
Abstract
BACKGROUND:
Accurate prediction of recovery is essential to determine whether a knee-ankle-foot orthosis (KAFO) is required in the subacute phase of stroke. However, there are currently no reliable methods to predict such recovery.
OBJECTIVE:
This study aimed to determine whether muscle strength of the affected lower limb (affected side LL strength) in stroke patients in the subacute phase who cannot walk without a KAFO can be used to predict the continuous need for a KAFO, using a hand-held dynamometer.
METHODS:
We enrolled patients with severe hemiplegia (n = 51) who were unable to walk without a KAFO for 10 days after stroke onset. They were divided into two groups depending on the continuous need for a KAFO at 1 month after onset; the KAFO and non-KAFO groups. Logistic regression analysis was used to investigate whether the affected side LL strength was a predictor of the continuous need for a KAFO at 1 month after onset. In addition, significant predictors were analyzed using receiver operating characteristic (ROC) curves.
RESULTS:
The KAFO and non-KAFO groups included 23 (45.10%) and 28 (54.90%) patients, respectively. The affected side LL strength and pusher syndrome severity were identified as predictors of the continuous need for a KAFO. The predictor with the highest predictive ability was the affected side LL strength, with an area under the ROC curve of 0.80 (95% CI, 0.68–0.93).
CONCLUSIONS:
Affected side LL strength may be a highly accurate predictor of the need for a KAFO in the subacute phase of stroke.
Introduction
The mobility of many stroke survivors is limited (Jørgensen et al., 1995); therefore, regaining independence and safe mobility is a frequent goal of stroke rehabilitation. Previous systematic reviews have reported that leg orthoses improve leg kinematics, kinetics, and energy cost of walking in stroke patients (Tyson et al., 2013), as well as improve their walking ability (Tyson & Kent, 2013). Patients with severe hemiparesis especially require a knee-ankle-foot orthosis (KAFO), because such patients exhibit both ankle and knee instabilities (Boudarham et al., 2013; Kakurai & Akai, 1996; Maeshima et al., 2015; Ota et al., 2018; Yamanaka et ai., 2004).
Recently, some studies have reported the impact of gait training using a KAFO on patients with severe hemiplegia (Abe et al., 2021a; Abe et al., 2021b; Ota et al., 2018; Sato et al., 2022). One retrospective study reported that early use of a KAFO was associated with higher recovery of activities of daily living (Sato et al., 2022). One historical control study reported that gait function improved earlier in subjects who used a KAFO compared to those who did not (Abe et al., 2021b). In addition, a cross-sectional study by Sato et al. reported that standing balance improved when wearing a KAFO than when not wearing a KAFO in severe stroke patients (Ota et al., 2019). Abe et al. reported in a review article that physical therapy using an early-prescribed KAFO might be effective for improving walking and stair climbing functions in post-stroke patients with severe hemiparesis (Abe et al., 2021a). In Japan, walking training using a KAFO is recommended (Miyamoto et al., 2022), and many case reports have reported the therapeutic effect of a KAFO in stroke patients with regard to improvement in functional mobility and activities of daily living (ADL) (Kobayashi, et al., 2022).
A KAFO is typically custom-made for each patient to gain a good fitting. Moreover, a previous report revealed that early wearing of a prescribed custom-made KAFO accelerates the recovery of activities of daily living (Sato et al., 2022). In Japan, it takes approximately 2 weeks to make a KAFO following its prescription. Physicians and physical therapists must take this time period into account when prescribing a KAFO (Yamanaka et al., 2004), because many patients recover during the acute phase (Duncan et al., 1992). Some patients needed a KAFO initially, but no longer needed it after a very short period of time. If a patient with stroke hemiplegia achieves early function recovery, a KAFO will not be needed. Therefore, accurate prediction of recovery is essential to determine whether a KAFO is required in the subacute phase. However, there are currently no methods to predict such recovery.
Lower limb (LL) muscle strength is known as a parameter that can predict post-stroke walking ability with high accuracy, and hip extensor strength is a determining factor for long-term walking independence (Veerbeek, 2011). In addition, it has been reported that initial LL paralysis severity is a determining factor of the degree of a stroke individual’s future walking independence (Jørgensen, 1995). Additionally, a previous study reported that the knee extension strength/body weight ratio on the unaffected side on admission to a convalescent rehabilitation ward was associated with independent walking ability at discharge. (Hirano, 2016). Therefore, we hypothesized that, by quantitatively evaluating the LL muscle strength of the affected side by a hand-held dynamometer (HHD) (Cooper et al., 2012; Nollet & Beelen, 1999) in the acute phase of stroke, it is possible to accurately predict the walking ability in the subacute phase.
In the present study, we aimed to investigate whether LL muscle strength of the affected side of stroke patients, which was quantitatively evaluated using an HHD, could be used to predict the continuous need for a KAFO in the subacute period.
Materials and methods
Participants
A total of 2,061 patients with acute stroke who were admitted to Kohnan Hospital between 2015 and 2018 and were provided physiotherapy were enrolled in this study. Among them, we selected patients who were able to walk with a KAFO, but not with any type of cane, within 10 days of stroke onset. We then applied the following inclusion criteria: patients who were (1) unable to walk properly with an ankle-foot orthosis (AFO) because of severe knee instability, and (2) barely able to walk with an AFO because of gait abnormalities (De Quervain et al., 1996) such as buckling-knee pattern (BKP), extension thrust pattern (ETP), or stiff-knee pattern (SKP), on day 10 following stroke onset. Among the 2,061 patients, 51 were determined to be eligible (Fig. 1) and underwent the same clinical assessment twice. The first and second assessments were performed on day 10 (acute phase) and at 1 month after stroke (subacute phase), respectively. Participant selection was based on daily clinical information obtained by physical therapists.
