
Abstract
BACKGROUND:
Tablet technology is a promising tool for assisting therapeutic strategies in stroke rehabilitation. However, it is not clear whether the basic gestures (e.g. click, double-click) are feasible.
OBJECTIVE:
This study aimed to assess the successful performance of gestures and associated factors.
METHODS:
This cross-sectional study was conducted at a rehabilitation center in Austria. The successful tablet use was checked on a Samsung Galaxy Tab 4 (10.1 Wi-Fi 25.6 cm; 10.1 Zoll) with a specifically developed app. To identify factors associated with successful use, impairments in activities of daily living (Barthel index), cognitive functions (Montreal Cognitive Assessment, MoCA), motor functions (Nine-Hole Peg Test), and grip strength (handgrip dynamometer) were assessed.
RESULTS:
One hundred and twenty-nine participants were analyzed, whereof 53.5% had a paretic upper limp and 69.2% were able to perform all gestures with at least one hand. Factors associated with successful use were higher Barthel index (OR: 1.06; 95% CI
CONCLUSIONS:
The majority of stroke patients are able to perform the basic gestures on a tablet with at least one hand, but only few patients with paresis could do them. Gestures like double-clicking and zooming should be avoided when designing apps for rehabilitation, as especially these were found difficult.
Introduction
Worldwide about 15 million people suffer from stroke (ischemic or hemorrhagic) [1]. In stroke survivors, sensorimotor and cognitive impairments as well as aphasia are very common and can have a detrimental impact on activities of daily living as well as health related quality of life [2, 3]. It has been found that 30% to 66% of persons have issues with arm paresis that remains without function 6 months after stroke [4], while in about 50% neuropsychological deficits are presented [5], with approximately 40% suffering from aphasia [6] with a detrimental impact on health care system.
Rehabilitation can help to minimize the post-stroke disabilities. Furthermore, it has been noted that the recovery of functional outcomes is positively correlated with the dose of the applied rehabilitative intervention [7, 8, 9]. Post-stroke therapy should be provided at a high intensity, a high frequency and over long periods of time [7, 10].
In such rehabilitation processes, computerized rehabilitation methods using multimedia and informatics resources to optimize sensorimotor and cognitive compromised performances are gaining interest. Tablets are a novel line of computers controlled by a multi-touch screen. Although the clinical interest in tablet technology using commercially available tablet devices is rising, the evidence is still limited. Recent pilot studies have shown that tablet technologies increase the manual dexterity and cognitive functions in persons with stroke [11, 12]. Additionally, it has been shown that the use of tablets can increase motivation and avoid boredom [13]. Thus, tablets have been suggested as a motivating training tool for persons with stroke who struggle with loss of dexterity [12]. Research has also shown that tablets are feasible in speech-language therapy [6], and the feasibility for home use with fine motor weakness and/or neglect has also been proven [14].
It has been stressed that, when using tablets in persons with stroke, it is important to consider disability-related accessibility and particularly watch at issues like large print, simple language, consistency in tasks, visual simplicity and setting of the user interface [15]. Additionally, for successful use, some basic gestures such as click, double click, press, swipe, flick/fling, spread and pinch are needed. These basic commands are listed in the Touch Gesture Reference Guide [16]. To our knowledge there are only two studies which assess the successful performance of tapping and swiping in persons with stroke with different results [17, 18]. No further examines on basic gestures have been studied. Additionally, no study assesses factors influencing successful tablet use in persons with stroke. Although tablet applications can generally be well implemented in health services of people without motor or cognitive limitations, the aim of this study was to find out if tablet use is also possible in stroke survivors enrolled for rehabilitation programs. Therefore, we investigated the performance of the most common basic gestures needed for tablet use in this patient group. Additionally, putative factors associated with a successful use (e.g. socio-demographic factors; prior technical experience; usability of the system) were evaluated.
