
Abstract
Background:
Current interventions for major depressive disorder (MDD) are suboptimal, and only one third respond to them on initial treatment. Neuroplasticity theories are the basis for several emerging treatments. Evidence on the impact of yoga, a well-known mind-body intervention, on neuroplasticity in MDD is limited.
Objectives:
To determine the effects of 12-week yoga- and meditation-based lifestyle intervention (YMLI) on depression severity and systemic biomarkers of neuroplasticity in adult MDD patients on routine drug treatment.
Methods:
A total of 58 MDD patients were randomized into yoga or control group. The severity of depression was assessed with Beck Depression Inventory-II scale (BDI-II). Blood samples were collected before and after intervention for the measurement of the biomarkers that characterize neuroplasticity, including mind-body communicative and cellular health biomarkers.
Results:
There was a significant decrease [difference between means, (95% CI)] in BDI-II score [–5.83 (–7.27, –4.39), p < 0.001] and significant increase in BDNF (ng/ml) [5.48 (3.50, 7.46), p < 0.001] after YMLI compared to control group. YMLI significantly increased DHEAS, sirtuin 1, and telomerase activity levels, and decreased cortisol, and IL-6 levels, in addition to decreasing DNA damage and balancing oxidative stress. Multiple regression analyses were used to associate neuroplasticity biomarkers with depression severity. A ‘post-intervention change in BDNF’ x ‘group’ interaction indicated that yoga group had more BDNF in association with less BDI-II scores relative to controls. Increased sirtuin 1 and telomerase activity and decreased cortisol significantly predicted this association (all p < 0.05).
Conclusion:
These results suggest that decrease in depression severity after YMLI in MDD is associated with improved systemic biomarkers of neuroplasticity. Thus YMLI can be considered as a therapeutic intervention in MDD management.
Introduction
Major depressive disorder (MDD) is a modern world pandemic, affecting both mind and body (Penninx et al., 2013). It has become the largest contributor to the global burden of disease (Ferrari et al., 2013; Korsager Larsen & Matchkov, 2016; World Health Organization, 2016) with a worldwide prevalence of 9–36% and is associated with an increase in mortality risk by 60–80% (Cuijpers et al., 2014; Penninx et al., 2013; Walker et al., 2015). Accelerated cellular aging associated with this disorder (Sibille, 2013; Verhoeven et al., 2014) contributes to decreased neuroplasticity (Player et al., 2013) and impaired mood, cognition, and somatic health (Verhoeven et al., 2014). Current first-line treatment based on monoamine hypothesis has failed to explain the pathobiology of MDD thoroughly and provides remission only in approximately one-third of the patients (Kuhn et al., 2014) on treatment initiation. Considering the limited and suboptimal remission, frequent relapses, and complications associated with it, new theories of depression are emerging, and improving neuroplasticity has become the basis for many new treatments (Cramer et al., 2011; Gerhard et al., 2016). These emerging treatments include passive interventions like ketamine and repetitive transcranial magnetic stimulation (rTMS) (Gerhard et al., 2016). The long-term biological and clinical effects of these interventions are unknown, and the patients may suffer from severe irreversible complications (Corlett et al., 2006; Morgan et al., 2004; Wassermann & Zimmermann, 2012). Interventions that provide a long-lasting improvement in neuroplasticity and characterize the mechanisms which determine optimum neuroplasticity in regions of the brain affected by MDD warrant further research.
Yoga is a mind-body intervention (MBI) that has become increasingly popular worldwide. Yoga is a profound science for wellbeing and disease management. Biopsychosocial principles underlie the practice of yoga, and the accumulating evidence suggests that it has a positive impact on both mental and physical health (Büssing et al., 2012). A recent meta-analysis (Goldberg et al., 2018) support the notion that mindfulness-based interventions hold promise as evidence-based treatments for psychiatric disorders and showed the most consistent evidence in support of mindfulness for depression. Regular practitioners of yoga and meditation showed a reduced age-associated decline in gray matter, which is an index of optimum neuroplasticity (Froeliger et al., 2012; Villemure et al., 2015). Recent studies have shown that practice of yoga and meditation, even for short duration, can increase neuroplasticity in the brain of both healthy individuals (Hölzel et al., 2011) and patients with neuropsychiatric conditions (Eyre et al., 2016). Although several recent studies have shown clinical benefits of yoga in MDD (Cramer et al., 2017; Prathikanti et al., 2017), surprisingly, there are few studies examining how yoga- and meditation-based interventions affect systemic biomarkers of neuroplasticity in MDD. In this regard, Naveen et al. (2016) showed a significant positive correlation between the decrease in depression severity and rise in serum BDNF and reduced cortisol levels in MDD patients after yoga practice for 12 weeks. Recently, studies have also reported the benefits of yoga in improving multiple biomarkers that have an impact on neuroplasticity, in apparently healthy (Qu et al., 2013; Tolahunase et al., 2017) and stressed individuals (Harkess et al., 2016).
Neuroplasticity is the ability of the central nervous system (CNS) to adapt and reorganize its structure and function in response to internal or external stimuli and manifests at both biological and clinical levels. The high-level of plasticity, which makes hippocampus and other regions of the CNS affected by MDD vulnerable to neurodegeneration (Bartsch & Wulff, 2015), suggests that it is equally modifiable by interventions. Systemic biomarkers dynamically reflect biology in the brain, including neuroplasticity (Liew, Ma et al., 2006), and the relationship between peripheral blood and brain across various domains of analysis provide a context for evaluating systemic biomarkers in MDD. The pathobiology which can influence neuroplasticity is associated with modifications in several mechanisms, including - neurotransmission; neuroendocrine, immune, and metabolic regulations; the microbiota and the gut-brain axis; and the gene-environment interactions. Novel systemic biomarkers of neuroplasticity that are associated with these processes include: BDNF (brain derived neurotrophic factor) (Autry & Monteggia, 2012; Bocchio-Chiavetto et al., 2010), sirtuin1 (Abe et al., 2011; Jesko et al., 2017), cortisol (Vreeburg et al., 2009), IL-6 (Zhang et al., 2016), DHEAS (dehydroepiandrosterone sulfate) (Uh et al., 2017), and also the markers of oxidative stress (Liu et al., 2015), DNA damage (Czarny et al., 2015), and telomere metabolism (Henje Blom et al., 2015). As several imaging studies suggest that the practice of yoga and meditation altered the regional brain volumes and functional brain circuits (Froeliger et al., 2012; Hölzel et al., 2011), they presumably could affect neuroplasticity. However, current evidence is limited regarding how yoga practice affects the systemic biomarkers of neuroplasticity, especially in MDD. Evidence suggests that these novel biomarkers improve with MBIs, comprising either or both physical and mental components, in a spectrum of clinical and experimental conditions, and have resulted in increased neuroplasticity (Bayod et al., 2012; Boccatonda et al., 2016; Campbell et al., 2010; Duraimani et al., 2015; Hofer et al., 2008; Ornish et al.; Szuhany et al., 2015; Villanova et al., 2013).