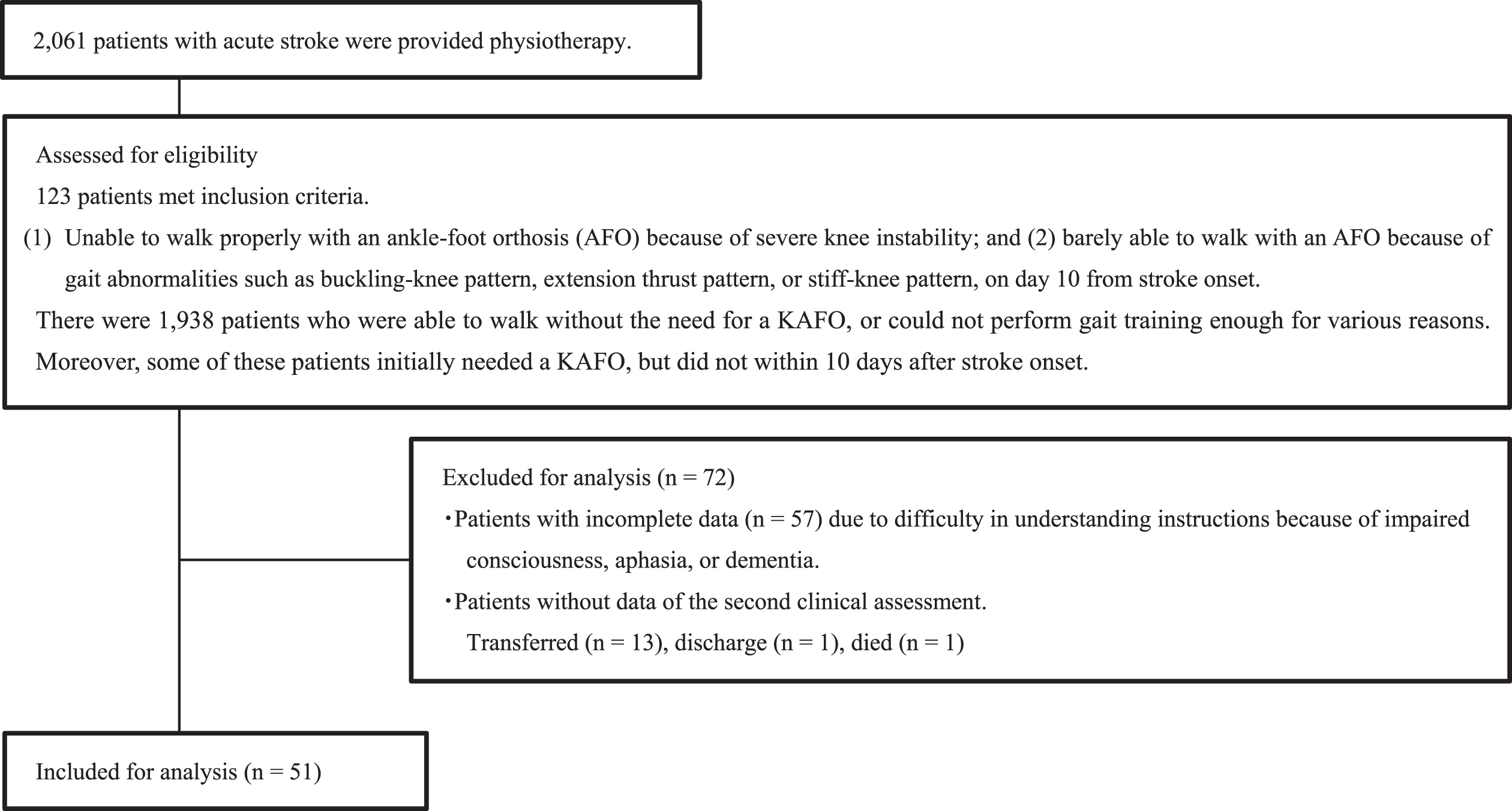
Flowchart of inclusion criteria.
All procedures were approved by the local ethics committee of Kohnan Hospital and were in accordance with the Declaration of Helsinki. Written informed consent was obtained from all patients prior to their participation in this study.
We provided rehabilitation in accordance with the Japan Stroke Society Guideline 2021 for the Treatment of Stroke (Miyamoto et al., 2022). All subjects typically received one hour of individualized physiotherapy per day, five days per week. The therapists continually made decisions regarding therapy type and dose for each patient based on their clinical judgement and service capacity. The subjects receive conventional rehabilitation that included not only physical therapy (PT), but also occupational therapy (OT) and speech therapy (ST). In cases where the general condition of the patient was unstable, PT was started from bedside and included range-of-motion, sitting, and standing exercises. If permitted by the patient’s general condition, exercises for transfer maneuvers such as walking and stair climbing were performed incrementally. OT included ADL (referring to daily self-care activities) training and arm exercises. ST included exercises for dysphagia and aphasia.
