
Abstract
BACKGROUND:
Hemiparetic patients lose the ability to move their trunk selectively, abdominals are affected and neither voluntary nor reflex activity is present.
OBJECTIVE:
To investigate if the inclusion of specific exercises for the trunk muscles in a rehabilitation program for chronic hemiparetic patients could lead to an additional improvement.
METHODS:
A multiple-participant single-subject design was replicated in patients with hemiplegia. The study was conducted in two cycles: for the first cycle (A), patients received conventional rehabilitation program, then for the second cycle (B), six months later, the same subjects received conventional rehabilitation therapy plus an additional specific selective trunk muscles training. Trunk Impairment Scale (TIS), Berg Balance Scale (BBS), 10 meters distance walk test (10 MWT), Functional Independence Measure (FIM) and instrumental gait analysis were performed before and after both treatment cycles.
RESULTS:
Significant changes were observed in TIS and 10 MWT after the two treatment cycles. However, after treatment cycle B, BBS and FIM score showed an additional improvement. Whereas, after treatment cycle A gait analysis did not relevantly changed, but after cycle B a significant improvement was registered in velocity, cadence and percentage of stance in the gait cycle.
CONCLUSIONS:
In our patients, the training for selective activation of the trunk muscles had led to a consistent improvement of gait analysis parameters, and hemiparesis-related disability in stance and activities of daily living.
Introduction
Trunk muscle control and trunk stability are relevant features for rehabilitation strategies in stroke patients, which are traduced in the length of stay reduction and motor functional enhancement (Verheyden at al., 2009; Franchignoni at al., 1997). Trunk muscles are key structures for the preservation of lumbar and pelvic girdle stability, and their contribution is a milestone for optimal limb movements and control (Kibler et al., 2006). Chronic stroke patients frequently present strength asymmetry of the trunk due to a unilateral weakness of flexor and extensor muscles, which can affect gait ability and balance (Marigold et al., 2006). A systemic review by Cabanas-Valdes et al. (2013) described the efficacy of trunk training for the improvement of trunk control. A meta-analysis by Alhwoaimel et al. (2018) confirmed the results obtained by Cabanas-Valdes, especially for the dynamic subscale of Trunk Impairment Scale, but claimed the lack of evidence about trunk training efficacy on upper limb function (Van Criekinge et al., 2019). Moreover, trunk training was studied assessing the muscular thickness and activity (Van Criekinge et al., 2018).
A systematic review (Van Criekinge at al., 2019) analyzed eight studies that unstable surface trunk exercise is useful in the rehabilitation stroke patients and studies (Bae at al., 2013; Yoo et al., 2014; Seo at al., 2012) shown a significant balance ability and transversus abdominis thickness variation, whether internal and external obliques muscles did not.
Other studies examined the effect of trunk training on the activity of lower back and lower limb muscles, which resulted to be both increased versus the control group (Lee et al., 2014; Yu et al., 2013; Kim et al., 2011). Specifically, quadriceps and soleus muscles appeared to be more recovered than others (Kim et al., 2011; Dean et al., 1997). Moreover, a large effect was recorded in studies assessing mobility in patients who were not completely able to walk and have a safe stance. Chung et al. (2013) assessed the effects of trunk training on step length and cadence in stroke patients with a minimal gait ability, showing an improvement of velocity and cadence. Notwithstanding this, to the best of knowledge, no researches in terms of the effects of specific trunk training on gait functionality even after a suboptimal rehabilitation program are present in chronic stroke patients. Therefore, the study aims to assess if trunk muscular training can be observed even in chronic hemiparetic stroke patients after a preview standard rehabilitation program, and the amplitude of its effect on gait ability, biomechanics and clinical.
Material and methods
Participants
All patients were admitted for a comprehensive rehabilitation program to the Division of Neurology and Neurorehabilitation - IRCCS Institute Auxologico Italiano. The experimental procedure was explained in detail to participants, the study was carried out in accordance with the ethical standards of the Institute Auxologico Italiano and with the 1964 Declaration of Helsinki and its latest amendments; written informed consent was obtained from the participants. Inclusion criteria were: (1) Unilateral supratentorial hemispheric stroke of more than 3 months duration before recruitment; (2) In sitting, ability to bend forward and come upright again; (3) Ability to walk with or without aid for 20 m; and (4) Ability to understand and follow verbal or non-verbal instructions.