With this context in mind, the primary aim of the present study was to determine the effects of a 12-week yoga- and meditation-based lifestyle intervention (YMLI) on depression severity and systemic biomarkers of neuroplasticity. Our study included a combination of biomarkers that characterize neuroplasticity in MDD patients that include: the cardinal biomarker of neuroplasticity – BDNF; mind-body communication biomarkers – cortisol, IL-6, DHEAS, and sirtuin 1; and biomarkers of cellular health – oxidative stress (reactive oxygen species, ROS and total antioxidant capacity, TAC), DNA damage (8OH2dG), and telomere metabolism (telomerase activity and telomere length).
Materials and methods
Trial Design
The study was a single-arm parallel-randomized controlled trial analyzing the effects of a 12-week YMLI on depression severity and systemic biomarkers of neuroplasticity in MDD patients on routine drug therapy. The intervention period was from April 2015 to September 2016. The study was initiated after ethical clearance (ESC/T-370/22-07-2015) from the institutional ethics committee and the registration of the trial (Clinical Trial Registry of India (CTRI) REF/2014/09/007532). CTRI is one among the primary registries of the International Clinical Trials Registry Platform (ICTRP) of the World Health Organization (World Health Organization, 2018). All participants provided signed informed consent. The data were reported according to CONSORT statement (Moher et al., 2010).
Participants, eligibility criteria, and settings
Participants were recruited from the outpatient unit of Psychiatry department of AIIMS, New Delhi. The study inclusion criteria included age 19–50 years old MDD patients diagnosed with DSM-5 criteria and on routine drug treatment for at least six months. The exclusion criteria included subjects having very severe depression (BDI-II scale score ≥45), and subjects having other co-morbid neuropsychiatric and chronic medical conditions, including bipolar disorder, hypertension, diabetes mellitus that secondarily have co-morbid depression.
Interventions
A total of 58 participants were randomized into yoga or control group, after recruiting and screening eligible subjects. Baseline characteristics were recorded before the intervention. Participants underwent a 12-week pre-tested YMLI program comprising theory and practice sessions (Tolahunase et al., 2017). YMLI program included sessions five days per week and was suitably modified for MDD patients in the current study. The sessions were taught by registered, specialized yoga instructors at the integrated health clinic (IHC), AIIMS, New Delhi. The details of the activities during YMLI program are given in Table 1. Each session in YMLI included a set of asanas (physical postures), pranayama (breathing exercises), and dhyana (meditation) for approximately 120 minutes. YMLI included interactive lectures on lifestyle, lifestyle diseases, MDD, and the importance of their prevention. The Hawthorne effect was insignificant because of YMLI’s emphasis on environmental enrichment and self-awareness.
Details of activities of the yoga- and meditation-based lifestyle intervention (YMLI) program
Details of activities of the yoga- and meditation-based lifestyle intervention (YMLI) program
The primary outcome was to assess the change in severity of MDD [Beck Depression Inventory-II scale (BDI-II) scores)] from baseline to week 12. The composite primary outcome was to assess the change in the levels of blood biomarkers related to neuroplasticity that included: the cardinal biomarker of neuroplasticity – BDNF; mind-body communicative biomarkers – sirtuin 1, cortisol, IL-6, and DHEAS; and biomarkers of cellular health – oxidative stress markers (reactive oxygen species, ROS and total antioxidant capacity, TAC), DNA damage marker (8OH2dG), and telomere metabolism (telomerase activity and telomere length).
Sample size calculation
The sample size calculation was based on the findings from previous publications of other research groups who have shown beneficial effects of yoga with similar sample size (Sarubin et al., 2014). Calculations assumed two-tailed α= 0.05 and 1-β= 80% to detect a 20% difference.
Randomization and blinding
Computer-generated random numbers were used for randomization with unrestricted equal participant allocation, with the assistance of the web tool research randomizer (https://www.randomizer.org/), and with the participants not blinded to the study. A research assistant not otherwise involved in the study created the randomization allocation schedule.
Measurement of clinical parameters
The severity of depression was assessed with BDI-II scale, which is considered a clinically useful criterion and is widely accepted in MDD trials as the primary outcome (Frank et al., 1991; Freedland et al., 2015; Reeves et al., 2012).
Measurement of blood biomarkers related to neuroplasticity
During this 12-week study, the participants were evaluated for various biomarkers at baseline and week 12. Fasting venous blood samples (5 mL) were collected and divided into two parts. One part was allowed to clot, and the serum was separated within 30 min, and the other part was transferred to heparinized and EDTA vials and was centrifuged at 2000 g for 15 minutes at 4°C. Both serum and plasma were stored at –80°C until analyzed.
ROS detection was done by chemiluminescence assay (Berthold detection luminometer, USA). TAC was estimated by a colorimetric assay (Cayman Chemical, Ann Arbor, USA). Telomerase activity was determined by using a telomerase assay kit (Roche, Switzerland) as per the manufacturer’s protocol. Peripheral blood leucocyte telomere length was measured by the qPCR method. 8-OH2dG was estimated in white blood cell DNA (Cayman’s EIA kit). ELISA kits were used for the levels of BDNF (Raybiotech, Inc), sirtuin 1 (Qayee Bio-Technology), DHEAS (Qayee Bio-Technology), cortisol (DRG Diagnostic, Germany), and IL-6 (Gen-Probe, Diaclone Diagnostic, France). Quality-control assays for biomarkers and validation were performed.
Statistical analysis
Tests were conducted using SPSS 23.0 (SPSS Inc., Chicago, IL) at an α of 0.05 using primary intent-to-treat analysis (ITT) approach, with the baseline observation carried forward (BOCF). We used chi-square test and Fisher’s exact test to compare categorical characteristics at baseline; we used student’s t-test to compare normally distributed continuous variables and the Wilcoxon rank-sum test to compare nonparametric continuous data (Table 2). Within-group changes over time (pre- to post-intervention) were evaluated using paired t-tests for continuous variables, or Wilcoxon signed rank test for continuous variables without normal distribution. Between-group differences over time were assessed using independent samples t-test. Mixed factorial design ANOVA was used to assess gender differences. Multiple regression was used to determine the change in which variables significantly explained the association and interaction of neuroplasticity and change in depression severity.
Baseline characteristics
Baseline characteristics
Data were described as frequency (%) for sex and mean (SD) for others. SES, socioeconomic status.
Participants’ flow and baseline characteristics
Participants (n = 58) were randomly assigned to yoga or control groups. Figure 1 shows the CONSORT flowchart of intervention. No harmful effects were observed by YMLI. There were no significant differences in baseline characteristics between the two groups (Table 2).