Clinical assessment
For the analysis, we collected demographic data including age, gender, stroke type, lesion side, stroke recurrence, and body mass index at admission, as well as Functional Ambulation Category (Holden et al., 1984) before admission.
Using an HHD (SAKAI Medical Co., Ltd.; mobie MT-100), we measured the muscle strength of the hip flexor of the affected side (HHD-AH) and non-affected side (HHD-NH); the knee extensor of the affected side (HHD-AK) and non-affected side (HHD-NK); the ankle dorsiflexor of the affected side (HHD-AAD) and non-affected side (HHD-NAD); and the ankle plantar flexor of the affected side (HHD-AAP) and non-affected side (HHD-NAP). Isometric bilateral muscle strength was measured at maximal effort for 5 seconds, three times, with intervals of at least 30 seconds between measurements. Each muscle action was measured in a gravity-neutralized position. HHD-AH, HHD-NH, HHD-AK, and HHD-NK were measured with the subjects sitting in a chair with their knee joints angled at 90°. HHDAAD, HHD-NAD, HHD-AAP, and HHD-NAP were measured with the subjects lying on a treatment bed (Fig. 2).
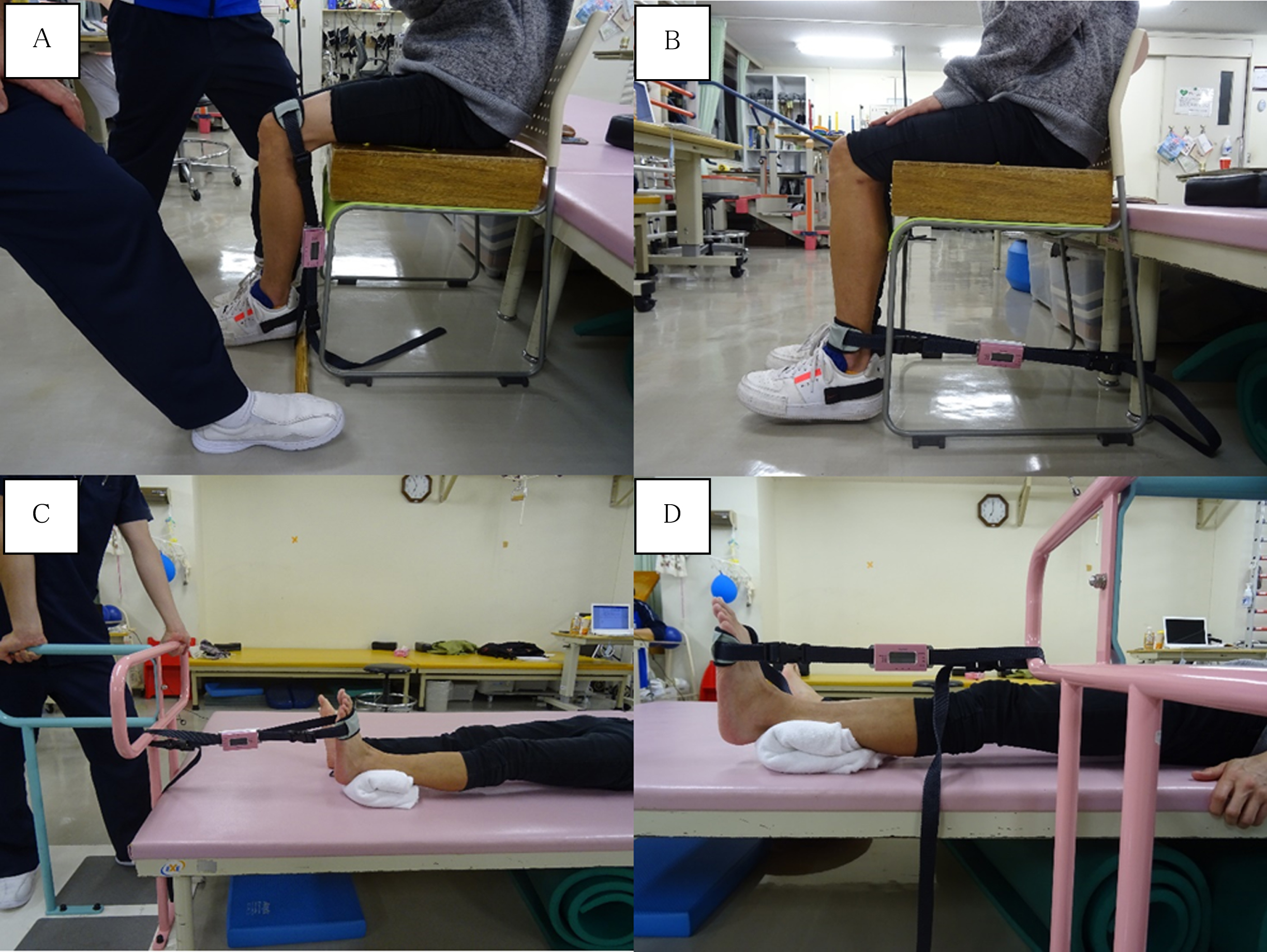
Evaluation of bilateral lower limb strength using an HHD: hip flexor, knee extensor, ankle plantar flexor, and ankle dorsiflexor. The force pad of the HHD was held perpendicular to the limb segment, and the HHD sensor was fastened to the distal part of the lower leg by using a hook-and-loop fastener. The subjects were instructed to push against the dynamometer with maximal force for 5 seconds. The desired movement was demonstrated to the participants, and their understanding was confirmed before starting. The evaluation was performed in the unaffected lower limb, followed by the affected lower limb. All measurements were obtained after practice and prior orientation. Each measurement was performed three times, with a short rest between measurements, on the same day. (A) For HHD-AH and HHD-NH, the subjects sat in a hard chair with their hips and knees flexed to 90°, and the examiner then fastened the HHD belt to their thigh just proximal to the patella. (B) For HHD-AK and HHD-NK, the subjects sat in a hard chair, the same as that used for the measurement of HHD-AH and HHD-NH, and then the examiner fastened the HHD belt to their lower leg just proximal to the lateral malleolus. (C) For HHD-AAD and HHD-NAD, the subjects lay in the supine position on the treatment table with the hips and knees at 0°, and then the examiner fixed their ankle at 0° and fastened the HHD belt to the dorsum of the foot just proximal to the toes. (D) For HHD-AAP and HHD-NAP, the subjects also lay in the supine position, the same as that for measurement of HHD-AAD and HHD-NAD, and then the examiner fastened the HHD belt to their sole, just proximal to the toes.