Methods
Study design and participants
This monocentric cross-sectional study was conducted at the “Neurologisches Rehabilitationszentrum Rosenhügel” NRZ (Vienna, Austria) from July 2017 to August 2017. To find out if tablet use is possible in stroke survivors enrolled in rehabilitation programs, consecutive stroke patients admitted to the NRZ within the recruitment period, were screened and investigated for motor and cognitive impairments. In all included patients, irrespective of their impairments, successful tablet handling was tested by applying the most important gestures needed for use. Inclusion criteria were: clinically confirmed stroke diagnosis (as classified by ICD-10 codes I60-I64), older than 18 years, given written and oral consent, as well as having sufficient knowledge of the German language.
The study was approved by the Clinical Research Ethics Board of the City of Vienna (EK 17-088-VK), and was performed in accordance with the relevant guidelines of the Declaration of Helsinki, 1964, as amended in Tokyo, 1975, Venice, 1983, Hong Kong, 1989, and Somerset West, 1996 [19]. From all included participants, written informed consent was obtained.
Measurements
For assessing the successful use of the tablet and for assessing factors associated with a successful use, the following measurements and questionnaires were used:
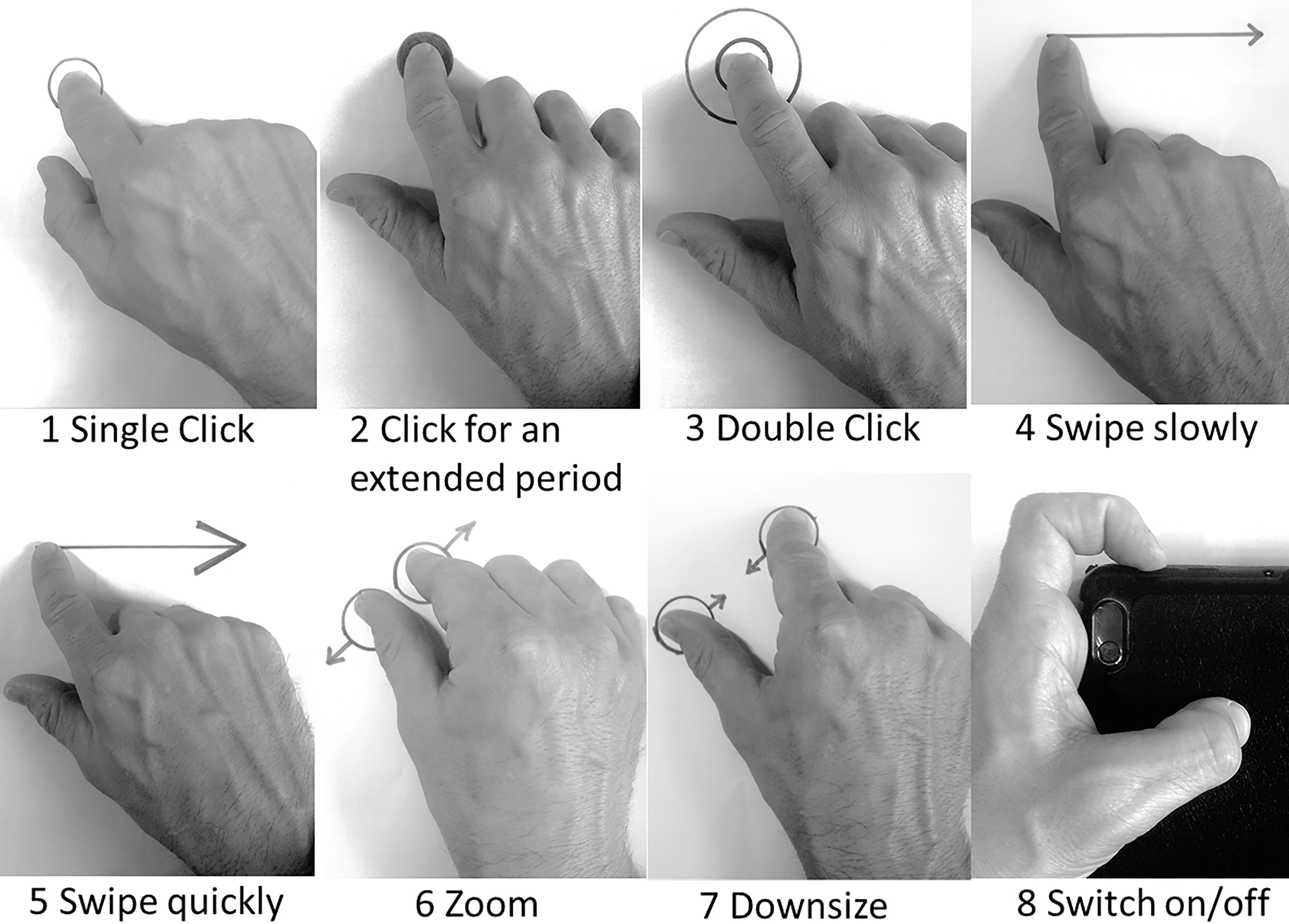
The successful use of the tablet was tested with the tablet Samsung Galaxy Tablet 4 (10.1 Wi-Fi 25.6 cm; 10.1 Zoll). Prior to this study a “Touch Detector test” application, which contained all basic gestures listed in the Touch Gesture-Reference Guide, [16] was developed within a bachelor thesis [20]. This application was developed in Java programming language Android 3.0 operating system using Android Studio for Mac. Participants were asked to conduct the eight basics gestures with both hands (Fig. 1) on the tablet. First, the requested gesture was shown via a video to the participant with an acoustic description. Secondly, they had to perform each gesture 5 times within 30 seconds without any help.
Tasks of the “Touch Detector test” measuring successful performance of the basic gestures. 1: Single Click (tap): a quick up-and-down motion with one finger, lightly striking the screen. 2: Click for an extended period (touch and hold): a down motion with one finger, touching the screen and leaving the finger motionless until the information is displayed or the action occurs. 3: Double click (double tap): two quick taps. 4: Swipe slowly (drag): a slow move from one finger on the screen in the desired direction without lifting it from the screen. 5: Swipe quickly (flick): a quick move from one finger on the screen in the desired direction. 