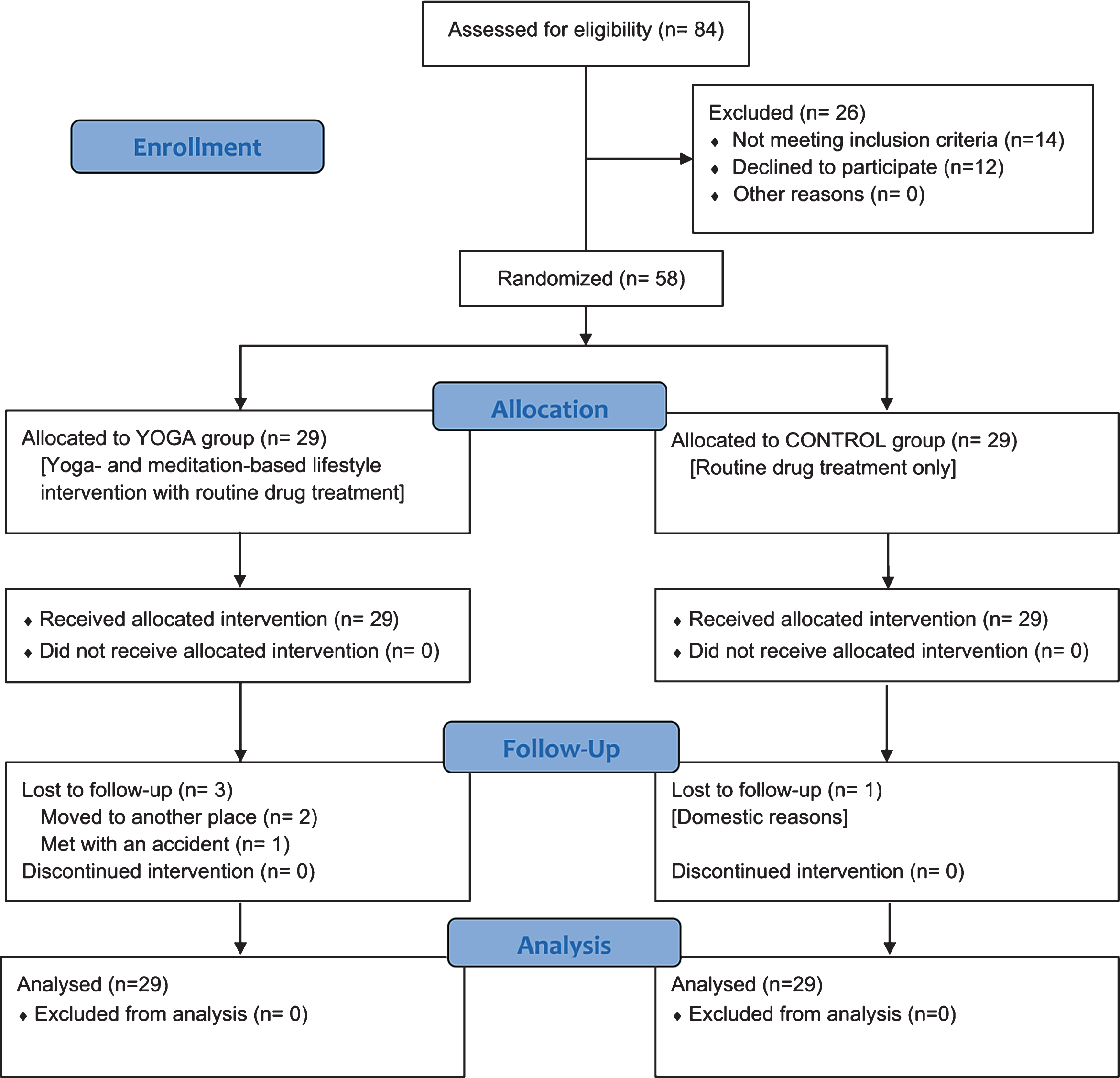
CONSORT flow chart of the study.
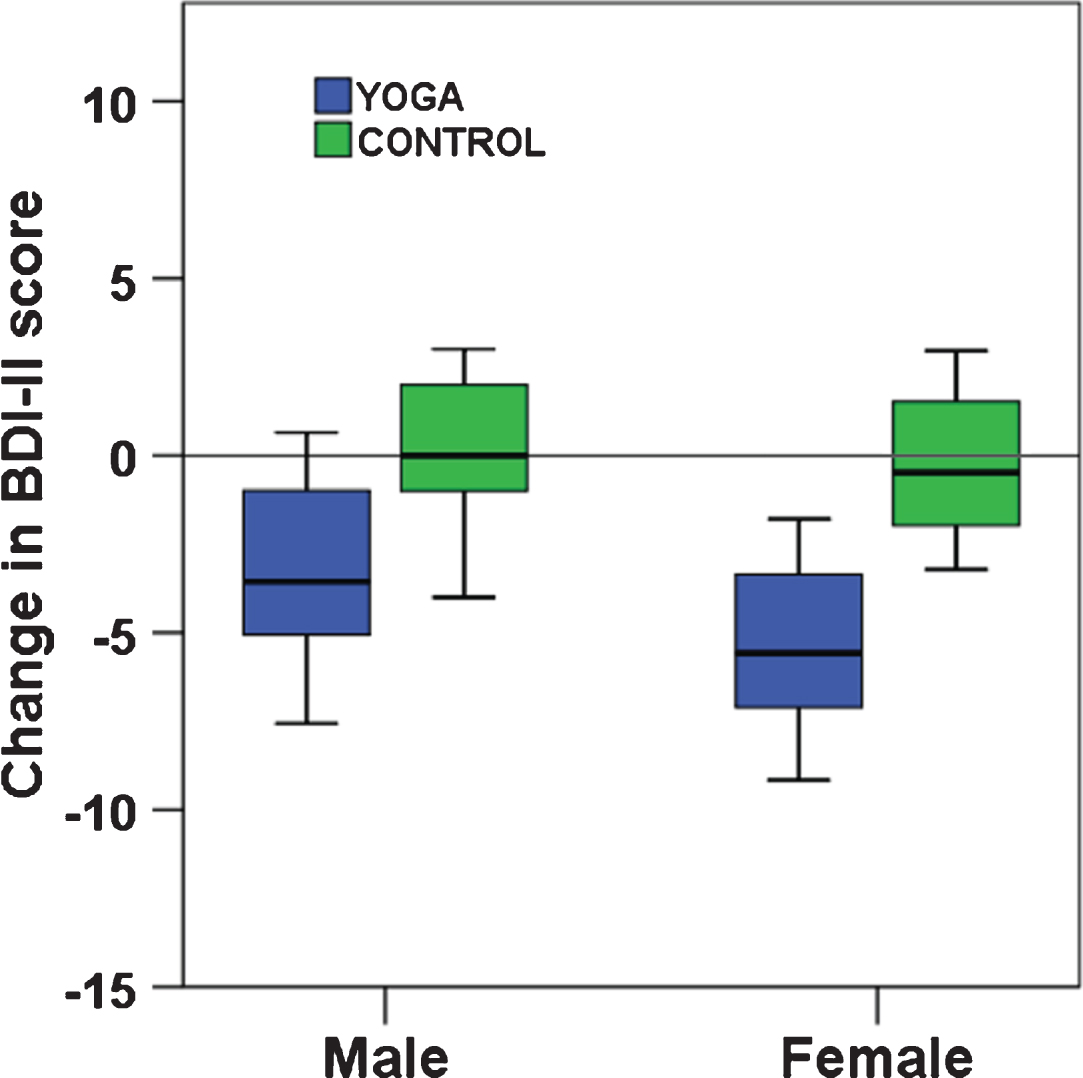
Gender interactions for change in depression severity after the intervention. A. Mean change of BDI-II score with 95% CI for men in the yoga and the control groups; p < 0.032 for between-group difference of change in the study, adjusted for baseline value. B. Mean change of BDI-II score with 95% CI for women in the yoga and the control groups; p < 0.003 for between-group difference of change on the study, adjusted for baseline value.