Medically unstable patients with a history of any other neurological disease, patients with psychiatric disorders, alcoholism, vestibular or orthopedic disorders that could affect balance. Patients with a recent history of acute low back pain or disorders of the musculoskeletal system were excluded.
Design of the study
A multiple-participant single-subject design was replicated in the patients. The study was conducted in two cycles: in the first cycle (Treatment cycle A), all patients received one hour of a conventional rehabilitation program five days a week for four weeks i.e. in the second cycle (Treatment cycle B), six months later, the same subjects received one hour of conventional rehabilitation therapy plus an additional 1/2 hour of specific selective trunk muscles training for the four weeks. Clinical and functional assessments and instrumental evaluations were performed before and after both the treatment cycles (T0: pre-Treatment cycle A; T1: post-Treatment cycle A; T2: pre-Treatment cycle B; T3: post-Treatment cycle B). For the instrumental evaluation, a group of healthy subjects age-matched (Control Group, CG) was considered to have provided normative data.
Intervention
The treatment of the motor impairments combined elements from different commonly used physiotherapy concepts for treating patients with neurological diseases. The main emphasis was on the neurodevelopmental treatment concept (Richards at al., 1995) and motor relearning strategies (Hunter at al., 1961; Jackson at al., 1895) (active mobilization, muscular strengthening, mobilization of the nervous system and task-oriented activities) and was applied for 1 hour, 5 times a week, for 4 weeks.
The key features of the treatment protocol were additional specific exercises to retrain selective trunk activity, performed for 30 minutes, 5 times a week, for 4 weeks (for a total of 10 hours of additional training). These exercises consisted of selective movements of the upper and lower part of the trunk in supine and sitting according to those suggested by Klein-Voghelbach et al. (2004) and Davies (1990). Selective trunk activity means the ability to move one part in isolation, be it with flexor or extensor activity, while the rest of the trunk is stabilised or moves in a different direction to the other part. The ideas of Klein Vogelbach in her concept of functional kinetics provide different exercises to retrain selective trunk activity with the following suggestive names: The Bridge: is formed when two parts of the body, in contact with a supporting surface, hold that part of the body situated between them away from the supporting surface. The arch of such bridge is maintained by the muscles of the underside of the arch being activated. The Tentacle: is a part of the body which moves against the pull of gravity with its distal extremity free, in the sense of not being supported. If the parts are not absolutely vertical, the muscle activity to support the “tentacle” will take place in those muscle groups on its uppermost side in relation to the pull of gravity. The Bridge/Tentacle: combining the bridge and the tentacle in certain movements, the muscle activity changes accordingly as the muscles on the uppermost side of the bridge will need to be activated as well in order to anchor the tentacle arising from it.
Exercises were performed in two positions: In lying: mobilising the rib-cage and the sternum, upper trunk rotation, with the legs crossed and knees flexed swaying from side to side, bridging with “tentacle”, and gymnastic ball exercises with the lower limbs, supported on the ball moving from lying to sitting with rotation. In sitting: balance reactions, selective pelvic tilting forward and back, selective side flexion of the lumbar spine.
Exercises were gradually introduced and the number of repetitions was determined by the therapist based on the patients’ performance. The intensity of the exercises was increased by introducing one or several of the following changes: 1) reducing the base of support; 2) increasing the lever arm; 3) advancing the balance limits; 4) increasing the holding time.
The activities to retrain selective trunk activity must be carried out very exactly because the patient will otherwise use compensatory or alternative muscle activity to perform them. Even 1-centimetre shift of weight or a tiny alteration in the position of the body can change the activity from flexion to extension or vice versa. Other stroke rehabilitation activities such as occupational therapy, nursing care, neuropsychological and speech therapy were provided if needed.