Peak force values (kg) were used in all trials. To normalize the affected side’s muscle strength, we calculated the ratios of muscle strength, which were done by dividing the strength of the affected side by that of the unaffected side, then multiplying by 100. Similarly, we multiplying by 100, and defined them as NormHHD-AH, NormHHD-AK, NormHHD-AAD, and NormHHD-AAP.
In addition, the degree of motor function recovery was evaluated using the Brunnstrom recovery stage (Brunnstrom 1966) (BRS). We scored both patellar and Achilles tendon reflexes (1, absent; 2, diminished; 3, normal; 4, slightly exaggerated; 5, moderately exaggerated; and 6, markedly exaggerated), as well as the spasticity of both the ankle joint plantar flexion and knee joint flexion using a modified Ashworth Scale (MAS, 0, no increase in muscle tone; 1, slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end of the range of motion [ROM] when the affected part is moved in flexion or extension; 1.5, slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder [less than half] of the ROM; 2, more marked increase in muscle tone through most of the ROM, but the affected part is easily moved; 3, considerable increase in muscle tone, with difficulty in passive movement; and 4, rigidity of the affected part in flexion or extension) (Bohannon & Smith, 1987).
The assessment of sensation, visuospatial perception, aphasia, and pain was performed using the Stroke Impairment Assessment Set (SIAS) (Chino et al., 1994). Light touch sensation was checked on the dorsum of the foot (0, anesthesia; 1, severely or moderately decreased; 2, slightly decreased or subjectively decreased, or abnormal sensation is present; and 3, normal). To assess position sense, the great toe of the affected side was used (0, passive movement in a full range of motion is not recognized; 1, passive movement in all directions is recognized; 2, passive movement in greater than 50% of all directions is recognized; and 3, passive movement in less than 50% of all directions is recognized). To assess unilateral spatial neglect, we used visuospatial perception in the SIAS, in which the patient was asked to touch the center of a tape held horizontally in front of the patient at a distance of about 50 cm, with the tips of the thumb and index finger of the non-affected side. Two trials were conducted and the larger deviation was used for scoring (0, deviation≥15 cm; 1, deviation between 15 and 5 cm; 2, deviation between 5 and 3 cm; and 3, deviation < 3 cm). Aphasia was rated by evaluating both expression and comprehension, not including dysarthria (0, total or global aphasia, practical communication is impossible; 1, severe sensory aphasia, severe mixed aphasia, and severe motor aphasia; 2, moderate aphasia; and 3, no aphasia). Whether the patients experienced pain that interfered with their gait was also investigated (presence/absence) using the SIAS (Chino et al., 1994).
The Clinical Assessment Scale for Contraversive Pushing (SCP) was used to assess pusher syndrome (PS) severity (Babyar et al., 2009; Karnath et al., 2000). As higher SCP score indicates higher severity, we converted the SCP score to a negative value in order to run ROC analysis and expressed it as “SCP reverse”. The Trunk Control Test (TCT) was used to assess trunk function (Collin & Wade, 1990; Franchignoni et al., 1997). Knee instability was evaluated by measuring the knee joint angle during single-leg standing on the affected side with reference to the Gait Assessment and Intervention Tool (Daly et al., 2009), which is usually an index to evaluate the stability while walking. The measured knee joint angle was scored 1–5 as follows: 1, flexion of≥30°; 2, extension thrust (hyperextension); 3, flexion between 15° and 30°; 4, flexion between 5° and 15°; and 5, normal (Fig. 3). The total duration of standing exercise (min), and total walking distance (m) in one physical therapy intervention were also measured. Furthermore, the presence or absence of corticospinal tract injury was visually evaluated using conventional brain computed tomography or magnetic resonance imaging.