As shown in Table 3, there was a significant decrease [difference between means, (95% CI)] in BDI-II score [–5.83 (–7.27, –4.39), p < 0. 001] and significant increase in BDNF (ng/ml) [5.48 (3.50, 7.46), p < 0. 001] after YMLI compared to control group. Among the mind-body communicative biomarkers, there was a significant increase in circulating DHEAS and sirtuin 1 and a significant decrease in circulating cortisol and IL-6 after YMLI compared to yoga group at baseline level and control group. A total of 12 weeks YMLI showed improvement in cellular health biomarkers that included - significant decrease in 8OH2dG (marker of DNA damage); significant increase in TAC and decrease in ROS (markers of oxidative stress); and significant increase in telomerase activity (marker of telomere attrition) compared to control group (all p < 0. 05) (Table 3). However, change in telomere length was not significant in both groups. Also, the control group showed significantly increased ROS and IL-6 levels compared to baseline (P < 0.001).
Means (SD) and results of within-group and between-group analysis of systemic biomarkers of neuroplasticity (n = 58; YMLI, 29; Control, 29)
Means (SD) and results of within-group and between-group analysis of systemic biomarkers of neuroplasticity (n = 58; YMLI, 29; Control, 29)
CI = Confidence interval. 1paired samples t-test. † Wilcoxson signed rank test. 2independent samples t-test.
Men were significantly more depressed at baseline than women (BDI-II scores 30.4±7.82 and 26.10±8.26 mean±SD respectively). Three-way interactions including group and gender indicated favorable responses to YMLI for men for DHEAS (F(1,54) = 5.02; p < 0.03). Separate analyses for males and females were, therefore, performed to overcome baseline violations in depression severity and to explore further specific gender effects. Clinical improvement was more significant for the women in yoga group (mean between-group difference of change: Female = –6.12, F(1,29) = 10.81, p = 0.003; Male –3.86, F(1,25) = 5.14, p = 0.032 (Fig. 3).
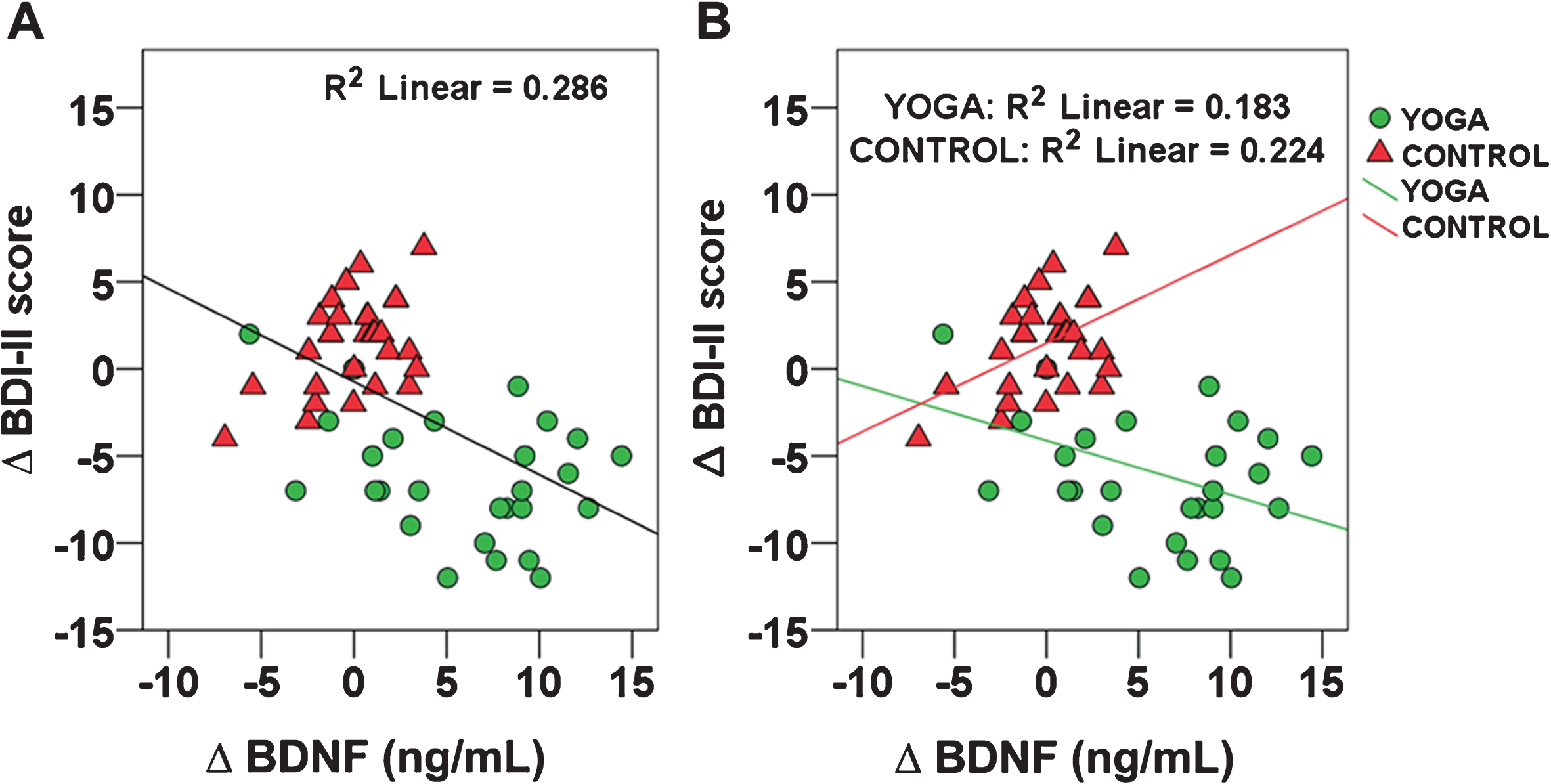
The relationship between Δ BDNF and Δ BDI-II (depression severity) score across participants (A) and a Δ BDNF×group interaction (B) testing such an association for each intervention group. Δ indicates pre-post intervention change.
Since neuroplasticity influences depression severity, we planned to analyze the relationship between BDNF, the cardinal marker of neuroplasticity, and depression severity. Figure 3A depicts the correlation between BDNF and the BDI-II scores across groups (R2 = 0.286; P < 0.001). Follow-up multiple linear regression was conducted to analyze the association of the mind-body communicative and cellular health biomarkers that are related to neuroplasticity.
The dependent variable was the BDNF predicted change in BDI-II scores. Different regression models using stepwise, forward, or enter methods produced similar results. The regression model predicted 18.7% of the variance across both groups [F(9,48) = 3.960; P < 0.01]. Higher levels of cortisol (R2 = 0.194; P < 0.05) and ROS (R2 = 0.178; P < 0.05) were associated with increased BDI-II scores (data not shown). Since YMLI may significantly affect neuroplasticity, we tested for the association of change in BDI-II scores in yoga group in comparison to control group. Yoga group showed greater reduction in BDI-II scores as BDNF increased (R2 = 0.183; P < 0.05) (Fig. 3B). However, for controls higher BDNF unexpectedly corresponded to increased BDI-II scores (R2 = 0.224; P < 0.01) (Fig. 3B). To further analyze the mediators that might explain the interaction of group effect, multiple linear regression was performed in parallel on each intervention group. The BDNF×group interaction predicted change in BDI-II scores was the dependent variable. As shown in Table 4 and Fig. 4 A–C yoga group had strong associations between cortisol, sirtuin 1, or telomerase activity and change in BDI-II score related to the interaction. However, the control group showed nonsignificant relationships for these variables as shown in Fig. 4 D–F and Table 4.