6: Zoom (pinch open): a two-finger gesture used to zoom in by placing the thumb and a finger (or two fingers) close together on the screen and moving them apart without lifting them from the screen. 7: Downsize (pinch close): a two-finger gesture used to zoom out by placing the thumb and a finger (or two fingers) a little distance apart on the screen and moving them toward each other without lifting them from the screen. 8: Switch on/off: a quick press on the switch with one finger with the required strength. Sociodemographic data: Sex, date of birth, living alone, educational level and employment status before stroke were assessed. Disease-related parameters: Time after stroke (month), affected side and evidence of hemispatial neglect was taken from the medical chart. Communication deficits: Aphasia was categorized according to the “National Institutes of Health Stroke Scale” (NIHSS), in “normal language”, “light to moderate aphasia”, ”severe aphasia” and “not able to talk” [21, 22]. Dysarthria was categorized in “light to moderate dysarthria” and “severe dysarthria”. Finally, communication deficits were defined when at least light to moderate aphasia or dysarthria was present. Cognitive function: The Montreal Cognitive Assessment (MoCA) was applied [23]. It is a brief one-page screening tool, which was validated in mild cognitive impairment. Highest possible score is 30 points. People with scores Paresis upper limp: The presence of a paresis was determined by the British Medical Research Council (BMRC). The score was estimated by neurologists. A paresis was rated when the score was Activities of daily living (ADL): The Barthel index was taken from the medical charts. The Barthel index, which was introduced in 1965 [25], consists of 10 questions (feeding, bathing, dressing, bowels, bladder, toilet use, transfers, mobility, stars) and ranges from 0 to 100 points. Motoric function: The Nine-Hole Peg Test (NHPT) was applied [26]. This test is a valid and reliable test to assess dexterity in individuals with stroke [27]. Within this test patients have to put nine wooden pegs into the holes of a peg board, which was placed in front of the patient. One practice trial per hand was conducted prior to the test. Used time was noted in second(s). For baseline characterization the mean duration of the left and right hand was used. Grip strength: For this purpose, the hydraulic handgrip dynamometer Jamar Premorbid use of information technology was assessed by asking the participants about experience with computers, smartphones and tablet computers [29]. The question concerning technology use was: “How often do you use your PC/smartphone/tablet computer?”. The interview guide provided possible answers such as “never, rarely, weekly, and daily”.