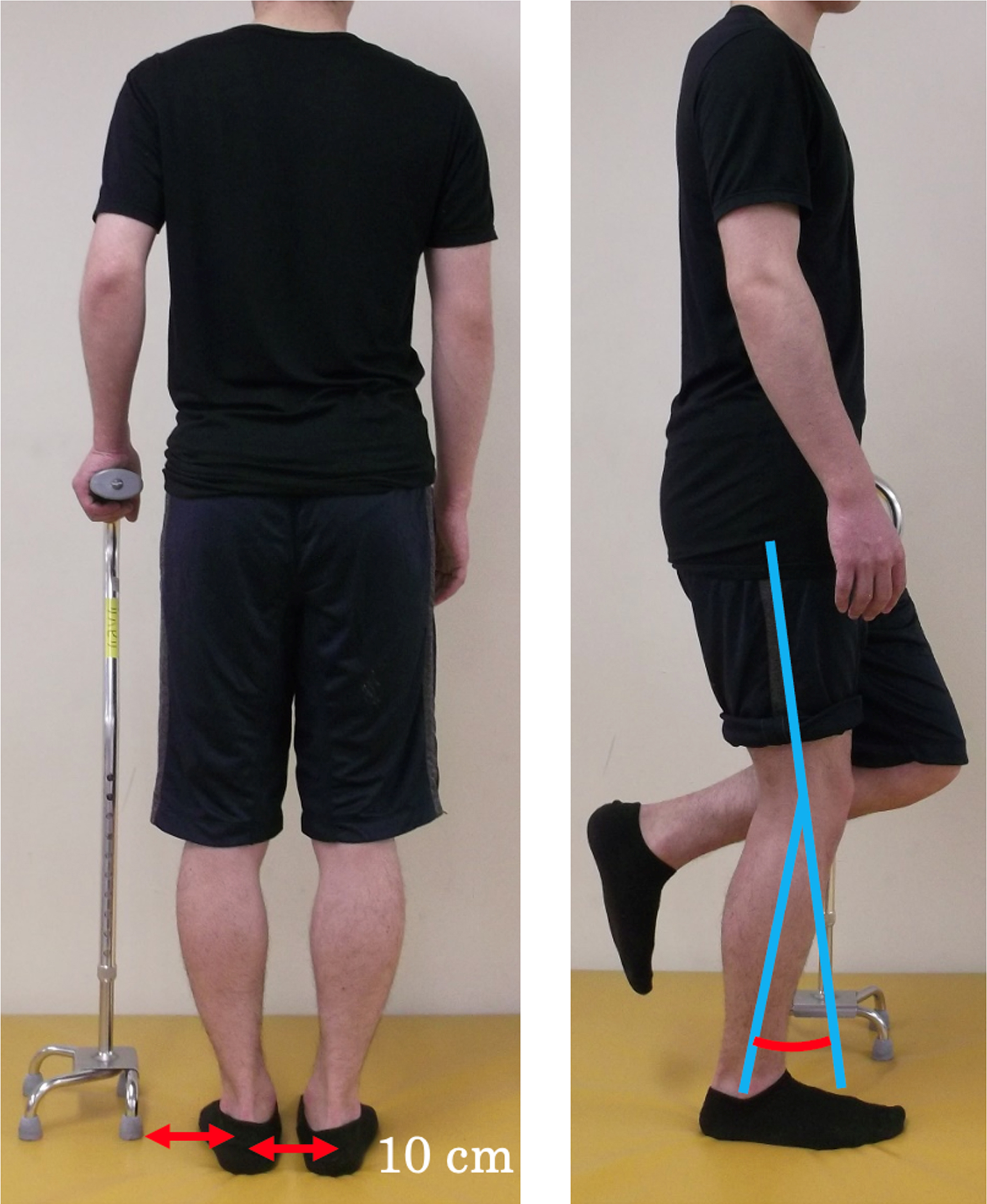
Method of measuring knee instability. The photographs show a case of right hemiplegia. The subject stood in as upright a position as possible using a 4-point cane. The distance between the heels and the distance from the non-paretic side heel to the cane were both set at 10 cm. We measured the angle of the knee joint while the patient stood on one leg.
When patients become able to walk without a KAFO via improvement in knee instability, gait training using an AFO is provided instead of a KAFO. However, if gait abnormalities such as ETP, BKP, and SKP are observed while walking using an AFO, we provide training using an AFO combined with a KAFO. We carefully assessed whether the patients were able to walk using an AFO without abnormalities, such as ETP, BKP, or SKP. Next, we divided the patients into two groups; the KAFO and non-KAFO groups. The non-KAFO group included patients whose total gait training time with an AFO accounted for more than half of the total gait training time at 1 month after stroke onset. The remaining patients were included in the KAFO group.
Statistical analysis
Before the analysis, all variables were assessed for normal distribution using the Shapiro– Wilk test (p < 0.05). Each variable was compared between the KAFO and non-KAFO groups using either the t-test or the Mann– Whitney U test, based on the results of the Shapiro– Wilk test. A chi-squared test was performed to analyze nominal variables. For multicollinearity, Spearman’s rank correlation among variables with significant differences was investigated; as a result, variables with a correlation coefficient of > 0.60 were detected. We constructed three binomial logistic regression analysis models. In the first and second models, we calculated odds ratios (ORs) and 95% confidence intervals (95% CIs) after controlling simultaneously for potential confounders. The first model was adjusted for age, and the second model was adjusted for age, gender, and stroke type. In the third model, a forward selection (likelihood ratio) logistic regression analysis was conducted to determine which variables could predict whether the patients would require a KAFO 1 month after stroke onset. In addition, among the significant predictors, diagnostic performance was assessed by analyzing the receiver operating characteristic (ROC) curve, which was a plot of sensitivity versus (1 – specificity) for all possible cut-off values. The probabilities of a true-positive (sensitivity) and a true-negative (specificity) were determined for selected cut-off values, and the area under the ROC curve (AUC) was calculated for each predictor with significance. The maximum Youden indices were considered the optimal cut-off values. All statistical analyses were performed using the IBM SPSS Statistics for Mac, Version 25.0 (International Business Machines Corporation, Armonk, New York, USA), and the significance level was set as 0.05.