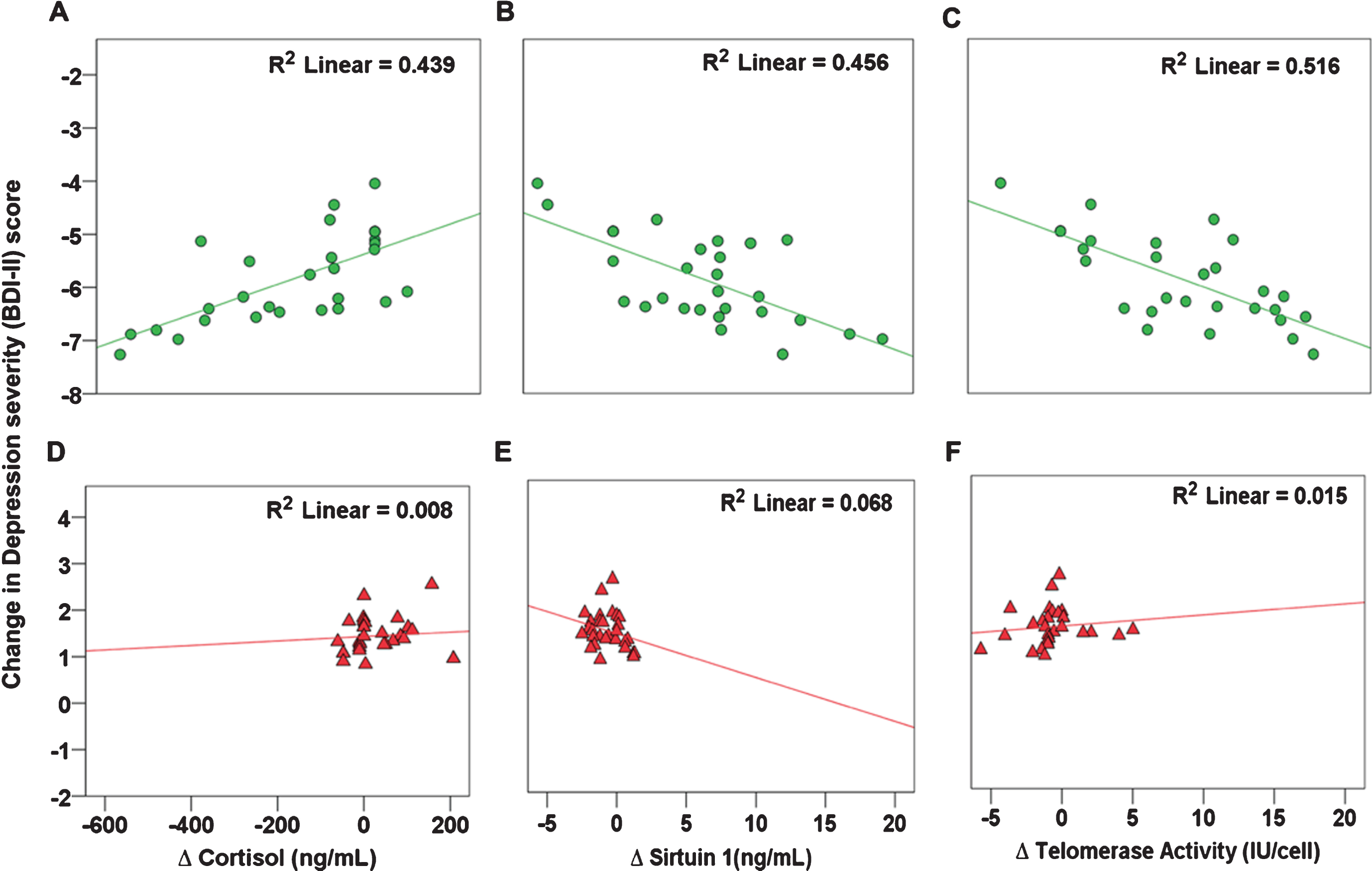
Shown are the partial regression plots that depict error variance of the effect on change in BDI-II scores by cortisol, sirtuin 1, and telomerase activity in yoga and control groups. Neuroplasticity mediator variables are shown regressing on the change in BDI-II scores predicted by change in BDNF × group interaction. Yoga and control groups are represented by circles and triangles respectively.
Significant predictors of change in BDNF x group interaction with change in BDI-II scores
Multiple regression was used to assess which mind-body communicative and cellular health variables mediated the Δ BDNF×group interaction effect. These variables were regressed onto the predicted Δ BDI-II scores due to Δ BDNF for yoga or control groups. For the final yoga model, the adjusted R2 of the mediation model was 0.786 [F(9,19) = 12.440; P < 0.001]. For the final control mediational model, the adjusted R2 was –0.024 [F(9,19) = 0.926; NS]. DHEAS, dehydroepiandrosterone sulfate, ROS, reactive oxygen species, TAC, total antioxidant capacity, 8OH2dG, 8-hydroxy 2’-deoxy guanosine. *P≤0.05. Δ indicates a change between post-intervention and pre-intervention values.
We hypothesized that YMLI reduces depression severity by improving neuroplasticity, as indicated by its systemic biomarkers. In the present study, the increase in BDNF, the cardinal biomarker of neuroplasticity, after 12 weeks YMLI, was significantly associated with the reduction of depression severity. While yoga group showed a significant post-intervention increase of BDNF levels in comparison to control group, there was an unexpected trend of increasing BDI-II scores with increasing BDNF levels in the control group. Our study also highlights that yoga group significantly improved systemic biomarkers related to neuroplasticity, including: mind-body communicative biomarkers - sirtuin 1, cortisol, IL-6, and DHEAS; and cellular health biomarkers - markers of oxidative eustress (ROS and TAC), DNA damage (8OH2dG), and telomere metabolism (telomerase activity). Improvement in systemic biomarkers of neuroplasticity in association with the positive clinical outcome of reduction in clinical severity, suggests that YMLI may provide long-term clinical remission in MDD, by positively modifying the pathobiology, at the level of the brain, mind-body communications, and cellular health.
YMLI improves neuroplasticity
Yoga, a premier MBI, has been increasingly accepted as a cost-effective strategy for promoting physical and mental health. This is evident from the reduced age-associated decline in the gray matter of regular meditators (Froeliger et al., 2012; Hölzel et al., 2011). Recent studies and meta-analysis (Boccia et al., 2015; Fox et al., 2014) of neuroimaging in meditation practitioners, found consistent alterations and activations of brain areas involved in the processing of higher mental functions. BDNF plays an important role in neuroplasticity and neurogenesis and is a cardinal biomarker (Thoenen, 1995), which positively correlate with the enhanced neuroplasticity seen at morphometric, neural network, and molecular levels. There is even a growing interest to translate BDNF biology into therapies for depression (Lu et al., 2013). Although passive interventions modify neuroplasticity (Duman & Voleti, 2012) and related processes in the brain, they fail to provide long-term remissions and are associated with complications (Penn & Tracy, 2012). In a recent study, exercise increased BDNF levels in MDD patients (Kerling et al., 2017). In another study, Taekwondo, a form sport, and exercise, improved neuroplasticity-related growth factors, including BDNF, in healthy children (Cho et al., 2017). Yoga has also been shown to improve levels of BDNF in MDD (Naveen et al., 2016). Our study further confirmed that in MDD subjects 12 weeks of YMLI could significantly increase systemic BDNF levels, in association with improvement in biomarkers of mind-body communication and cellular health. A recent review has analyzed how peripheral somatic stimulation by acupuncture may increase neurotrophic factors like BDNF, and improve neuroplasticity (Shin et al., 2017). Asanas (postures), and pranayama (breathing exercise) in YMLI may provide similar peripheral stimulation to CNS. In this regard, increased BDNF levels and improved clinical outcomes by YMLI, suggest that it may be an intervention to improve neuroplasticity, reverse pathobiology of MDD, and provide long-term remission.
