive SSC exercise program, applied twice/week over three successive months in a sample of children with UCP and demonstrated remarkable improvements in muscle-activation strategies and the children’s capacity to preserve balance when subjected to external postural perturbations (Elnaggar, 2020b). Our results also extend those of previous investigations on healthy adolescents, which stated that short-term SSC exercises applied at a moderate frequency (i.e., twice per week) has a large effect on improving balance control (B. A. Johnson, Salzberg, & Stevenson, 2011; Ramírez-Campillo et al., 2015). It seems possible that these results are due to improved leg muscle activities and agonist/antagonist co-activation patterns. Such an argument is supported by Chimera et al. who pointed out that SSC exercises can modify muscular activities and produce neuromuscular adaptations that enable the opposing muscle groups to co-activate symmetrically, which is required during dynamic restraints to maintain balance across the joints (Chimera, Swanik, Swanik, & Straub, 2004). This perhaps is supported in part by the results concerning the decline in the average onset-latency of the gastrocnemius and tibialis anterior in our study, proving the changes in muscle activities following SSC exercises. Also, the dynamic nature of SSC exercises may have played a role in improving balance. Such an exercise paradigm involves rapid and repetitive transitions between muscle lengthening and shortening that have been claimed to contribute to muscle force/work and enhance the mechanical efficiency of movement (Elnaggar, 2020b). Additionally, SSC exercises provide a wide spectrum of balance challenges as the center of gravity moves in the horizontal and vertical directions, thus created a neural adaptation that enhances children’s balance capabilities (Chaouachi, Othman, Hammami, Drinkwater, & Behm, 2014). Further, the SSC exercises are associated with an increase in the proprioceptive input to the brain evoked by the myotatic stretch reflexes (Seo, Shin, Yoon,& Han, 2010), which increases the overall kinesthetic awareness, speeds up the onset of contraction of stabilizing muscles (Chimera et al., 2004), and promotes a short-latency agonist/antagonist co-activation, all of which contribute to boosting the balance capabilities (Hogan, 1984).
The findings of the present study may somewhat be limited by the scarcity of comparable data from CP cases, thus further studies on the effect of SSC exercises in children with CP or other developmental disorders are suggested to confirm the results shown herein. The sample was restricted to children with UCP who show greater motor abilities than other types of CP. Hence, there is abundant room for further progress in determining how children with different types of CP would respond to SSC exercises. This study examined children aged 8 –12 years. Therefore, there is still an unanswered question about the effect of SSC exercises on children with UCP at younger or older age-groups. This study did not follow the treatment effect in the long term. Further studies, which take this point into account, need to be undertaken.
Conclusion
The findings of this investigation suggests that the use of SSC exercises besides the standard physical rehabilitation is effective for improving gait-symmetry and enhancing balance in children with UCP. It is, therefore, recommendable for the rehabilitation professionals to include this exercise-model in the treatment of this patient population.
Footnotes
Acknowledgments
The authors are thankful to all participants and their families for their cooperation and participation in this study. The authors also thank the Biomechanics Laboratory team of the Department of Physical Therapy and Health Rehabilitation at PSAU for their assistance and cooperation.
Conflict of interest
The authors declare that they have no conflicts of interest regarding the publication of this article.