
Abstract
BACKGROUND:
After a stroke, patients experience sensorimotor damage, balance disorders, loss of selective movement, hypotonia and/or hypertonia, and hypersensitivity, all of which affect gait.
OBJECTIVE:
The aim of the study was to establish the effectiveness of Bobath therapy with additional specific soft tissue mobilizations versus standard Bobath intervention.
METHODS:
Subjects were randomly divided into two groups (S1 and S2) of 20 people each. Both groups underwent the same intervention (Bobath concept) over a 5-week period, while the second study group (S2) also received additional, specific soft tissue mobilization. The Berg Balance Scale (BBS), Timed Up and Go Test (TUGT), Active Range of Motion (AROM) of dorsiflexion and knee flexion and extension were used as clinical variables to assess the efficacy of therapy modalities. Data was analysed using a mixed model ANOVA.
RESULTS:
A significant interaction of group and time was found. The experimental (S2) group had a larger improvement of balance and AROM than the control (S1) group. There was no clear advantage of one group over the other for TUGT.
CONCLUSION:
The findings demonstrate that a combination of Bobath treatment and additional specific soft tissue mobilizations are more effective in increasing AROM and balance and mobility.
Introduction
Stable gait can be defined as one that does not lead to a fall and requires control of the position of the center of mass (CoM) relative to the base of the support (BoS). A disadvantage of human gait is that a relatively large share of the body weight is positioned over a relatively small base of support, and thus even the slightest deviation from perfect body orientation can lead to a displacement of the center of mass from the base of support, resulting in a fall (Bruijn & Van Dieen, 2018).
Gait pattern after a stroke includes increased postural sway and instability, most frequently in the frontal plane (Haart et al., 2004) and greater visual dependence while controlling postural sway in the medial-lateral direction (Marigold & Eng, 2006). According to Tyson et al. (Tyson et al., 2006), stronger postural sway occurs due to a smaller weight shift and a shorter time of weight shifting to the weaker leg.
In the case of a hypotonic leg, the gait of a stroke patient is characterized by inadequate activity of the leg in weight shift onto the affected leg, and a sway when stepping forward. It also affects forward propulsion of the CoM causing an asymmetrical gait pattern and reduced gait speed (Allen et al., 2014). The same changes are seen if the affected leg is hypertonic. The hypertonic leg shows signs of mass spastic extension of the plantar flexors and supinators of the foot. Gait in patients with hemiplegia or hemiparesis leads to burdening of various parts of the body, which requires increased energy consumption and causes fatigue (Gjelsvik & Syre, 2016).
The Bobath concept is based on plasticity (neural and muscle) that enables the patient to acquire new (old) skills simultaneously with the recovery of the central nervous system (CNS) recovery. Changes in plasticity occur as a result of sensorimotor training of meaningful tasks to the best of the ability of the damaged CNS (Kes et al., 2014).
Specific soft tissue mobilization (STM) is an integral part of the Bobath concept. This is a manual technique that aims to improve the mobility of joints and soft tissues (muscles, tendons, joint capsules and ligaments), establish better alignment of body structures, and improve circulation. This tends to cause positive changes in the metabolism, structure and function of the musculature (Gjelsvik & Syre, 2016). This technique is used to achieve better muscle length and elasticity, and it places the treated muscles in a more optimal alignment in relation to the closest joints and segments. Mobility is achieved by translating muscle(s) position in relation to other muscles, muscle groups, bone, and joint structures. Muscle elongation and elasticity is achieved by the manual elongation technique. Treatment is combined with alignment correction and leads to functional movement or integration into functional activity (Raine et al., 2009). Specific mobilization of the musculature and correction of “alignment” allows the patient to achieve tone normalization the recovery of the central nervous system (CNS) and a better starting position for motor control. Through therapeutic guidance, the patient receives normal, i.e., corrected information about the relationship between different parts of the body, and between the body and the environment, providing a better basis for achieving the therapeutic goal. At the same time, good information and stimulation in the patient can cause a sense of recognition of movement, activity, or function. Multisensory inputs such as proprioception and tactile sensation also influence the formation of the body schema (Naito et al., 2016). All this information allows the parts of the CNS responsible for motor planning and execution to generate and control the movement (Gjelsvik & Syre, 2016). To our knowledge, there are no randomized clinical trials that compared Bobath therapy and Bobath therapy with additional specific mobilizations.