Evidence regarding how yoga practice affects blood BDNF level, and increase neuroplasticity remains inconsistent. On a neurobiological level, BDNF (Thoenen, 1995) and its signaling partners (Park & Poo, 2012) have emerged as key regulators of neuroplasticity. They contribute to complex functions of the brain, like cognition and emotion, by mediating synaptic plasticity and structural and functional long-term potentiation (LTP) (Sasi et al., 2017). BDNF activated signaling cascades involve, mainly its receptor, the receptor tyrosine kinase (TrkB), and mechanistic target of rapamycin (mTOR). Evidence suggests that vagal nerve stimulation rapidly activates TrkB in rat brain. Yoga components in YMLI might improve parasympathetic activity and cardiovagal tone (Streeter et al., 2012). mTOR is a regulator for the initiation of protein translation and synthesis. Elevated mTOR signaling promotes the synthesis of synaptic proteins that are necessary for synapse formation and maturation (Abelaira et al., 2014; N. Li et al., 2010). The mTOR signaling pathway may also be activated by N-methyl-d-aspartate (NMDA) receptor, and dopamine receptor-mediated signaling (Duman & Voleti, 2012). The mTOR-dependent translational cascade in synaptic plasticity may be the final pathway that represents a rapid-acting and long-lasting onset of therapeutic benefits, including YMLI. Bekker et al. (2014) have suggested that regulation of gene expressions including BDNF is important for the actions of active interventions like mindfulness. Improved mind-communicative and cellular health biomarkers may have a significant role in optimizing gene expressions, including BDNF.
YMLI improve mind-body communications (MBCs) to regulate neuroplasticity
The most significant dysregulation of MBCs for brain pathology in MDD includes exaggerated stress response, immune hyperactivity (Pribiag & Stellwagen, 2014), and abnormalities in adiposity, vascularity, and sexuality (Verhoeven et al., 2014). These dysregulations in MBCs have a detrimental impact on the CNS, and damage neuropil structure and function leading to deficits of neuroplasticity. The HPA axis is the most common biological system for MBCs in MDD (Holsboer & Ising, 2010; Schatzberg, 2015) and alterations in it are associated with impaired higher mental functions (Hinkelmann et al., 2009). Meta-analyses concluded in the past have confirmed that patients with MDD have increased cortisol levels (Stetler & Miller, 2011). Higher cortisol levels are associated with reductions in hippocampus volume (Colla et al., 2007), and decreasing cortisol levels reverses this change (Vythilingam et al., 2004). Increased cortisol is known to suppress BDNF secretion in the brain by repressing glucocorticoid receptors (Chen et al., 2017; McEwen et al., 2016) and contribute to neurodegeneration. Findings across groups in our study support the association of increased cortisol with reductions in BDNF and increase in depression severity. A study by Taren et al. (Taren et al., 2015) indicates that mindfulness meditation training promotes functional neuroplastic changes, and implicate decoupling of the amygdala and subgenual anterior cingulate cortex (sgACC) as a potential neurobiological mechanism underlying mindfulness training intervention effects. Naveen et al. (2016) have shown that cortisol reduction in MDD by yoga correlated with an increase of BDNF levels in the blood. Our study confirms that YMLI decreases cortisol level and improve MBCs that regulate neuroplasticity in MDD. Also, findings from our study show that YMLI mediated decrease in cortisol has a significant impact on increasing BDNF and reducing depression severity. Previous studies have indicated that increased cortisol depress activity-dependent expression of BDNF mRNA in hippocampal neurons (Cosi et al., 1993; Smith et al., 1995). Therefore, decrease in cortisol after YMLI may increase BDNF and enhance BDNF mediated neuroplasticity. Cellular recovery may involve multiple regulatory factors like the eukaryotic translation initiation factor 2 alpha (eIF2α) that converge on the regulation of adaptive pathways including integrated stress response (ISR) (Pakos-Zebrucka et al., 2016), which drive the signaling toward cell survival and longevity.
The immune system is an essential component of the physiological stress-sensing pathways and closely interacts with the body’s primary integrative MBC systems, including HPA axis, in mutually regulatory feed-forward and feedback loops. Previous research has documented the neuroimmunological mechanisms of peripheral immune dysfunction in MDD, and have shown that these routes converge in the CNS to alter molecular programmes, neurogenesis, and plasticity (Hodes et al., 2015). Frodl et al. have reported that high IL-6 levels are associated with increased cortisol and reduced hippocampal volumes in MDD (Frodl et al., 2012). A systematic review of gene expression changes by Buric et al. (2017) indicate that MBI practices are linked to downregulation of nuclear factor kappa B (NF κB) pathway, an effect opposite to that of chronic stress on gene expression. Meditation results in a decrease in inflammation as evident from the reduction in levels of inflammatory marker IL-6 and increases neuroplasticity, as shown in a study using imaging (Creswell et al.). Our findings of a decrease in IL-6 after YMLI suggests that MBI practices may lead to a reduced risk of inflammation-related neuropathology (Buric et al., 2017). Our present study is the first to show that 12 weeks of YMLI could reduce the IL-6 levels in MDD, indicating that YMLI practice is an efficient way for reducing neuroinflammation and pathological changes in the brain associated with MDD.
DHEA and its sulfated derivative, DHEAS, are cholesterol-derived steroids synthesized in the adrenal glands and de novo in neurons and glia. DHEAS acts as a GABA(A) receptor noncompetitive antagonist and a positive allosteric modulator at the NMDA receptor (Genud et al., 2009; Kimonides et al., 1998). It has neuroprotective, antioxidant, and anti-inflammatory properties (Maninger et al., 2009), and appears to be dysregulated in MDD (Wong et al., 2011). Previous studies have shown that DHEA administration in MDD patients reported a significant reduction in depressive symptomatology (Schmidt et al., 2005). In a review, Sripada et al., (Sripada et al., 2013) have illustrated that DHEA enhances emotion regulation neurocircuits and modulates memory for emotional stimuli. In the present study patients receiving YMLI showed increased DHEAS levels. Postmortem studies using the brain of MDD patients indicate a close relationship between DHEA and BDNF-TrkB pathways (Qi et al.). DHEA has also been shown to increase neuron survival by modulation of the mTOR signaling (T. Chen et al., 2017). Therefore, increased DHEAS after YMLI may increase BDNF mediated neuroplasticity by activating mTOR pathways. Increased DHEAS after YMLI may also decrease depression severity by decreasing heightened brain excitability of MDD (Pennisi et al., 2016), since DHEAS can inhibit glutamate-induced excitotoxicity (T. Chen et al., 2017; Dong et al., 2009) and modulate the inhibitory neurotransmitter GABA (Genud et al., 2009). Goldman and Glei have reported that lower levels of DHEAS increase depressive symptoms in men, which may contribute to increased baseline severity as seen in our study (Goldman & Glei, 2007). Although not significant, women tended to show higher reductions in depression severity. This may be due to transitory and fluctuating sex hormone levels in the brain that induce the continuous functional adaptation of the CNS throughout the lifespan, particularly in females (Juraska et al., 2013; Nugent et al., 2012). It has been observed that neurogenesis in the dentate gyrus is higher in female than in males, probably because of the variations in gonadal hormones (Duarte-Guterman et al., 2015). Evidence suggests that estradiol (E2) and/or progesterone (P4) promote neurogenesis and neurological functions under different brain insults and diseases (Z. Li et al., 2012; Zheng et al., 2013), and also protect against neurodegenerative diseases.
