
Abstract
BACKGROUND:
Transapical off-pump mitral valve (MV) repair is a novel minimally-invasive surgical technique, allowing to correct mitral regurgitation (MR) caused by chordae tendineae rupture. While numerical simulation of the MV structure has proven to be useful to evaluate the effects of the MV surgical repair techniques, no numerical simulation studies on the outcomes of transapical MV repair have been done up to now.
OBJECTIVE:
The purpose of this study is to evaluate the transapical MV repair using finite element modeling and to determine the effect of the neochordal length on the function of the prolapsing MV.
METHODS:
The reconstruction of the MV geometry based on the patient-specific data was performed. In order to simulate prolapse, chordae inserted into the middle segment of the posterior leaflet (P2) were ruptured. A total of four virtual transapical repairs using neochordae of different length were performed. The function of the MV before and after virtual repairs was simulated.
RESULTS:
The evaluation of the effect of the neochordal length on post-repair MV function showed that the length of the implanted neochordae has a significant impact on the correction of MR caused by chordae tendineae rupture.
CONCLUSIONS:
The presented results can improve the understanding of the effects of transapical MV repair.
Introduction
The mitral valve (MV) separates the left atrium (LA) from the left ventricle (LV) and ensures unidirectional blood flow during the cardiac cycle. It is a complex cardiac structure composed of the valve annulus, the valve leaflets (anterior and posterior), the chordae tendineae and the papillary muscles (PMs) (Fig. 1). Each leaflet of the valve can be divided into 3 segments: lateral, middle and medial, as proposed by Carpentier [1], thus allowing a precise description of the location of the valve dysfunction. Both leaflets are anchored to the PMs by cord-like tendons which are called the chordae tendineae. Studies on the chordae tendineae have distinguished different types of the chordae by their location of insertion into the leaflets: (a) marginal chordae are inserted into the free margin of the leaflets; (b) basal chordae are found near the annular attachment; and (c) strut chordae attach PMs to the central parts of the leaflets [2, 3].
Anatomy of the mitral valve.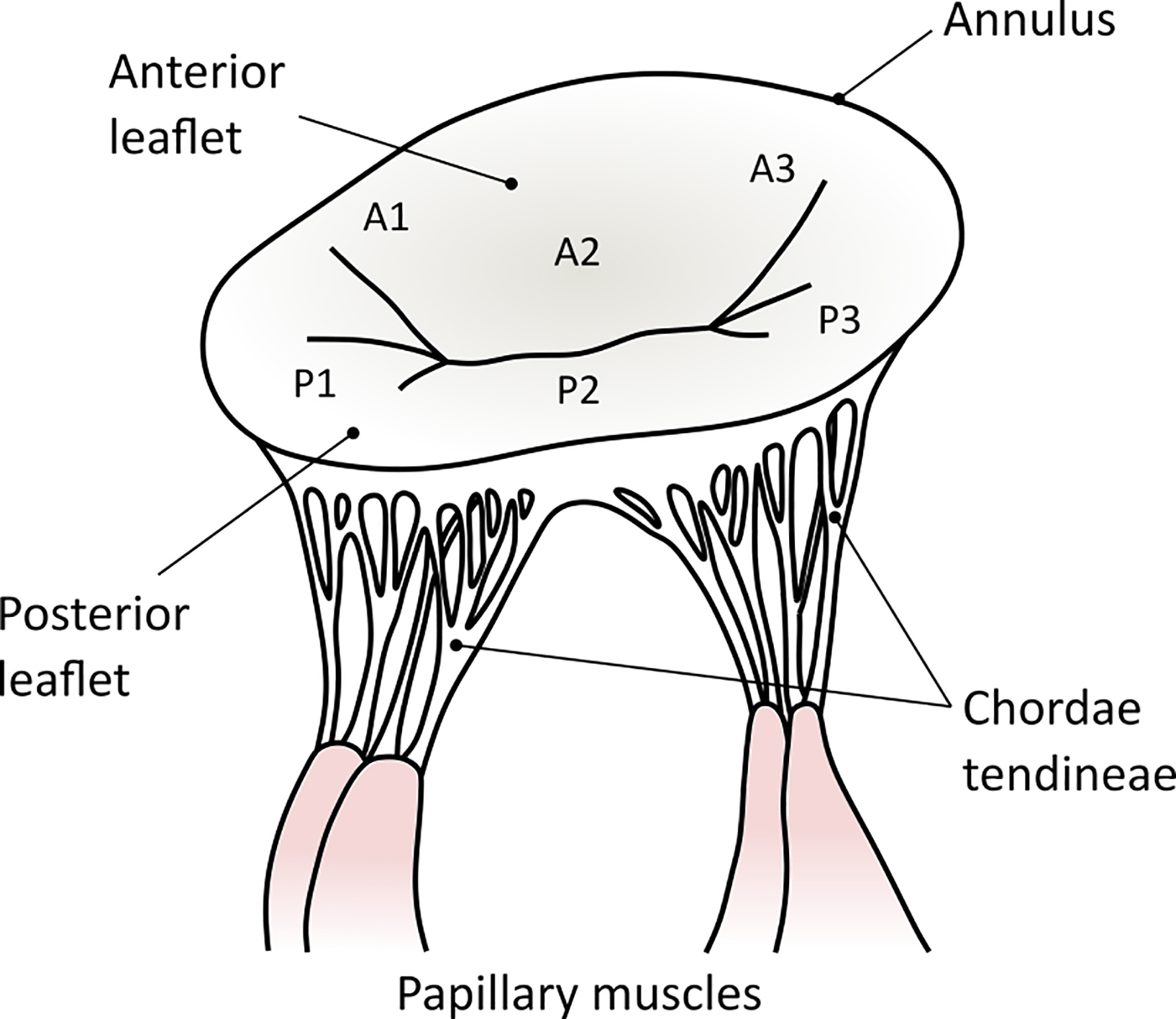
During the diastole, the MV opens as a result of increased pressure in the LA as it fills with blood. The blood then flows to the LV. The chordae tendineae are relaxed during the diastole because the MV is opened. The diastole ends with atrial contraction and the leaflets close thus preventing the backflow of the blood into the LA. Since the pressure in the LA becomes much lower than in the LV, the leaflets attempt to evert to the lower pressure region. The chordae tendineae prevent this eversion, called prolapse, by becoming tense and holding the leaflets in the closed position.
MV prolapse is a condition in which the MV does not close smoothly but instead one or both leaflets bulge upward into the LA. This is occasionally due to the rupture of the chordae tendineae that support the MV [4]. In some cases, the prolapsed MV lets a small amount of blood flow backward from the LV into the LA. This disorder is called mitral regurgitation (MR). If mild, MR may not cause problems, however, severe MR can lead to a life-threatening emergency including pulmonary congestion and heart failure. The severity of MR generally depends on the number and location of the ruptured chordae. A single ruptured chorda may lead to mild MR which requires no treatment, while the multiple chordae ruptured simultaneously can cause severe MR [5]. The rupture of the marginal chordae almost always leads to severe MR, while the ruptured basal chordae are usually not critical [6].