Results
The number of participants assigned to the KAFO or non-KAFO group
The mean duration from stroke onset to the second clinical assessment was 30.96±1.92 days. Of the 51 participants, 23 (45.10%) were assigned to the KAFO group and 28 (54.90%) to the non-KAFO group.
Comparison of characteristics between the KAFO and non-KAFO groups
The mean duration from stroke onset to the first clinical assessment was 10.28±1.63 days. Results of the comparison of the initial demographic data and clinical assessment between the two groups are shown in Table 1. These results showed that BRS, HHD-AH, HHD-AK, HHD-AAD, HHD-AAP, NormHHD-AH, NormHHD-AK, NormHHD-AAD, NormHHD-AAP, position sense, TCT, knee instability, and walking distance were significantly greater in the non-KAFO group than in the KAFO group (p < 0.05). Moreover, SCP score was significantly lower in the non-KAFO group than in the KAFO group (p < 0.05).
Comparison of first clinical assessment between the KAFO and non-KAFO groups
Comparison of first clinical assessment between the KAFO and non-KAFO groups
Summary statistics are presented as mean±standard deviation (normally distributed characteristics), median [first quartile, third quartile] (characteristics with skewed data), or number (categorical data). *: Mann-Whitney U test was used to compare the differences between the KAFO and non-KAFO groups. **: Chi-square test was used to compare the differences between the KAFO and non-KAFO groups. ***: Independent t-test was used to compare the differences between the KAFO and non-KAFO groups. †: p < 0.05, ††: p < 0.01.
The results of Spearman’s correlation among variables with significant differences between the non-KAFO and KAFO groups are shown in Table 2. There were significant correlations between Achilles tendon reflex and patellar tendon reflex (Spearman’s correlation: rs, rs = 0.763, p < 0.01), between MAS of ankle planter flexion and MAS of knee flexion (rs = 0.795, p < 0.01), and between position sense and light touch sense (rs = 0.840, p < 0.01). Significant correlations were also found between BRS and HDD-AH (rs = 0.767, p < 0.01), HDD-AK (rs = 0.716, p < 0.01), HDD-AAD (rs = 0.754, p < 0.01), NormHDD-AH (rs = 0.790, p < 0.01), NormHDD-AK (rs = 0.786, p < 0.01), NormHDD-AAD (rs = 0.761, p < 0.01) and NormHDD-AAP (rs = 0.627, p < 0.01). Regarding TCT, significant correlations were observed between TCT and HDD-AK (rs = 0.638, p < 0.01) and NormHDD-AK (rs = 0.637, p < 0.01). A significant correlation was found between classification of knee instability and NormHDD-AH (rs = 0.606, p < 0.01). Significant correlations were also found between HDD-AH and HHD-AK (rs = 0.861, p < 0.01), HDD-AAP (rs = 0.667, p < 0.01), NormHDD-AH (rs = 0.923, p < 0.01), NormHDD-AK (rs = 0.749, p < 0.01), and NormHDD-AAP (rs = 0.610, p < 0.01). A significant correlation was found between HDD-AK and HDD-AAP (rs = 0.701, p < 0.01), HDD = NH (rs = 0.600, p < 0.01), NormHDD-AH (rs = 0.736, p < 0.01), NormHDD-AK (rs = 0.863, p < 0.01), and NormHDD-AAP (rs = 0.617, p < 0.01). Regarding HDD-AAD significant correlations were found with NormHDD-AH (rs = 0.608, p < 0.01), and NormHDD-AAD (rs = 0.980, p < 0.01).
Spearman’s correlation among variables with
Spearman’s correlation among variables with
*p < 0.05; **p < 0.01.
Regarding HDD-NH, significant correlations were found between HDD-NH and HDD-NK (rs = 0.710, p < 0.01), and HDD-NAD (rs = 0.678, p < 0.01). Significant correlations were also found between NormHDD-AH and NormHDD-AK (rs = 0.767, p < 0.01), and NormHDD-AAD (rs = 0.607, p < 0.01). Finally, significant correlations were found between NormHDD-AK and NormHDD-AAD (rs = 0.614, p < 0.01), and NormHDD-AAP (rs = 0.633, p < 0.01). There were no correlations among the other variables using Spearman’s correlation coefficient > 0.6.
The NormHHD-AK was used as a representative value because it had a strong correlation with the other three normalized HHDs on the affected side. It is appropriate to use NormHHD-AK, which indicates knee extensor strength, as a representative index value when evaluating the change from KAFO to AFO. The results of binominal logistic regression analysis are shown in Table 3. The first model revealed that the predictor for the continuous need for a KAFO was NormHHD-AK (OR, 1.05; 95% CI, 1.02–1.09; p < 0.001). The correct classification rate was 76.5%. The second model also revealed that the predictor for the continuous need for a KAFO was NormHHD-AK (OR, 1.05; 95% CI, 1.02–1.09; p < 0.001). The correct classification rate was 78.4%. According to the results of a univariate analysis and Spearman’s correlation coefficient, position sense, TCT, SCP, knee instability, and NormHHD-AK were selected as independent variables for a forward selection (likelihood ratio) logistic regression analysis. Although TCT showed a correlation with NormHHD-AK at 0.64, it was also included because there were differences in clinical significance between these evaluations. The third model revealed that the predictors for the continuous need for a KAFO were NormHHD-AK (OR, 1.04; 95% CI, 1.00–1.07; p < 0.005), and SCP (OR, 0.57; 95% CI, 0.37–0.89; p < 0.005). The correct classification rate was 84.0%.