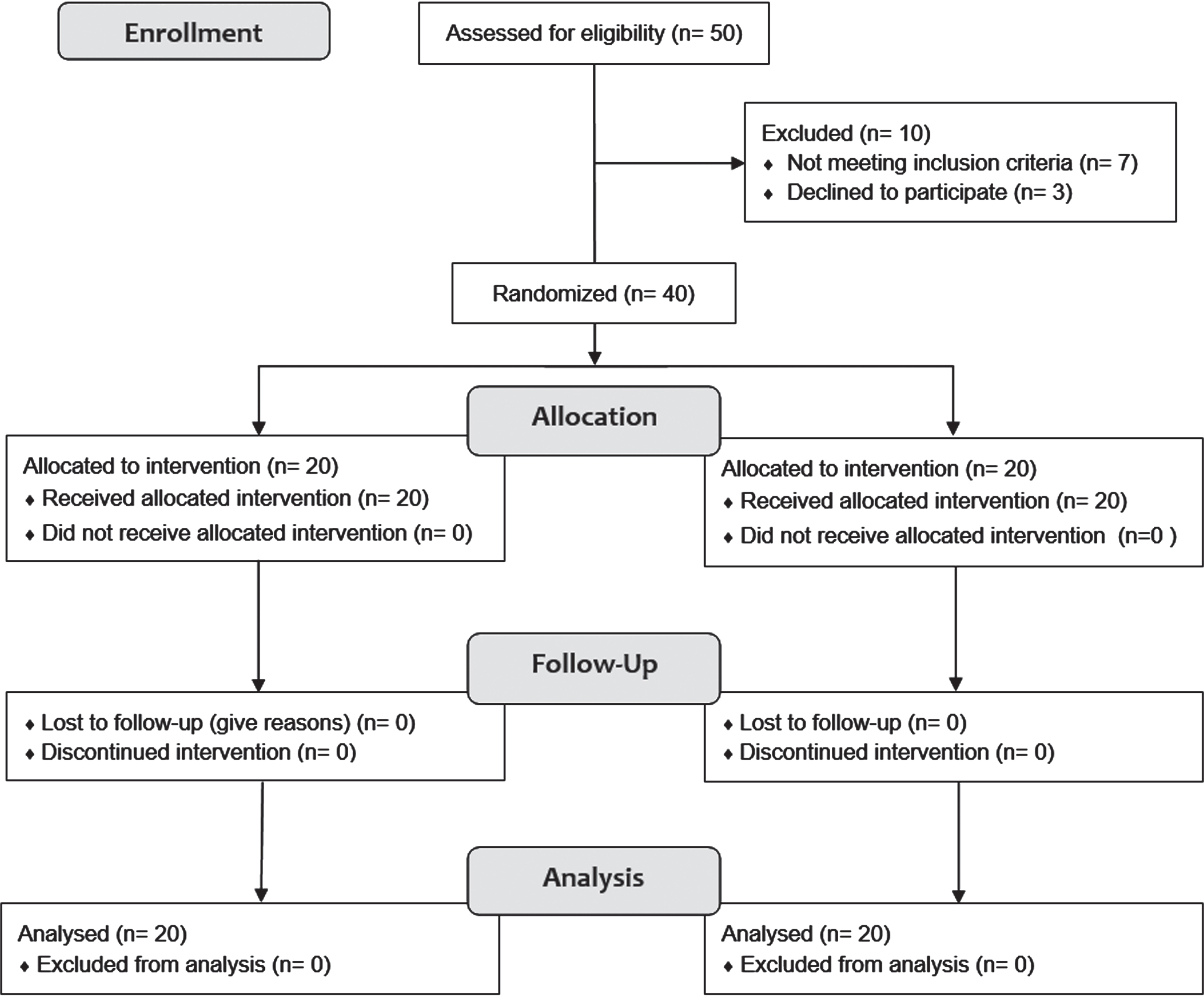
Flowchart of the study (from CONSORT, 2010).
Design and recruitment
The aim of this study is to evaluate the effectiveness of including additional specific soft tissue mobilizations to standard Bobath treatment on balance and gait in stroke patients. The study was designed as a two-arm, randomized clinical trial to compare the effectiveness of two therapy modalities – standard Bobath treatment versus standard Bobath treatment with additional specific soft tissue mobilizations. All participants signed an informed consent form to take part in the study, which was approved by the Ethics Committee of Krapinske Toplice Special Hospital for Medical Rehabilitation.
Patients were recruited from Krapinske Toplice Special Hospital for Medical Rehabilitation. Inclusion criteria were: patients aged 18 to 75 years and diagnosed with stroke in the previous 3 months, and grade 3 hemiparesis according to the Medical Research Council scale (Gregson et al., 2000).