Outcome measures
Clinical and functional examinations: Trunk Impairment Scale (TIS) (Verheyden et al., 2004), Berg Balance Scale (BBS) (Downs et al., 2013), 10 meters distance walk test (10 MWT) (Cheng et al., 2020) were the outcome tools to measure the trunk control, balance and gait parameters respectively; functional disability was assessed using raw scores of the Functional Independence Measures scale (FIM™) (Hamilton et al., 1987) with its total score and the sub-score of motor ability. All the outcome measures were collected by a physiotherapist who was not involved in conducting the study intervention. All clinical assessments were conducted within 72 hours of admission and at the time of discharge.
Instrumental evaluation (Gait analysis - GA): All patients were quantitatively evaluated using an optoelectronic system with 6 cameras (460 VICON, Oxford Metrics Ltd., Oxford, UK), two force platforms (Kistler, CH) and a video system. After the collection of some anthropometric measures, passive markers were placed at special points of reference, directly on the subject’s skin, as described by Davis et al. (1990), to evaluate the kinematics of each body segment. After one-minute walking in the laboratory in order to gain familiarity with the environment, subjects were asked to walk barefoot at their own natural pace (self-selected and comfortable speed) along a (8 m long) walkway where the two force platforms were placed. At least six trials were collected for each subject in order to ensure the consistency of the data. All graphs obtained from GA were normalized as % of gait cycle. While kinematics (angles of the main lower limbs) and kinetics were also acquired during this study, it is not included in the present analysis and are not discussed in this paper. In the present study, only spatio-temporal gait variables were analyzed. In particular, the considered parameters were: Velocity (m/s): mean velocity of progression; Cadence (step/min): Number of step for minute; % stance (% gait cycle): % of gait cycle that begins with initial contact and ends at toe-off of the same limb; Step length (m): longitudinal distance from one-foot strike to the next one.
Statistical analysis
All the previously defined parameters were computed for each participant and then the mean values and standard deviations of all indexes were calculated before and after each treatment cycle (T0, T1, T2 and T3 sessions) for the patients and Control Group.
The Kolmogorov–Smirnov tests were used to verify if the parameters were normally distributed; the parameters were not normally distributed, so to detect significant differences between the two treatment phases at baseline (T0 vs. T2) the Mann-Whitney U test was used and to measure the treatment output differences the Friedman’s test (alpha < 0.05) was applied and the post-hoc comparisons was performed by the Bonferroni’s test. The data of the patients and CG were compared with Mann-Whitney U tests. Statistical significance was set at p < 0.05.
Results
Twelve patients were enrolled in this study (8 men, 4 women; mean age 56 years (range 38–84); mean body weight was 73.9±14.9 kg). All had suffered their first stroke more than 3 months before recruitment: disease duration was defined as the time from stroke onset to rehabilitation admission and ranged from 3 to 60 months (mean 39.1 months). Four of these participants had a right hemiparesis and eight patients a left.
Main gait analysis parameters along assessment time points (A1: before treatment A, A2: after treatment A; B1: before treatment B, B2: after treatment B).
The results obtained in terms of clinical and functional tests are reported in Table 1. Selective trunk muscle training (Treatment cycle B) demonstrated quite higher effect on trunk control respect the traditional rehabilitative program (Treatment cycle A) (TIS: + 12.7% after Treatment cycle B vs. + 7.6% after Treatment cycle A), on balance (BBS: + 6.3% after Treatment cycle B vs. + 5.3 after Treatment cycle A) and on walking test (10 MWT: –25.9% after Treatment cycle B vs. –13.8% after Treatment cycle A). In addition, the improvement in functional ability was higher after Treatment cycle B than after Treatment cycle A as demonstrated by FIM scores (FIM total score: + 6.2% after Treatment cycle B vs. + 4.9% after Treatment cycle A; FIM motor score: + 10.7% after Treatment cycle B vs + 6.8% after Treatment cycle A).