The underlying causes of chordae tendineae rupture include subacute endocarditis, rheumatic heart disease, myxomatous degeneration and other heart and valvular diseases [5]. Mechanical properties of diseased chordae are significantly different from those of normal chordae [7], therefore the rupture occurs when the strain forces exceed the stretching threshold of the diseased chordae [5].
MR caused by chordae tendineae rupture is typically corrected by the chordae replacement with expanded polytetrafluoroethylene (ePTFE), also known as Gore-Tex, sutures [8]. These sutures appear to be a good material for the synthetic chordae replacement because of their biomechanical properties, similar to those of the natural chordae [9].
A variety of surgical techniques for the chordae replacement are available [10]. The most common technique for replacing the ruptured chordae with the neochordae is called the loop technique. This technique uses a set of premade ePTFE suture loops which are anchored to the PM and then used to re-suspend the prolapsing segment of the leaflet [11]. The disadvantage of this technique is that during the surgery the heart is stopped and the cardiopulmonary bypass pump takes over the work of the heart and the lungs. Another disadvantage is that the required length of neochordae is obtained by a process of trial and error, therefore the heart may have to be stopped and restarted few times during the surgery [10].
Recently, a new technique of neochordae implantation was introduced. NeoChord DS1000 device enables off-pump (also called “beating-heart”) transapical implantation of neochordae. The device is passed into the beating heart through a small incision and advanced through the MV into the LA under echocardiographic guidance. A grasping mechanism with a semi-dull needle on the tip of the device is used to anchor the neochordae to the prolapsing segment of the leaflet. The neochordae are then secured under proper tension to the LV apex [12].
While transapical implantation of neochordae shows promising clinical results [13, 14], it requires additional experience and further studies. Some aspects of this technique, such as exact positioning of the neochordae to the prolapsing segment or the length adjustment of the neochordae to eliminate prolapse while preventing additional restriction of the leaflet, can only be assumed at this moment [15]. Therefore, the use of a numerical simulation to clarify these aspects should be considered.
Numerical simulation of the MV structure based on the patient-specific data has proven to be useful to evaluate the effects of the MV surgical repair techniques [16]. However, only a few studies on the numerical simulation of the MV repair with neochordae implantation were published [17, 18, 19, 20, 21]. Moreover, none of them has addressed the problem of the transapical MV repair.
Therefore, the purpose of this study is to evaluate the transapical MV repair using finite element modeling and to determine the effect of the neochordal length on the function of the prolapsing MV.