Among the factors which promote longevity, nutrition and energy sensing pathways are important, and sirtuin 1 play a prominent role, in association with other factors. Sirtuin 1 (SIRT1), a member of mammalian class III histone deacetylases, and a nutrient and energy sensor (Toorie et al., 2016), has been a target for interventions in longevity and aging-related diseases. It is known to block neuropathology, prevent neuronal cell death (Cunha-Santos et al., 2016; Guida et al., 2015; Nimmagadda et al., 2013), and promote synaptic plasticity (Gao et al., 2010). Recent evidence suggests that caloric restriction and resveratrol could increase circulating sirtuin 1 levels (Guarente, 2013; Xu et al., 2014). Our study is the first to document an increase in sirtuin 1 levels independent of caloric restriction after YMLI in MDD. Our findings also suggest that sirtuin 1 contributes significantly to the association of BDNF with BDI-II scores. A study in rats has reported that rehabilitation training and resveratrol improve the recovery of neurological and motor function after cerebral ischemic injury through the sirt1 signaling Pathway (Shi et al., 2016). Potential underlying molecular mechanisms for decrease in MDD severity by increased sirtuin 1 include: (1) increasing cell survival and neurogenesis through mTOR signaling (Guo et al., 2011), (2) promoting synaptic plasticity by increasing BDNF transcription, mediated by inhibition of miR-134 expression that inhibit binding of cAMP response element-binding protein (CREB) to several BDNF promoters, (3) regulating circadian rhythm mediated by inhibiting the central circadian timer protein CLOCK, a histone acetyltransferase (Nakahata et al., 2009).
The improved mind-body communicative biomarkers constitute the reversal of senescent secretory phenotype of cells, both in the CNS and peripheral organ systems. Since, secretory phenotype from somatic cells provides regulatory feedback to the brain (Tchkonia et al., 2013), improved biomarkers after YMLI may mediate to optimize the vicious cycle of regulation between mind and body and contribute to decrease in MDD neuropathology. Crosstalk between regulatory feedback pathways and neurocircuits in the brain not only play a role in pathogenesis but also drive the progression of depression, which may contribute to non-responsiveness to current antidepressant therapies. Regulated mind-body communications may lead to the minimization of the adverse effects of these cross-talks to provide improved clinical outcomes. Our present study suggests that, in MDD, 12 weeks of YMLI could improve MBCs, decrease pathobiology of MDD and contribute to enhanced neuroplasticity and decrease in depression severity.
YMLI improves cellular health to promote neuroplasticity
Cellular health, of both CNS and peripheral organ systems, and its long-term maintenance across the lifespan, is fundamental to achieve optimum neuroplasticity. This can ensure continued remission in MDD, prevent complications, and improve somatic health. Achieving and maintaining optimum cellular health depend on oxidative eustress, genomic stability, chromosomal integrity and telomere length maintenance. Biomarkers of cellular health are rapidly being accepted as surrogate markers of MDD and other chronic lifestyle diseases. Deviation from oxidative eustress is associated with macromolecular damage, telomere attrition (Szebeni et al., 2014), epigenetic modifications, and altered gene expressions. It is strongly associated with MDD pathobiology (Black et al., 2015), including altered neuroprotection, neurogenesis, and neuroplasticity in the brain (Vaváková et al., 2015). HPA hyperactivity predisposes to increased cellular oxidative stress (Spiers et al., 2015). Within the CNS, in comparison to glial cells, neurons are more vulnerable to oxidative stress due to the relatively poor expression of endogenous antioxidants. Szebeni et al. (2017) have even documented the elevated DNA oxidation and DNA repair enzyme expression in brain white matter in MDD. Our study suggests that increase in oxidative stress may significantly impact BDNF levels and depression severity in MDD. Therefore, achieving optimum oxidative eustress, even under extremes of stress associated with lifestyle and environmental challenges, is a highly sensitive task. Previous studies from our laboratory have documented that YMLI improves mitochondrial integrity as evident from increased COX activity. This aids in reducing supraphysiological free radical levels by the electron transport chain during oxidative phosphorylation. A range of strategies is adopted for reducing or preventing the oxidative stress (Poljsak, 2011). A meta-analysis by Liu et al. (2015) reported that the levels of antioxidant are increased, and the levels of oxidative damage products are decreased after antidepressant medication. While passive interventions like drugs and anti-oxidants can modify oxidative stress, clinical benefits are suboptimal. Active interventions like regular physical exercise are also beneficial in reducing oxidative stress in chronic lifestyle diseases (Camiletti-Moiron et al., 2013; García-Mesa et al., 2016; Huang et al., 2015; Teixeira de Lemos et al., 2012; Vinetti et al., 2015). Recent evidence has confirmed that yoga and meditation could re-establish oxidative eustress in apparently healthy people by increasing total antioxidant capacity, reducing inflammation and improvement in mitochondrial DNA integrity (Tolahunase et al., 2017). Findings from our study show that MDD therapy with YMLI contributes significantly to achieve oxidative eustress and decrease DNA damage. The pathophysiological relationships between oxidative stress and depression, and the potential benefits of both passive and active interventions to achieve optimum oxidative eustress deserve further research.
Several studies and meta-analyses have reported that a reduction in telomere length systemically, is associated with stressed individuals and MDD (Lin et al., 2016; Lopizzo et al., 2017; Schutte & Malouff, 2015; Wolkowitz et al., 2011). Recent studies have also documented dysregulation in telomere metabolism within the brain of a rat model of depression (Wei et al., 2015) and postmortem brain of MDD patients (Szebeni et al., 2014). Research evidence suggests that regular practitioners of yoga have increased telomere length compared to controls (Krishna et al., 2015), and yoga practice by apparently healthy individuals can increase telomere metabolism and promote longevity by slowing the rate of aging (Tolahunase et al., 2017).The main factor that causes rapid attrition of telomeres is oxidative stress, and YMLI reduces oxidative stress and inflammation and thereby aids in telomere length maintenance and promotes genome stability and maintenance of chromosomal integrity. Recent studies have also identified the possible molecular mechanisms of increase in telomere protection, after exercise (Ludlow et al., 2017). Telomerase activity is known to mediate the cell survival, promoting actions of BDNF (Fu et al., 2002). Findings from our study not only show a significant increase in telomerase activity in the yoga group but also to predict BDNF mediated reduction in depression severity. While yoga group showed an increase in telomere length compared to control group, findings were not significant, but a reduction in oxidative stress levels prevents further attrition of telomere length. Improvement in MBC and cellular health suggest that, unlike passive drug treatments and mind- or body-only interventions, YMLI improve cellular health and longevity in both brain and peripheral organ systems. This might be one of the mechanisms through which yoga- and meditation-based interventions exert their effects on neuroplasticity. However, further studies are required to confirm these findings. Molecular mechanisms underlying YMLI mediated reduction in depression severity might involve epigenetic regulation. Several studies have demonstrated the epigenetic modifications in MDD pathobiology, chiefly due to OS (Klengel & Binder, 2013, 2015). For example, DNA demethylation of FKBP5 leads to its increased expression in response to stress, which in turn leads to glucocorticoid receptor resistance and increased levels of cortisol. Na et al. (2016) have shown that higher levels of BDNF promoter methylation have a close association with the reduced cortical thickness among patients with MDD. Improved biomarkers of neuroplasticity after YMLI, may reverse these epigenetic modifications, and contribute to decrease in pathology and increase in clinical outcomes in MDD.