Mean values and standard deviations of clinical and functional scores (TIS, BBS, FIM and 10 MWT) for the two Treatment cycles (Treatment cycle A and Treatment cycle B) in the evaluated sessions and % variation (Var%) between pre and post session. *= p < 0.05, pre vs. post session (T0 vs. T1 and T2 vs. T3)
Mean values and standard deviations of clinical and functional scores (TIS, BBS, FIM and 10 MWT) for the two Treatment cycles (Treatment cycle A and Treatment cycle B) in the evaluated sessions and % variation (Var%) between pre and post session. *= p < 0.05, pre vs. post session (T0 vs. T1 and T2 vs. T3)
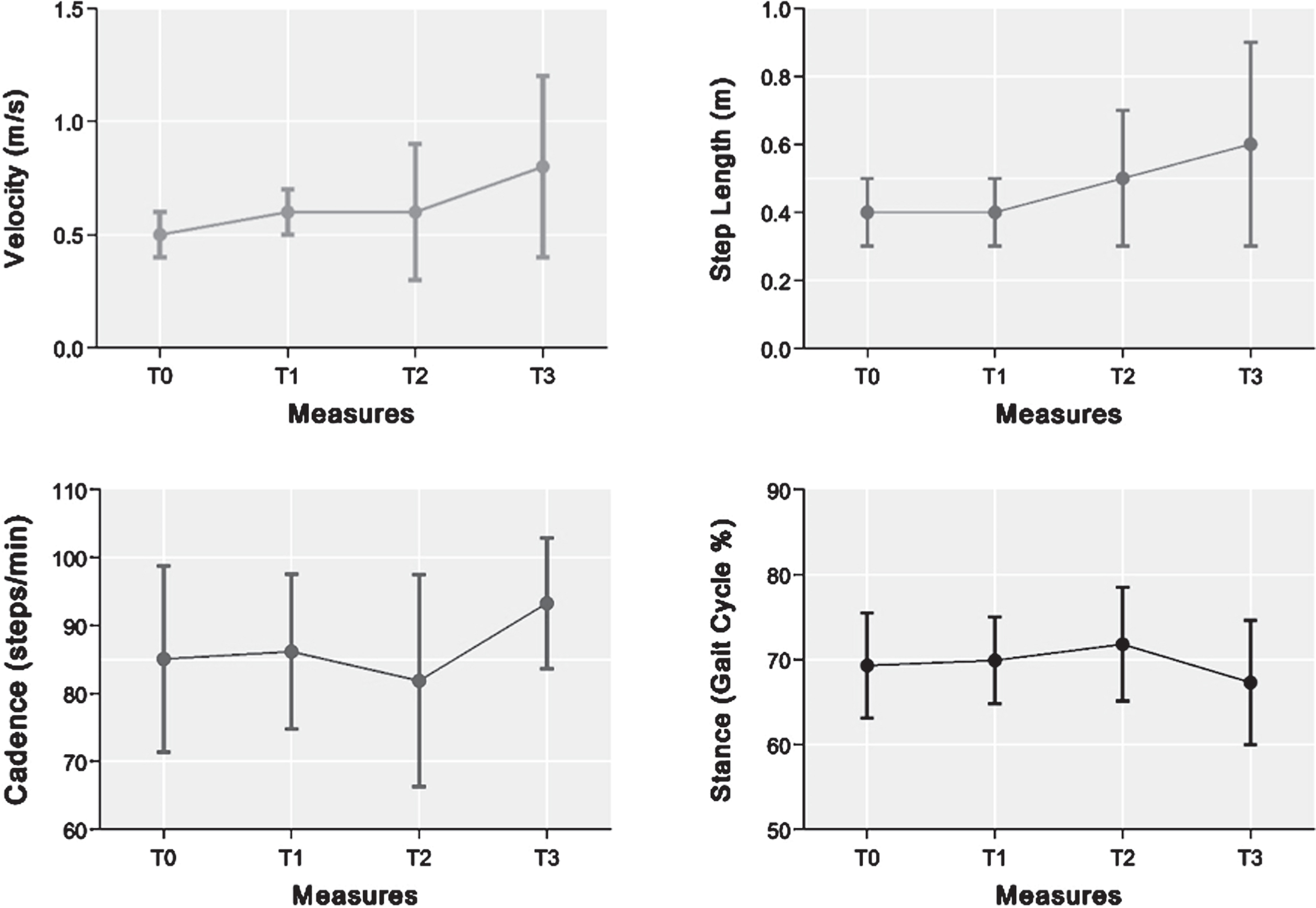
In Table 2, the mean values (standard deviation) of spatio-temporal parameters in all the sessions (T0, T1, T2 and T3) and for CG are reported. At baseline (T0 and T2), no statistical differences were detected. At baseline (T0 and T2 session) the patients’ performances were characterized by spatio-temporal parameters different if compared to CG. They exhibited significantly shorter step length, lower walking velocity and cadence, in comparison with CG.