Data acquisition
Echocardiography has become routinely used in the diagnosis, management, and follow-up of patients with any heart disease. Transthoracic echocardiography (TTE) is the most common type of echocardiography for the assessment of morphology and geometry of the MV, which provides accurate quantification of valvular dysfunction [22]. During TTE, the ultrasonic transducer is placed on the chest of the subject to get various real-time views of the heart.
The data of the movement of the non-prolapsing MV at the heart rate of 66 bpm, characterized by a 22 Hz time-frequency, was obtained during TTE using Vivid e95 (GE Healthcare) ultrasound machine. The acquired data set was stored as a volumetric medical image (VolDICOM) and exported for further processing.
Image processing
The reconstruction of the MV geometry was performed using the custom platform developed in MATLAB (Mathworks) by Biomechanics Research Group of Politecnico di Milano (Italy) [23]. The procedure consisted of the following steps: (1) positioning of the coordinate reference system into the VolDICOM; (2) generation of the radial planes; (3) manual tracing of the positions of the MV and the PMs; and (4) reconstruction of the 3D MV geometry. Afterward, the input file for the analysis in Abaqus/Explicit (Dassault Systèmes) was prepared.
The XYZ coordinate system was positioned into the acquired VolDICOM so that Z axis would connect the LV apex and the MV centroid, while X and Y axes would be perpendicular to the MV annular plane, thus creating two long-axis (ZX and ZY) and one short-axis (XY) planes. By rotating a long-axis plane by 10 degrees along Z axis, 18 radial planes were generated.
The end-diastole (ED) was chosen as the initial state for the analysis since at this point in time the MV can be assumed as approximately unloaded [23]. The positions of the MV annulus and free margin were manually identified on every radial plane during the ED. For each leaflet, the identified points were interpolated with a cubic spline of 32 points, uniformly distributed along the length of the leaflet (Fig. 2a). By fitting the 4th order Fourier approximation function to these points, a 3D point cloud was generated, consisting of 32 levels running from the annulus to the free margin, each with 200 points, uniformly distributed along the circumference of the MV (Fig. 2b).
Reconstruction of the MV geometry: tracing the positions of the MV leaflets (a); 3D point cloud of the profile of the leaflets (b); complete 3D model of MV and chordae tendineae (c).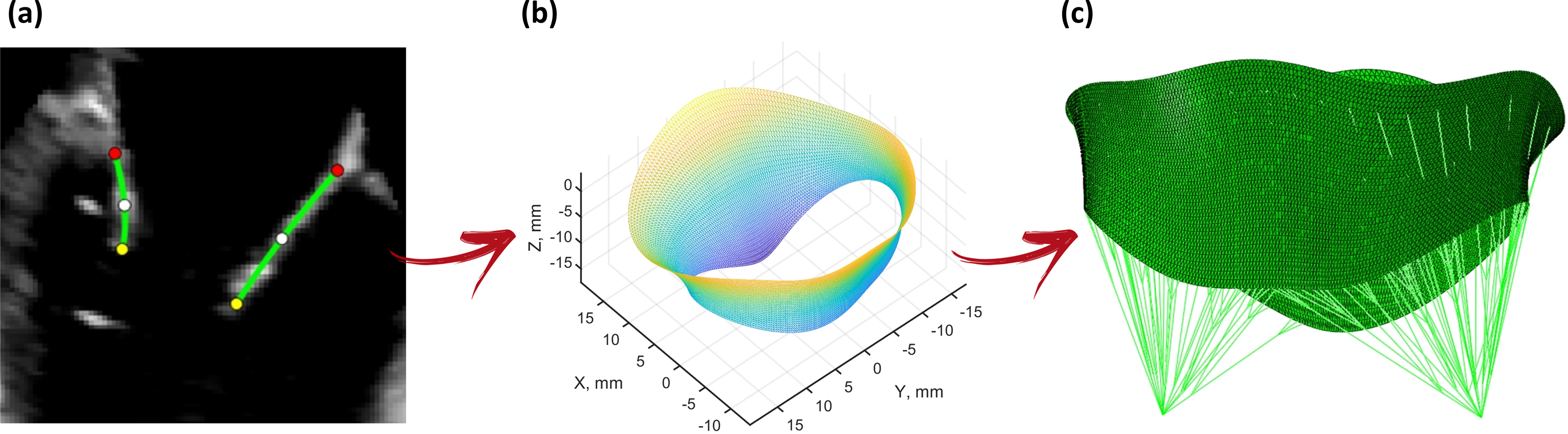
The created points were connected into a mesh of 3-node shell elements (type S3R in Abaqus). Regionally varying thickness was assigned to the leaflets, as suggested by Kunzelman et al. [24], with an average value of 1.32 mm for the anterior leaflet and 1.26 mm for the posterior one.