Categorical baseline variables as well as data on successful use are shown as frequencies (percentages). Continuous normal distributed data are shown as means (SD
To determine factors associated with a successful use with at least one hand (dependent variable), first, univariate logistic regression models were calculated. Afterwards, a multivariable logistic regression model including all independent variables of the univariate regression analyses with a
To assess factors influencing the successful use with the paretic hand (dependent variable) again univariate logistic regressions with the independent variables which could affect the use (neglect, communication deficits, MoCA score, NHPT and handgrip strength) were calculated. Here, too, a final multivariable logistic regression model including all independent variables of the univariate regression analyses with a
Baseline characteristics
Baseline characteristics
Categorical baseline variables are shown as frequencies (
During the two months enrolment period 166 patients with a clinically confirmed diagnosis of stroke were admitted for rehabilitation at the center. Thirty-seven patients had to be excluded for the following reasons: eight patients (4.8%) were represented by a legal guardian; one patient (0.6%) had severe cognitive deficits; eight patients (4.8%) did not understand the German language sufficiently; 18 patients (6.6%) refused to take part in the study and in two patients (1.2%) rehabilitation was prematurely terminated for clinical reasons. Finally, data from 129 patients, with a mean age of 65.9 (SD: 13.8) years were available for analyses. Further sociodemographic and diseases related parameters can be taken from Table 1.
Successful performance of the basic gestures
Successful performance of the basic gestures
Factors associated with successful performance of the basic gestures with at least one hand
Results are based on univariate logistic regression analyses with the dependent variable successful use with at least one hand. Values are presented in odds ratio (OR) and 95% confidence interval (95% CI).
Table 2 shows how many patients could successfully perform each single exercise with the paretic and the non-paretic hand. Out of the 69 patients who had a hemiparesis of an upper extremity, 18.6% could perform all exercises with their paretic hand, with a variability of 22.5% (zoom) to 35.7% (single click). Double-clicking and zooming were the two most difficult exercises. Successful performance of all basic gestures with at least one hand was possible in 69.2%. Single exercise variety reached from 76.7% (switch on/off) to 100% (single click).
Table 3 shows that in univariate regression analyses successful use with one hand disregarding a paresis was significantly associated with lower age, working before stroke, higher Barthel index, better MoCA score, lower time to perform the NHPT, higher grip strength, and it was also related to the daily use of a computer and a smartphone (Table 3). Results of the multivariable logistic regression model showed that higher Barthel index (OR: 1.06; 95% CI
Factors associated with successful performance of the basic gestures with the paretic hand
Factors associated with successful performance of the basic gestures with the paretic hand
Results are based on univariate logistic regression analyses with the dependent variable successful use with the paretic hand. Values are presented in odds ratio (OR) and 95% confidence interval (95% CI).
Table 4 shows that in univariate regression analyses successful use with the paretic hand was significantly associated with no communication deficits and with a NHPT performed in
Our findings indicated that most, more precisely 76.7%, of stroke patients enrolled in a rehabilitation program were able to perform the basic gestures needed for tablet training with at least one hand, whereas only 18.6% could do all eight tasks with a paretic arm. The characteristics of patients included in the study, are very representative for stroke survivors in rehabilitation programs offered in our center.