Patients suffering from mental or cognitive disorders, or those with a serious dysphasia or aphasia, were excluded from the study. Though the clinical trial planned for a total of 50 subjects, only 40 subjects were randomized since 7 subjects did not meet the inclusion criteria (due to comorbidities, including hypertension, diabetes, or other neurodegenerative diseases or due to a recurrent stroke in anamnesis) while 3 subjects declined to participate.
Figure 1 shows the study flowchart. No participants were lost to follow-up measurement.
Randomization and blinding
Participants were randomized off-site using the block randomization method and allocated to groups after they agreed to participate in the study. The researcher recruiting the participants did not know to which group participants would be allocated. The opaque envelopes containing group allocation were opened only after the participant was recruited. Therapists and patients were not blinded to group allocation.
Experimental and control group
The Bobath group (S1) underwent a 45-minute Bobath treatment 5 times a week over 5 weeks, whereas the Bobath with specific tissue mobilization group (S2) underwent the same treatment program, with an additional 20-minute treatment of specific soft tissue mobilizations 3 times a week over 5 weeks applied to specific muscles and tendon structures, such as the soleus muscle, medial head of the gastrocnemius and long tibialis extensors which are essential for the preparation of gait function.
Clinical measurements
Balance was assessed according to the Berg Balance Scale (BBS), gait function by the Timed Up and Go Test (TUGT), and active knee flexion and extension and foot extension by the Active Range of Motion (AROM).
The Berg Balance Scale (BBS) assesses balance based on the completion of 14 functional tasks, each scored from 0 to 4 for a maximum score of 56. It is a valid instrument for the assessment of static and dynamic balance treatments indicating a high, moderate or low fall risk (Berg et al., 1995). A retest conducted on subjects with hemiparesis showed high reliability of the test (Bland et al., 2012).
The Timed Up and Go Test (TUGT) registers levels of activity including static and dynamic balance (Podsiadlo & Richardson, 1991). Results are shown in seconds and the results indicate subject mobility level with a low, moderate and high fall risk (Chou et al., 2006).
The Active Range of Motion Test (AROM) assesses the range of active joint movement to determine the active movements of the joint and soft tissues needed to walk. Active knee flexion and extension and foot extension were measured according to standardized procedures (Norkin & White, 2016).
All outcomes were assessed at the beginning of the study, after randomization, and at the end of the 5-week intervention period.
Statistical analysis
Statistical analysis was conducted using R Statistical Software (version 4.1.2). Differences in demographic characteristics between groups were tested by the Chi-Square test, Student’s t-test and Mann-Whitney U test, as appropriate. Data was analyzed using a mixed model ANOVA after the assumptions of variance homogeneity, normality of residuals and lack of outliers were assessed. Partial eta squared was calculated as the measure of the effect size. Type I error probability was set to 5%.
Results
Table 1 shows the comparisons of basic subject demographic parameters between groups where no statistically significant differences were found. Table 2 presents the means and standard deviations of the descriptive clinical parameters.
Descriptive demographic parameters
Descriptive demographic parameters
Descriptive clinical parameters
Legend: Df – dorsiflexion; Fl – flexion; Ex – extension; TUGT – Timed Up and Go Test; BBS – Berg Balance Score.
According to the calculations in Table 3, TUGT was the only variable that showed no statistically significant interaction (F(1,38) = 3.628; p = 0.064). However the main effect of time was statistically significant (F(1,38) = 59.51; p < 0.001), demonstrating that both therapies were effective in improving walking speed.
Mixed model ANOVA (df = 1.38)
Legend: F – F ratio;
The interaction effect between groups and time was statistically significant for all other variables: ankle dorsiflexion, knee flexion, knee extension and the Berg Balance Score. According to Cohen’s interpretation (Cohen, 1973), the effect size for knee flexion and knee extension was moderate (0.11 and 0.12, respectively), while for ankle dorsiflexion and BBS the effect size was large (0.19 and 0.15, respectively). Interaction plots of statistically significant models are shown in Fig. 2. Figure 2 shows that all cases combining Bobath treatment with additional specific soft tissue mobilizations had a higher impact on improving ankle dorsiflexion, knee flexion and extension, and balance.