In addition, the points of the PM tips were manually traced during the ED. A branched network of the chordae tendineae of three orders, i.e. marginal, basal and strut, was created, connecting the PM tips and the valve leaflets (Fig. 2c). The number of the chordae and their insertion points on the leaflets were determined in accordance with ex vivo study by Lam et al. [2] and indications by clinicians [25]. The marginal, basal and strut chordae were modeled as truss elements (type T3D2 in Abaqus) with constant cross-sectional area values of 0.40, 0.79 and 1.15 mm
Structurally, the tissue of the MV leaflets is composed of collagen, elastin and muscle fibers. Such tissue demonstrates higher stiffness along the collagen fiber direction compared with the cross-fiber one. Since collagen fibers are oriented along the longitudinal direction (i.e. parallel to the annulus) of the leaflets, the mechanical response in this direction is stiffer than in the transversal one (i.e. perpendicular to the annulus). Therefore, the mechanical behavior of the MV leaflets was assumed non-linear and anisotropic, and described through a constitutive model, proposed by Lee et al. [26]:
where
Constitutive parameters of the tissue of the MV leaflets
Constitutive parameters of the tissue of the MV leaflets
The mechanical behavior of the chordae tendineae was assumed non-linear and isotropic. It was described as hyperelastic strain energy functions available in Abaqus material library: (1) 2nd order polynomial model for marginal and strut chordae; and (2) 5th order Ogden model for the basal chordae. The corresponding constitutive parameters were defined by fitting uniaxial test data, reported by Kunzelman and Cochran [3].
PM tips were modeled as nodes without physical properties.
In order to incorporate patient-specific kinematic boundary conditions, the motion of the MV annulus was manually traced for the time frame between the ED and the peak systole (PS) as described previously. The annular contraction was modeled by applying nodal displacements to the points of the annulus identified at ED. The same procedure was performed to model the movement of the PMs – the motion of the PM tips was manually traced during the same time frame, and the nodal displacements to the points identified at the ED were applied (Fig. 3a).
A time-dependent physiologic transvalvular pressure curve with values increasing from 0 mmHg during the ED up to 119 mmHg during the PS (Fig. 3b) was applied on the ventricular surface of the leaflets.
Motion of the annulus and the PM tips extracted from imaging data (a); time-dependent transvalvular pressure curve applied to the leaflets (b).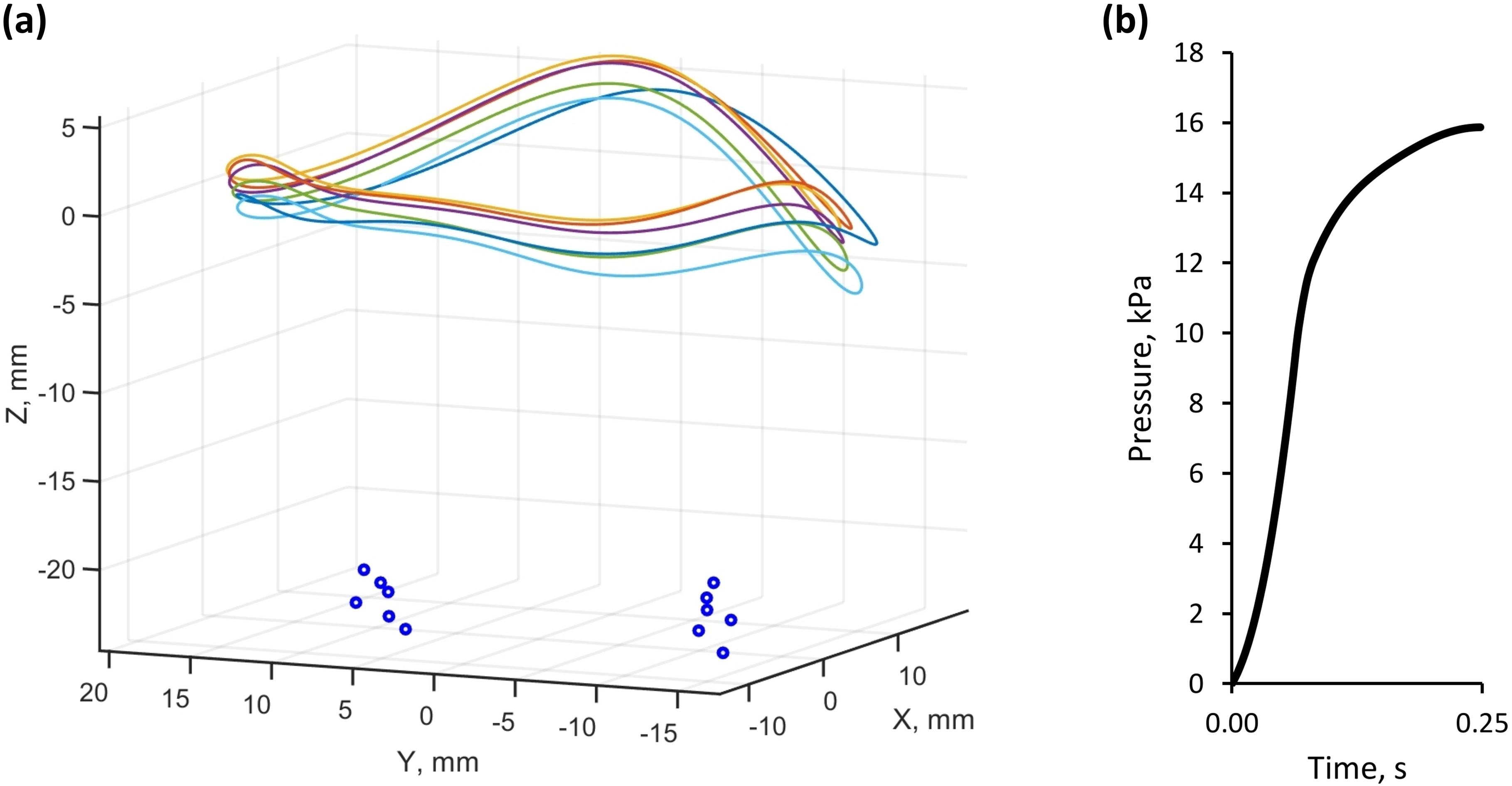
Contact was modeled for the atrial side of the MV leaflets, using a general contact algorithm available in Abaqus, with scale penalty method and the friction coefficient of 0.05 between the leaflets.