YMLI as a comprehensive MBI in MDD
Research has shown that both the passive and active treatments can modify neuroplasticity, although, the nature of biological and clinical impact vary (Dale et al., 2015). Current, first-line pharmacotherapy, is passive, and the therapeutic effect is based on increasing the levels of specific monoamines in the synaptic clefts. The regions where this increase will occur does depend on the type of monoamine targeted, and the neural circuitry of that monoamine. Serotonin is the target of the most commonly used anti-depressants, and its circuitry may not be regulating all the large-scale neural networks. While antidepressant drug treatments have been linked to a bottom-up modulation of neural networks related to cognition and emotion by increasing monoamine levels, mind-only active interventions like, cognitive behavioral therapy (CBT), have been implicated in a top-down control of these neural networks. Also, evidence shows that physical exercise can also provide remissions or decrease the severity in MDD, although the extent of its effectiveness is unknown. Yoga, a MBI having both psychological and physical components, will have benefits beyond additive effects from psychotherapy and physical exercise. The reason being, in yoga, as practiced in YMLI, is based on the yoga sutras (principles) of Patanjali having eight limbs (Yama, Niyama, Āsana, Prāṇāyāma, Pratyāhāra, Dhāraṇā, Dhyāna, and Samādhi). Āsana (physical postures), Prāṇāyāma (breathing exercises), and Dhyāna (meditation) are relatively more emphasized in modern times; yoga is most effective when practiced with all the classical components included, and as a way of life. Patients receive meditation (mind intervention, the seventh limb), only after both the body and the mind are conditioned, in a stepwise manner, so that brain is ready for the molding effects of this intervention. Āsanas (third limb) and Prāṇāyāma (fourth limb) provide benefits for somatic molding, independently too, like in exercise interventions. Moreover, YMLI extends further to Samādhi (the eighth limb), the final state of self-awareness (also termed Kaivalya), where the practitioner realize total freedom and independence from any stimulation whatsoever, both external and internal. Achieving such a state involve mental processes like deliberation, reflection, and bliss that involve complex and dynamic higher functional neural networks. Unlike in mind-interventions (MIs), where cognitive areas of the brain are mainly targeted, in MBIs (yoga), regions and networks of the brain regulating somatic and vegetative functions (hypothalamus), biological rhythms (pineal gland), emotion (hippocampus, amygdala), cognition (PFC), and social behavior (higher functional ‘comport’ neural networks), receive improved regulatory feedbacks from the peripheral organ systems, either directly, or through other regions of the CNS regulating them, like thalamus, and cerebellum. Studies from our laboratory have documented an increase in serotonin and melatonin levels post yoga intervention (outside the purview of this paper).
Expression of clinical symptoms in adults with MDD is associated with pathology that may result from cumulative changes during decades of brain development and structural and functional modifications in the brain due to environmental and lifestyle factors. It is widely believed that developmental alterations of neural networks may be difficult to restore by pharmacological intervention. Active MBIs like YMLI, may, however, refine the neural circuits formed during development, and enable functional modulation of synapses to restore neural network function. YMLI increases biomarkers of neuroplasticity, at the level of the brain, mind-body communications, and cellular health, improves the mitochondrial and nuclear integrity and improves COX activity. Therefore, YMLI may not only help to decrease severity in MDD but also offer hope for complete remission from MDD that result from heterogeneous biological mechanisms. Possible epistasis between the genes encoding functions of the brain, mind-body communications, and cellular health, may be responsible for modifying pathobiology and progression of MDD by YMLI that may not be possible due to the effect on one aspect of MDD pathology alone (like a gene, region or process), as occurs with pharmacological and other passive interventions. Therefore, benefits from YMLI is more powerful, since the effects of interactions may be beneficial for all endophenotypes of MDD, unlike in pharmacotherapy or psychotherapy, where specific endophenotypes show responses or remissions. These phenomena that empower neuroplasticity to CNS through YMLI need to be further explored using modern technologies and methodologies. As documented in our previous studies, improvement in mitochondrial and nuclear DNA integrity and improvement in COX activity after YMLI, aids in meeting the energy demands of a tissue with a high metabolic rate.
To the best of our knowledge, the present study is the first RCT of yoga studying its impact on cellular health and mind-body communicative factors on neuroplasticity and depression severity in cases with major depressive disorder. Exploring pathobiology of MDD is essential in the investigation of yoga as a potential therapy for major depression. Although the sample size was small, findings from our study contribute RCT data regarding clinical benefits of yoga and the potential biological mechanisms in MDD. Our trial is distinct from many previous yoga trials by including all limbs of classical yoga based on the yoga sutras (principles) of Patanjali. Such protocols facilitate the expansion of therapeutic options that can provide not only optimum remission but also promote long-term positive health and longevity. YMLI is a profound science of wellbeing which is designed in line with ‘the family traditions’ passed on through generations in Indian society. It can, therefore, be easily integrated as a way of life and reach a wider population, approximately a third of which is affected by depression.
Limitations
The sample size in our study was small and included adult group only, limiting its generalizability to other age groups. MDD is a heterogeneous disorder with several endophenotypes and specifiers, and our analysis did not include these because of small sample size. Limitations to the interpretation of data in this paper include the single time-point at which the two groups were differentiated, and not reporting longer-term follow-up effects.
Conclusions
Short term yoga- and meditation-based lifestyle intervention in MDD decreased clinical severity in association with an increase in neuroplasticity, by significantly improving brain physiology, MBC, and cellular health. Our study suggests that increased neuroplasticity may be part of underlying biologic mechanisms to decrease clinical severity in MDD. Moreover, it may prevent complications that are related to drug therapy, reduce relapses and provide long-lasting clinical remission. It may also increase cognitive reserve to decrease the risk of dementia and increase functional reserves to decrease risk for age-related chronic medical conditions. Thus it can be considered as a significant component of integrative health strategy in the prevention and management of MDD and increase both healthspan and lifespan.
Competing interests
The authors have declared that no competing interests exist.
Footnotes
Acknowledgments
We thank the participants for their dedicated participation in the study. Authors sincerely thank yoga instructors Amit Tomar, Sudheer Chaudhary, and Sneha. This study was supported by the ICMR (Grant number: 54/3/GER2014NCD11).