Looking at the successful performance with the paretic arm in more detail, 35.7% were able to tap with the paretic arm, which is a considerable lower percentage compared to the study of Kizony et al, showing that 75% were able to complete a tapping game [18]. Reasons for this difference might be that they had with 18.3 (SD: 6.5) kg higher handgrip values and they also showed better results in the NHPT. This leads us to the conclusion that they have included stroke patients who were less affected. Additionally, taping was assessed in a different way: The participants of Kizony et al. had to hold their thumb on an anchor shape while they tapped with different fingers on colored shapes. Another study, looking at the performance of taping and swiping in 87 hemiplegic patients, showed a comparable success rate in taping (38%) and swiping (48%). The authors of this study also tested a self-invented adapter and they concluded that a grip-control might be a good way to gain accessibility in motor training exercises for the severely affected hand [17]. As in our study the success rate of the paretic arm was also low, our results underline the necessity of grip-controllers in this sample. The fact that only 50% of patients with a significant paresis regain the function of the arm, further emphasizes this recommendation [31]. For the successful use with the paretic hand, the NHPT was the only detector, indicating that people who are able to perform the NHPT are also likely to use a tablet. Consequently, the dexterity of the paretic hand plays a relevant roll in successful use.
Tablet technology might not only be used for motor training, but also for cognitive or communication training [32, 33]. In these cases, people could simply use the touchscreen with their not affected arm. As the results of the present study showed that double-clicking and zooming was difficult, these gestures should be taken into consideration in future developments for stroke patients. On the one hand they could be diminished to gain feasibility. On the other hand, these gestures could be enhanced for training of dexterity. The fact that lower age, higher Barthel index and higher MoCA score were associated with successful use with at least one hand were predictable. Apart from that it is expectable that a paretic arm is related to a lesser likelihood of successful use. As these four parameters resulted in a satisfactory AUC, the model can be seen as a good predictive utility. Surprisingly, premorbid use of information technology did not remain in the final multivariable model. Hence, tablets can also be used in people without prior experience with technology.
In this context is has to be mentioned that the present study neither examines the motivation to use tablets at home nor looks at the usability of one single app. Nevertheless, whenever stroke patients conduct any kind of self-training on a tablet, like it was done in the Rehab@Home framework (insoles, estimating gait parameters, which are linked to a tablet PC) [32, 33], or like it was done in the “Rehab-let” protocol [11], the users have to be able to perform the basic gestures.
The major strength of the study was that the successful performance of the basic gestures was assessed for the first time. Therefore, our results can be seen as groundwork for further developments in tablet applications. As we have had to exclude only a few participants who could not participate or refused participation, the results indicated that the tablet technology might be feasible in exactly this population that is subject of most rehabilitation measures.
The major limitation is that the “Touch Detector test” was not validated in healthy subjects. However, there is no other assessment tool available and this test reflects the basic skills of using a tablet. A further limitation might be that we were not using a learning paradigm to see if the participants can learn how to perform more difficult gestures. Additionally, we have not tested the acceptance of the technique and the adherence to tablets. However, this was not the aim of the study. The results should not be generalized to the whole population of stroke survivors as our sample consists of patients specifically referred to for neurorehabilitation and are probably less severely affected than the general population of stroke survivors.
Conclusions
This study was performed to emphasize the use of tablet technology in the rehabilitation process of stroke survivors. Data showed that only few patients with motor limitations of the hand were able to perform all basic gestures, which are important to use this kind of technology. However, the majority of stroke patients and also survivors with aphasia and cognitive impairments can perform the basic gestures to use a tablet with at least one hand. Thus, tablet technology might be a tool to expand the variety and intensity of stroke therapy. Moreover, double-clicking and zooming should be avoided, as these basic gestures were particularly difficult to perform. The present results should be taken into account when programming further applications for stroke patients. Further evaluation on the impact of tablet technology on patient outcome and adherence is required. It should also be examined if these patients could use tablets after discharge independently. Therefore, the results show that tablet technology might be a considerable tool in stroke rehabilitation and factors which are important for this use in stroke survivors were pointed out for developers of these apps.
Footnotes
Acknowledgments
The authors would like to extend their gratitude to Stefanie Schmidt and Ursula Rumpler for data acquisition, to Marvin Reinprecht for assistance with the figure and to the Neurologisches Rehabilitationszentrum Rosenhügel, Vienna, Austria for funding the publication fee.
Conflict of interest
None to report.