Binominal logistic regression analysis
Binominal logistic regression analysis
Figure 4 shows ROC curves of NormHHD-AK and SCP reverse in the non-KAFO groups.
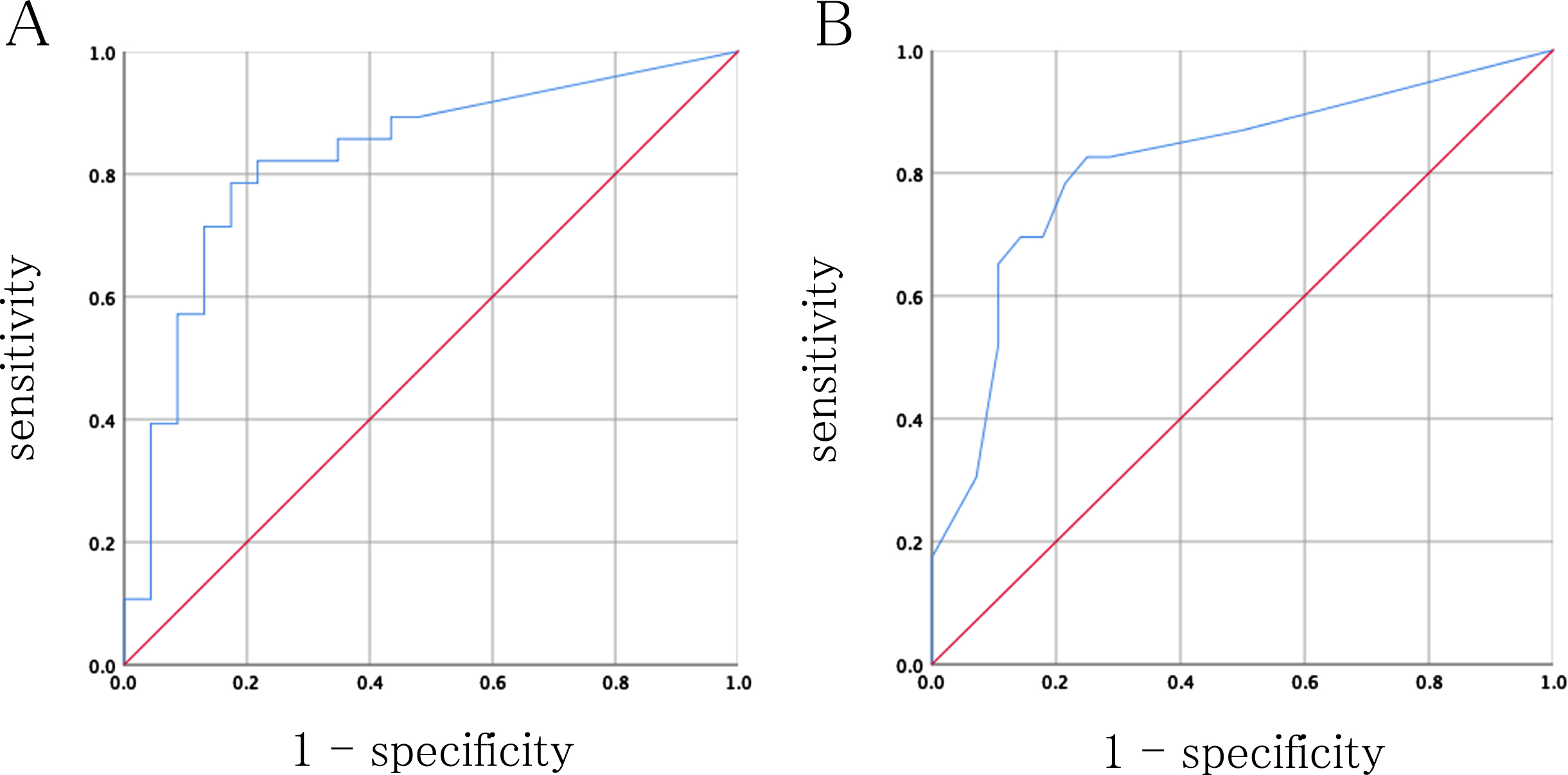
Receiver operating characteristic curve of the variables that predict the need for a KAFO in sub-acute period. A: normalized hand-held dynamometer value of the knee extensor strength on the affected side. B: value of Clinical Assessment Scale for Contraversive Pushing minus 6.
The AUC for NormHHD-AK was 0.80 (95% CI, 0.68–0.93), and the optimal cut-off value was 41.61 with a sensitivity and specificity of 0.68 and 0.91, respectively. The AUC for SCP reverse was 0.81 (95% CI, 0.69–0.94) and the optimal cut-off value was 0.88 with a sensitivity and specificity of 0.83 and 0.75, respectively.
The present study aimed to investigate whether the LL muscle strength of the affected side of stroke patients can predict the need for a KAFO at 1 month after onset. About half of the patients who required a KAFO on day 10 following stroke onset did not require a KAFO at 1 month after onset. Logistic regression analysis revealed that the predictors of the need for a KAFO were NormHHD-AK and SCP.