The most common segment involved in the MV prolapse is the middle segment of the posterior leaflet (P2) [28]. In order to simulate prolapse of the MV, marginal and basal chordae inserted into the P2 segment were ruptured.
The position of the LV apex was manually traced during the time frame between the ED and the PS, and the apex movement was modeled by applying nodal displacement to the apex position identified at the ED. Virtual transapical repair of the MV was then performed, connecting the prolapsing segment of the leaflet and the LV apex with the neochordae.
In general, implantation of more than two neochordae is desired to balance a load per suture and to provide structural support as needed. Early clinical results show that three to six ePTFE CV-4 type sutures with a diameter of 0.307 mm are usually implanted, and the implantation of four neochordae is the most common case [14]. Therefore, virtual transapical repair using four neochordae, evenly distributed along the free margin of the P2 segment, was planned (Fig. 4). In order to evaluate the effect of the neochordal length on post-repair MV function, a total of four virtual repairs using sutures of different length were performed. In the first case, four neochordae were added between the LV apex and the P2 segment without changing their lengths, while in the next three cases the lengths of the sutures were increased by 5%, 10%, and 15% respectively. The neochordae were modeled as nonlinear truss elements (type T3D2 in Abaqus) and their mechanical behavior was described using 2nd order polynomial model. The constitutive parameters were defined by fitting uniaxial test data, reported by Dang et al. [29].
Virtual transapical repair using four neochordae with 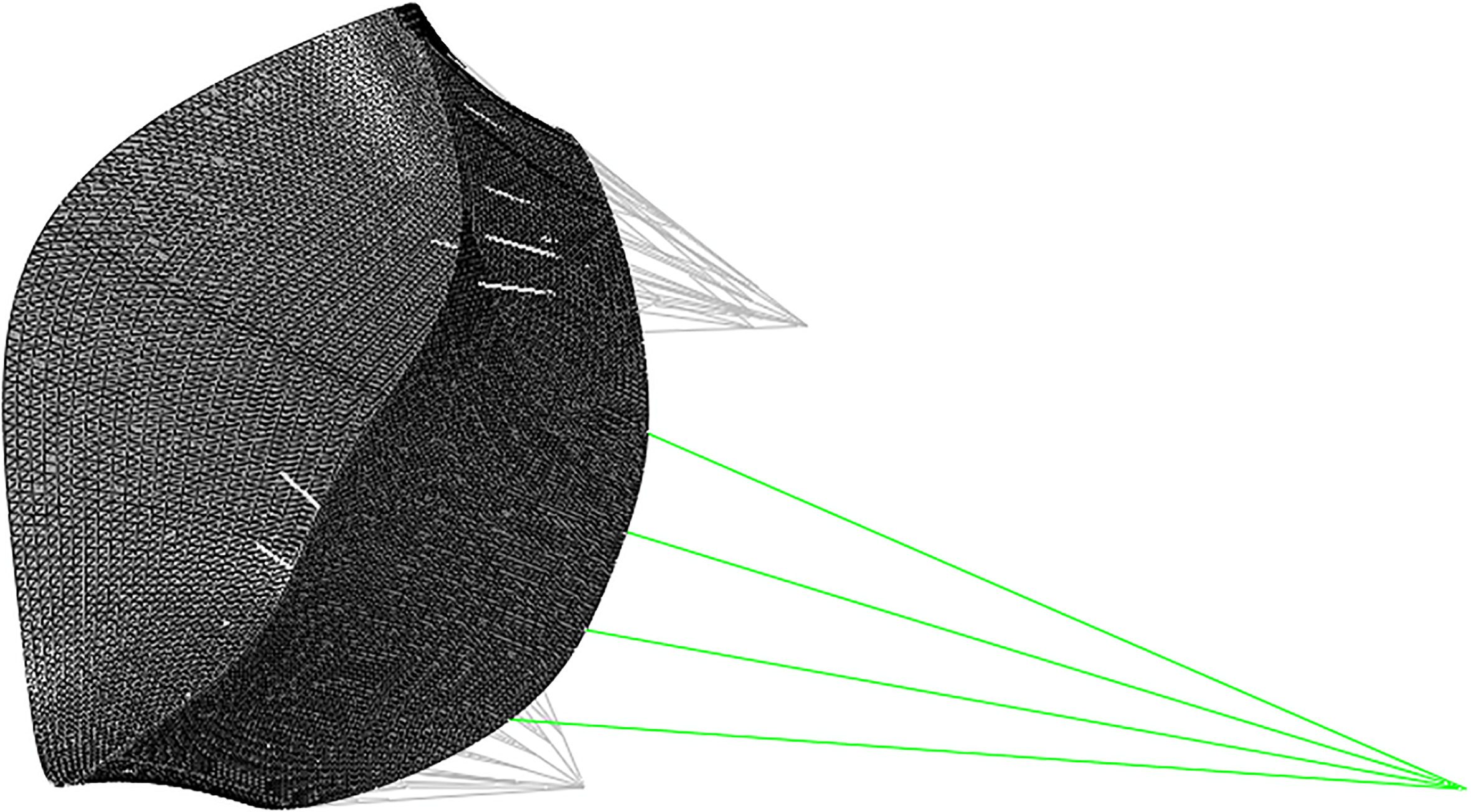
The time-dependent boundary conditions were applied and the function of the MV before and after virtual repairs for the time frame between the ED and the PS was simulated in Abaqus/Explicit.
Simulated post-repair MV functions were compared with the function of the MV prior to virtual repair and evaluated in terms of several aspects: (1) coaptation area of the leaflets, i.e. the area of each MV leaflet in contact with the opposite leaflet; (2) coaptation length, as the length of the leaflet apposition measured on septal-lateral diameter of the MV; (3) tenting height, defined