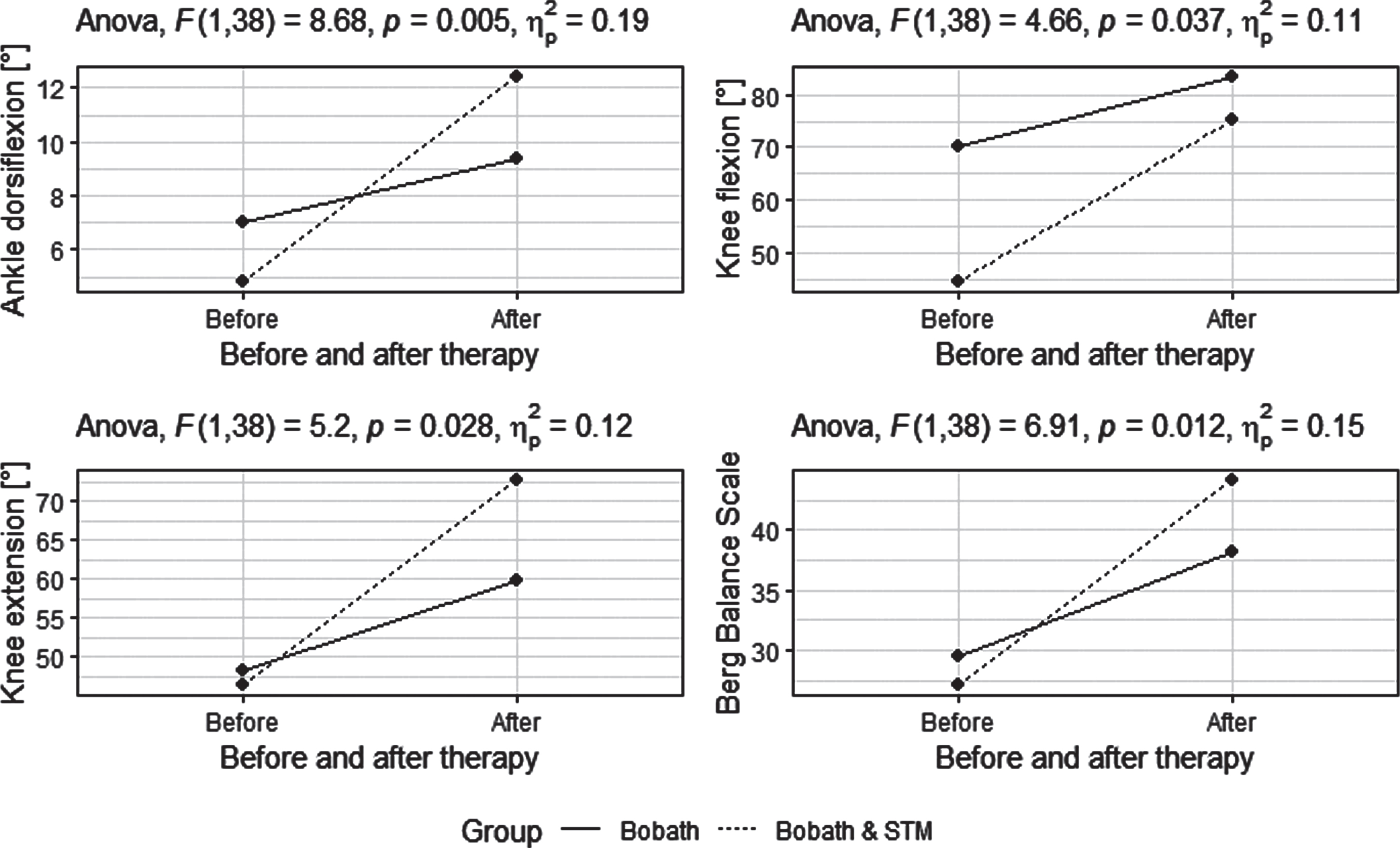
Four interaction plots of statistically significant models.
The differences in therapeutic approach between the Bobath treatment and additional STM treatment are in the added time of giving proprioceptive and tactile information to the muscular system through STM. In Bobath therapy, balance and gait learning methods are implemented through sequential movement treatment, therapeutic guidance of upright posture, balance and gait activities. Using this approach, the therapist seeks to facilitate, control and guide balance and gait movement and activity using maximally normal patterns, which mainly involves tactile and proprioceptive guidance and motor control of movement (Graham et al., 2009). In STM, tactile and proprioceptive information was additionally focused on soft tissues, namely muscles and tendons that were, due to spastic hypertonus, in unfavorable position to perform normal selective movements of the feet and knees important for gait function.