After the Treatment cycle A, no changes occurred (T0 vs. T1); on the contrary, after Treatment cycle B, statistical improvement was observed in terms of all spatio-temporal parameters (T2 vs. T3).
Spatio-temporal parameters (mean and standard deviation) for the two Treatment cycles (Treatment cycle A and Treatment cycle B) in the evaluated sessions and for the Control Group (CG) *= p < 0.05, pre vs. post session (T0 vs. T1 and T2 vs. T3);+ = p < 0.05, if compared to CG
Spatio-temporal parameters (mean and standard deviation) for the two Treatment cycles (Treatment cycle A and Treatment cycle B) in the evaluated sessions and for the Control Group (CG) *= p < 0.05, pre vs. post session (T0 vs. T1 and T2 vs. T3);+ = p < 0.05, if compared to CG
After stroke, many patient’s loss the automatic postural responses which adversely affect both sitting and standing balance (Van Criekinge et al., 2019). Both trunk and limb muscles are involved in the coordination and regulation of automatic postural responses (Franchignoni et al., 1997), but despite this, training to restore trunk control is not yet included in most rehabilitation programs, the tendency being to concentrate on the more obvious arm and leg impairments. In addition, a precise description of the used exercise techniques is also lacking in published papers.
Although hemiparesis affects primarily unilateral limb activity, trunk muscle activity is also impaired during movements in different directions. A study has reported weakness of both trunk flexors and extensors (Van Criekinge et al., 2019). Trunk muscle clinical evaluation reveal some difficulty in such cases (for example sitting up from laying particularly with the rotation of the trunk) which can be confirmed by instrumental examination to reveal the true nature of true problems. Karatas et al. (2004) with isometric and isokinetic measurements observed peak torque values for trunk flexion and extension were lower in the stroke patients than in the controls. The differences were significant in both groups, peak torque values for trunk flexors were greater than peak torque values for trunk extensors. There was a significant positive correlation between trunk muscle strength and the Berg balance scale score at discharge.
Different authors investigated the reasons for the trunk muscle weakness in hemiparetic patients (Karatas et al., 2004; Dean et al., 1997; Pereira et al., 2011), also taking in consideration that the nerve supply to the trunk muscles comes from the motor cortex of both hemispheres. Insufficient recruitment of high-threshold motor units is another possible explanation for poor muscle contraction, especially in high angular velocities, also to be considered as muscle weakness caused by disuse. Trunk muscle weakness caused by disuse was another possible mechanism according to Tanaka et al. (1998). Conversely, Karatas at al. (2004) demonstrated that weakness could occur quickly after immobilisation with an isokinetic evaluation, arguing that the disuse probably is not the prominent cause. Another fact to be considered is that abdominals do not have origin and insertion from bone to bone. Thus, the muscles on both sides are affected because no stable insertion is offered by the central aponeurosis.
Due to the loss of activity in the abdominals, the patient uses his residual activity to move at all namely the primitive extension of his trunk which returns relatively soon. This is a possible explanation to the findings of Dickstein about the different activity between trunk extensors and flexors. The back extensors are therefore in a constant state of activity or even hyperactivity. As a result, abdominal muscle activity is not stimulated and possibly a reciprocal inhibition of antagonists occurs. The condition is self-reinforcing and can be observed many years post-stroke if the patient does not receive specific training. Due to the relatively fixed joint between the heads of the ribs and the vertebral column, when the thoracic spine extends, the necks of the ribs are depressed simultaneously. The elevation of the anterior rib-cage is magnified because of the long lever arm formed by the rib shafts. The abdominals are therefore in a constant state of elongation.