as the distance from the coaptation point to the annular plane measured on septal-lateral diameter of the MV; (4) stress distribution across the leaflets; and (5) chordal stress distribution.
Coaptation area prior to virtual repair (a) and after implantation of neochordae with 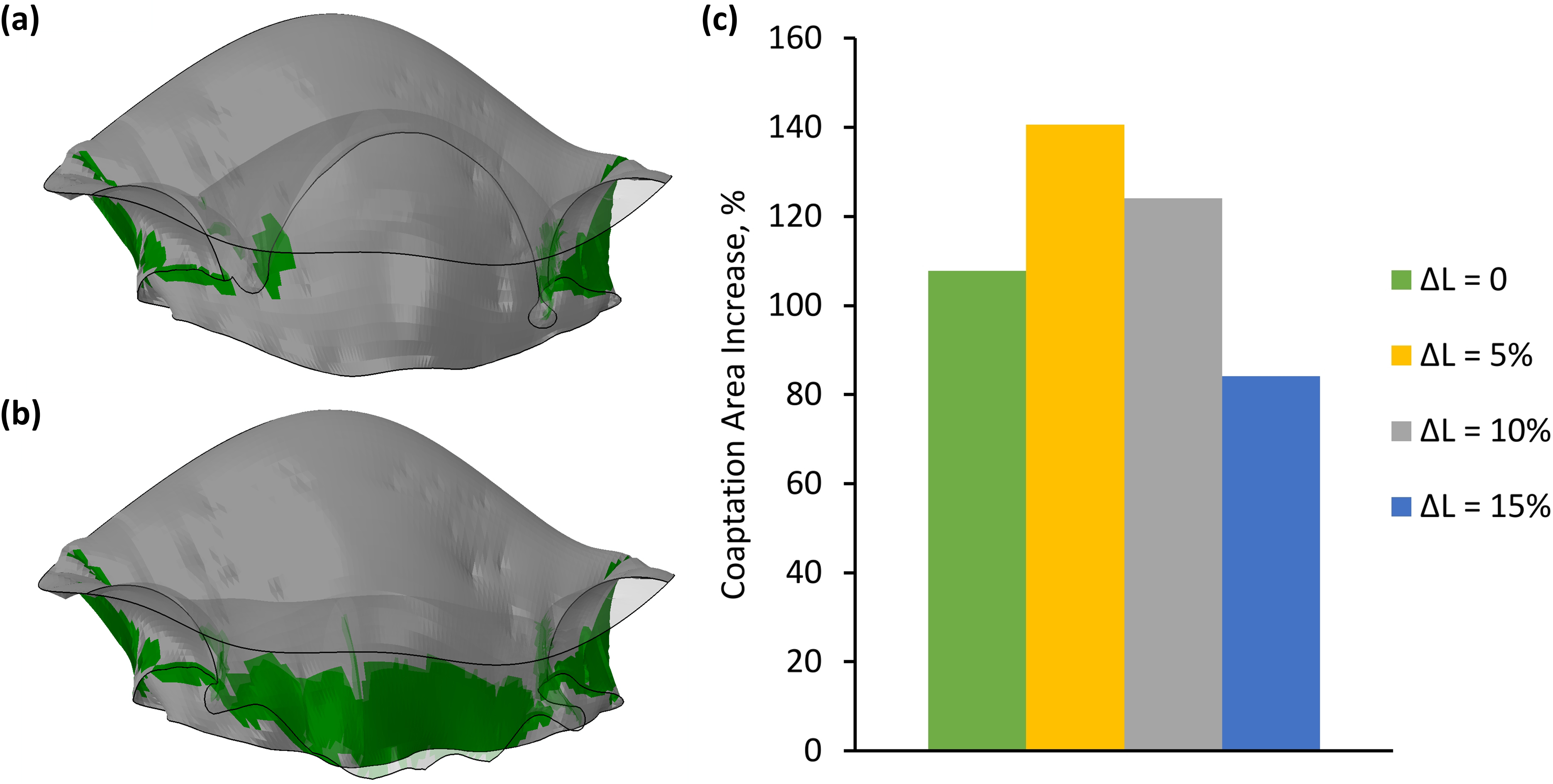
No leaflet contact on septal-lateral diameter in the prolapsing MV (a); coaptation length and tenting height after virtual repair (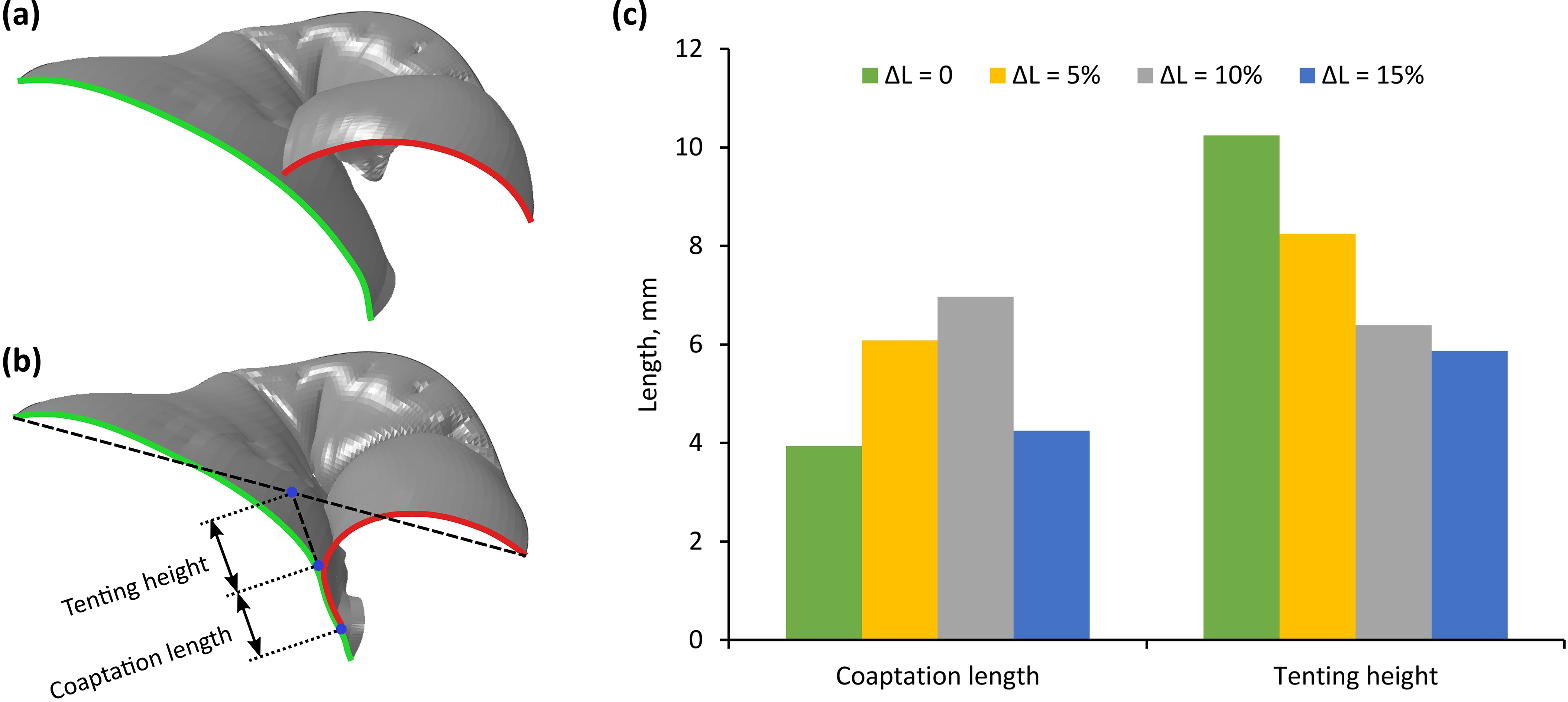
All virtual repair procedures eliminated prolapse and significantly increased the coaptation area (Fig. 5). The smallest increase of this area by 84.2% was obtained after the implantation of the longest neochordae (
As the MV prior to virtual repair was prolapsing, the leaflets on septal-lateral diameter were not in a contact, so there was no actual coaptation length. Therefore, all virtual repair procedures restored the different level of the coaptation length, ranging from 3.9 mm (neochordae with
The tenting height in each post-repair MV depended inversely on the length of the neochordae – the longer the sutures were used, the smaller the tenting height was, and vice versa (Fig. 6).