Walking ability of stroke individuals, assessment of which includes walking speed, stride length and walking independence is related to LL muscle strength (Akazawa et al., 2017; Bohannon, 2007; Watanabe et al., 2015). Watanabe et al. reported that paretic and nonparetic knee extension strengths were related to gait performance in inpatients with post-stroke hemiparesis (Watanabe, 2015), and Akazawa et al. reported that it is possible to determine the degree of walking independence by measuring knee extension muscle strength in chronic stroke patients (Akazawa, 2017). In a review article, Bohannon reported that knee extensor muscle strength was correlated with the independence in the sitting-to-standing motion independence in stand-pivot-sit transfer, maximum gait speed, comfortable gait speed, gait distance, gait independence, and stair ascent speed in stroke patients, showing an exceptionally higher correlation on the paralyzed side than the nonparalyzed side (Bohannon, 2007). Another previous study by Bohannon et al. investigated the relationship between walking independence 30 days after onset and all bilateral LL muscle strength (Bohannon, 1989). They reported that the highest correlation was found between affected side knee extensor muscle strength and gait performance (Bohannon, 1989). Patients with severe hemiparesis require a KAFO because such patients exhibit both ankle and knee instabilities (Boudarham et al., 2013; Kakurai & Akai, 1996; Maeshima et al., 2015; Ota et al., 2018; Yamanaka et al., 2004). A previous study reported that a majority of patients who were prescribed a KAFO had severe hemiparesis, such as BRS I or II (Ota et al., 2018). When clinicians and therapists consider the requirement of a KAFO for stroke patients with severe hemiparesis who are unable to walk, knee instability is typically the most concerning issue. In addition, the affected knee extensor muscle strength indicates global LL strength on the affected side (Aguiar et al., 2019). Thus, it is reasonable to consider that NormHHD-AK is a valid predictor of the need for a KAFO in the subacute phase of stroke.
In the present study, analysis of the ROC curve revealed a NormHHD-AK cut-off value of 41.61 to predict the continuous need for a KAFO in the subacute phase with high accuracy. That is, if the knee extension strength on the affected side is≤41.6% of that on the non-affected side at the time of initial evaluation, the patient is likely to require a KAFO 30 days after onset. The results of the present study suggest that knee extension strength assessed using an HHD is useful information in deciding whether to prescribe a KAFO in the acute phase of stroke. Based on the findings of recent studies (Abe et al., 2021a; Abe et al., 2021b; Sato et al., 2022), our results may be useful for early making of a KAFO in patients who need gait training using a KAFO.
In the present study, SCP was also associated with the continuous need for a KAFO. SCP is a method of evaluating PS (Babyar et al., 2009; Karnath et al., 2000). Stroke patients with PS actively push away from the unaffected side, leading to a loss of postural balance and falling towards the affected side (Karnath, 2007). Previous studies have reported that patients with PS are more likely to develop severe motor paralysis than those without (Danells et al., 2004). Regarding weight distribution while standing, patients with PS actively push away from the unaffected side, causing an overload on the leg on the affected side. This overload promotes bending of the knee on the affected LL and induces more instability. Therefore, patients with PS require KAFO support due to increased load on the affected LL, and it is reasonable that SCP was a predictor of the need for a KAFO in this study.
There are some limitations to the present study. First, our criteria for both patient selection and grouping of the KAFO/non-KAFO groups may have caused a selection bias; however, as there is no gold standard for determining the need for a KAFO, our results can be considered preliminary for the development of criteria that constitute the need for a KAFO in stroke patients. Second, our study did not include biomechanical data such as ground reaction force and three-dimensional motion analysis. Had we included biomechanical analysis, we could have obtained detailed information on hemiparetic gait. Third, the present study did not utilize any recently developed neuroimaging techniques, such as diffusion tensor tractography to evaluate the integrity of the corticospinal tract and single-photon emission computed tomography to detect cerebral blood flow abnormality. Fourth, the study population was relatively small, with limited statistical power, which preclude us from ruling out chance findings. Further large studies are needed to determine the factors for predicting the continuous need for a KAFO. Fifth, we did not investigate the duration of treatment in detail, which could have influenced the results of this study. However, the duration and content of physical therapy were standardized within the research facility, and the physical therapy itself was provided in accordance with the regulations concerning the Japanese health insurance system.
Conclusion
We hypothesized that, by quantitatively evaluating the LL muscle strength of the affected side in the acute phase of stroke, it is possible to accurately predict walking ability in the subacute phase. The results of the present study revealed that NormHHD-AK and SCP are predictors of the need for a KAFO. In particular, NormHHD-AK had the highest predictive ability, suggesting that it can be a useful predictor of the need for a KAFO in the subacute phase of stroke because of its simple and easy measurement with high reproducibility. At present, there are no definitive criteria for prescribing a KAFO. Therefore, it is desirable to establish accurate criteria that will allow clinicians to decide whether or not a KAFO should be prescribed. The present study revealed the factors related to the continuous need for a KAFO at one month after stroke onset. Our results may contribute to the early prescription of a KAFO for patients who require gait training with the help of such a device.
Footnotes
Acknowledgments
The authors are grateful to the individuals who volunteered to participate.
Conflict of interest
The authors have no conflicts of interests to report.
Funding
The authors report no funding.