STM treatment was based on manual muscle elongation. Providing new manual information to plantar flexors of the feet to relax and lengthen the treated muscles and Achilles tendon using the muscle plasticity phenomenon, affected the acquisition of adequate selective active foot dorsiflexion important for getting up, heel support and weight shifting on the soles while stepping forward, and consequently better balance and gait. By therapist placing their hands on the spastic muscle and providing it with proprioceptive and tactile information and elongating it, they directly affect muscle plasticity, changes in terms of stability and reduction of its activity and activate the inhibition reflex of the Golgi tendon organ. Stimulation of this inhibitory mechanism is considered responsible for better muscle elasticity and better active mobility of muscles responsible for selective movements in the knee and foot joints. The same treatment was applied to the lower leg extensors and flexors, which enabled better selective performance of knee flexion and extension and performance of normal movements. Improved range of motion of knee flexion and extension, and especially foot dorsiflexion, validate the contribution of additional treatment of specific soft tissue mobilizations, namely the lower leg extensor muscles, which make up the anterior thigh muscles, and plantar flexor muscles of the feet. Similarly, Richardson (Richardson, 2002) argues that specific physiotherapy treatments based on biomechanical and neurophysiological science are effective because of the focus of treatment on changes in muscle length, elasticity, and function.
Prevention of muscle shortening and development of contractures due to spasticity in persons after stroke should be the goal of neurophysiotherapy due to better functional outcomes for the patients, especially concerning gait function. Improved range of motion results in better selective motor control of foot dorsiflexion as well as knee flexion and extension, which automatically reflects on better balance (Güçlü Gündüz et al., 2019) such as standing, getting up and sitting down and better-quality gait where the time from walking from one point to another is shortened, as our research has shown. Papers that show the effect of soft tissue mobilization performed by a therapist through direct manual intervention on spastic muscles were unfortunately not found, except in the case of one case study (Maček & Telebuh, 2008).
The mobilization technique presented in this paper is a basic part of a Bobath therapist’s training. The results of our study show that by providing longer therapy using specific tissue mobilizations, we can obtain better outcomes for patients who suffered a stroke. Even though both groups improved their balance at the end of therapy and better active mobility of movement in the joints, the experimental group had significantly better progress in balance, but also in walking ability. Static and dynamic balance depend on better active foot and knee range of motion, therefore, it is not surprising that with the improvement of the active range of motion of the knee and ankle, there was also an improvement in static and dynamic balance.
Although it is due to the knowledge that specific soft tissue mobilization (STM) puts the treated muscles in a more optimal alignment, it changes the body schema in the cortex (Gjelsvik & Syre, 2016; Limanowski & Blankenburg, 2016; Naito et al., 2016; Raine et al., 2009), which ultimately enables more adequate and better performance of movements and functions (Blanke, 2012), our research hypothesis was that additional STM therapy, through these mechanisms, will also affect gait speed. There was no statistically significant improvement in walking speed between the groups, although it is possible to observe a tendency to walk faster in the experimental group.
There are also studies that show a positive effect and the reduction of spasticity using different types of physiotherapeutic mechanical approaches that indirectly affect soft tissue, but do not show the specific soft tissue mobilization technique we used in the study (Castilho et al., 2012; Zhang et al., 2021).
The study we conducted confirms earlier results of related work in the field of foot spasticity treatment as a method for improving balance activities, passive and active movement and gait, and it is based on the theory of neural and muscle plasticity (Kes et al., 2014; Lieber et al., 2004; Vattanasilp et al., 2000). Consistent with the meta-analysis conducted by Lohse et al., 2014, the results of our study showed that increasing the duration of targeted STM treatment allows for better treatment effects. The importance of our research is reflected in a clearly structured protocol of clinical STM application, scientifically proven effectiveness in improving balance, active and passive knee and ankle range of motion, and thus, we can recommend the implementation of STM in clinical practice in people with foot spasticity problems with the aim of improving the range of motion, balance and gait.
The limitation of the research is a relatively small sample size and the impossibility to blind the therapists and patients. Moreover, even though increasing active range of motion is a likely cause of increased stability and contributes to gait speed, future research that measures the range of motion while walking using kinematic methods could be more informative about the relationship between range of motion and its functionality. Also, future studies should need to have a longer follow-up period to be able to make sure that the observed effect of additional, specific tissue mobilization persists for a longer period. Such research would help answer the question of whether, considering the therapeutic outcomes, it is worthwhile to spend additional time on mobilization.
Conclusion
The main aim of this study was to examine the effects of Bobath treatment in combination with additional treatment of specific soft tissue mobilizations on gait function in stroke patients with hemiparesis. Bobath treatment with an additional specific soft tissue mobilization had a larger positive effect on both static and dynamic balance as well as on active range of motion in knee and ankle compared to group that only underwent standard Bobath treatment. While the observed effect for balance was large statistically speaking, further studies, with larger sample size, should investigate whether the increase in balance was clinically relevant given the increased time the therapist spent administering additional treatment of specific soft tissue mobilizations.
Conflict of interest
None of the authors have any conflict of interest to report.