When considering the predictive significance of balance on functional outcome in stroke patients, it becomes clear that loss of trunk muscle activity might be related to functional disability and a selective trunk muscle training should therefore be included as part of the rehabilitation program. Re-establishing trunk muscle function improves stability in upright positions, facilitate the re-education of limb muscles and helps the patient to manage the activities of daily living more easily. Verheyden et al. (2004) demonstrated an improvement in the performance of the activities of daily living after specific training for selective trunk activity. Other studies have reported that trunk muscles control affect more lateral balance performance than antero-posterior one. According to those findings, additional trunk muscles training has shown strongest association whit Berg Balance Scale improvement (Winzeler-Merçay et al., 2002).
Significant improvement after Treatment cycle B were found in terms of the spatio-temporal parameters obtained through GA: after Treatment cycle B, velocity, step length, cadence and stance phase duration revealed statistical improvements, while after Treatment cycle A no variations were observed. In addition, a precise description of the types of muscle exercises and interventions is provided to help an ideal process of standardization of rehabilitative techniques.
The results of this study showed that some improvements are observed after conventional rehabilitation but more significant improvements are obtained after a specific training of the selective activity of the muscles of the trunk (Treatment cycle B). According to these results, it seems crucial in these patients to regain good trunk control for maintaining balance while sitting and standing, and that it is also necessary for functional activities such as transferring, reaching for objects, and walking safely. The key to successful treatment and rehabilitation outcome lies in regaining dynamic adaptive stabilization of the trunk, and the ability to move part of it in isolation. Re-establishing trunk muscle activity improves stability and makes the re-education of limb function easier. The patient may even be able to use the recovering activity in his arm for functional tasks of increasing complexity. He may discard his cane voluntarily as his balance improves and he is less afraid of falling. Likewise, the patient could be better able to manage daily living activities as were the patients in the study, according to the FIM results.
This study has some limitations. The small number of participants resulted in the limited strength of the clinical and statistical findings. Furthermore, it would be important to extend this rehabilitative treatment for acute/subacute patients with a long follow up particularly aimed at assessing the maintenance of their walking ability and independence. There are many conflicting opinions as to the most effective treatment for regaining good control of the trunk for hemiparetic patients, for example exercises performed on a gymnastic ball (Lee et al., 2014), shifting weight on an unstable surface, proprioceptive neuromuscular facilitation (PNF), using anterior elevation and posterior depression of pelvic movements for the lower trunk muscles; sling exercise therapy (Cirstea et al., 2000) and still Lee et al (2020) shows that selective abdominal muscles activation has beneficial effects on abdominal muscles, equilibrium and mobility.
A previous study had shown that “the balance ability of stroke patients is related to trunk intersegmental movement (Mudie et al., 2002); the authors emphasized that exercises need to restore the selective trunk activity in order to achieve a significant difference in improvement between groups. The study also explained how different results depends on intervention time, and the ability to detect these results depends on measurement tools, and/or measured items: literature confirms that muscle activity measured using EMG exhibits early changes within several days after intervention due to neural adaptation (Dickstein et al., 2004). Specific studies are needed not only on strength measures but also on the quality of the trunk muscles recovery and this opens up new and interesting insight into the treatment of chronic patients. This is could be important especially for those cases when the therapist believes that’s no longer to achieve further progress and the patient is not satisfied by his progress during and after conventional treatment.
Footnotes
Acknowledgments
The author address a special thanks to Patricia M. Davies who first recognized the importance of the trunk control in rehabilitation. LV would furthermore like to thank the PhD Programme in Experimental Medicine and Therapy of University of Turin.
Conflict of interest
The authors declare that there is no conflict of interest.