Stress distribution across the leaflets at peak systole.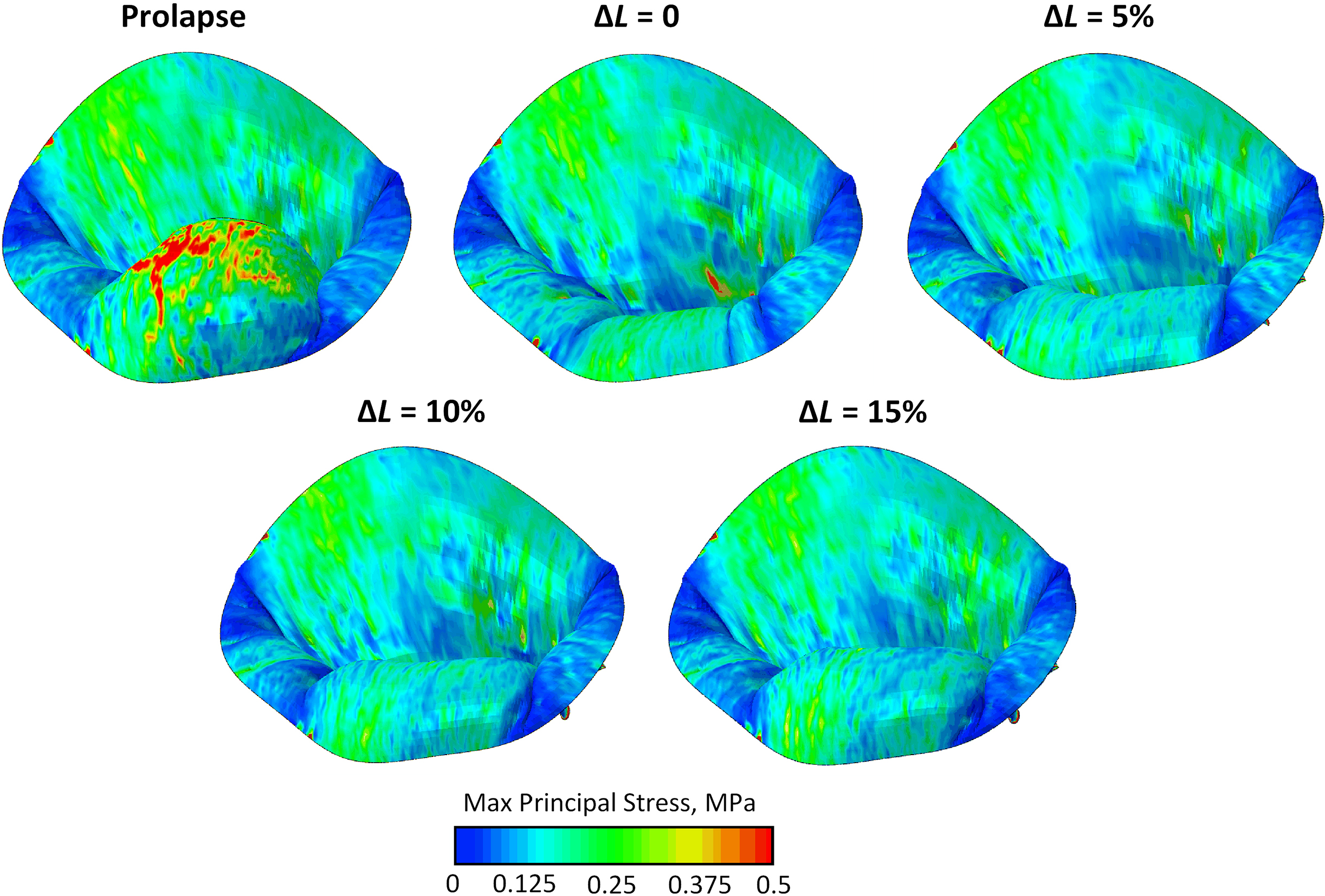
Comparison of maximum principal stresses on posterior leaflet, native chordae, and neochordae at peak systole.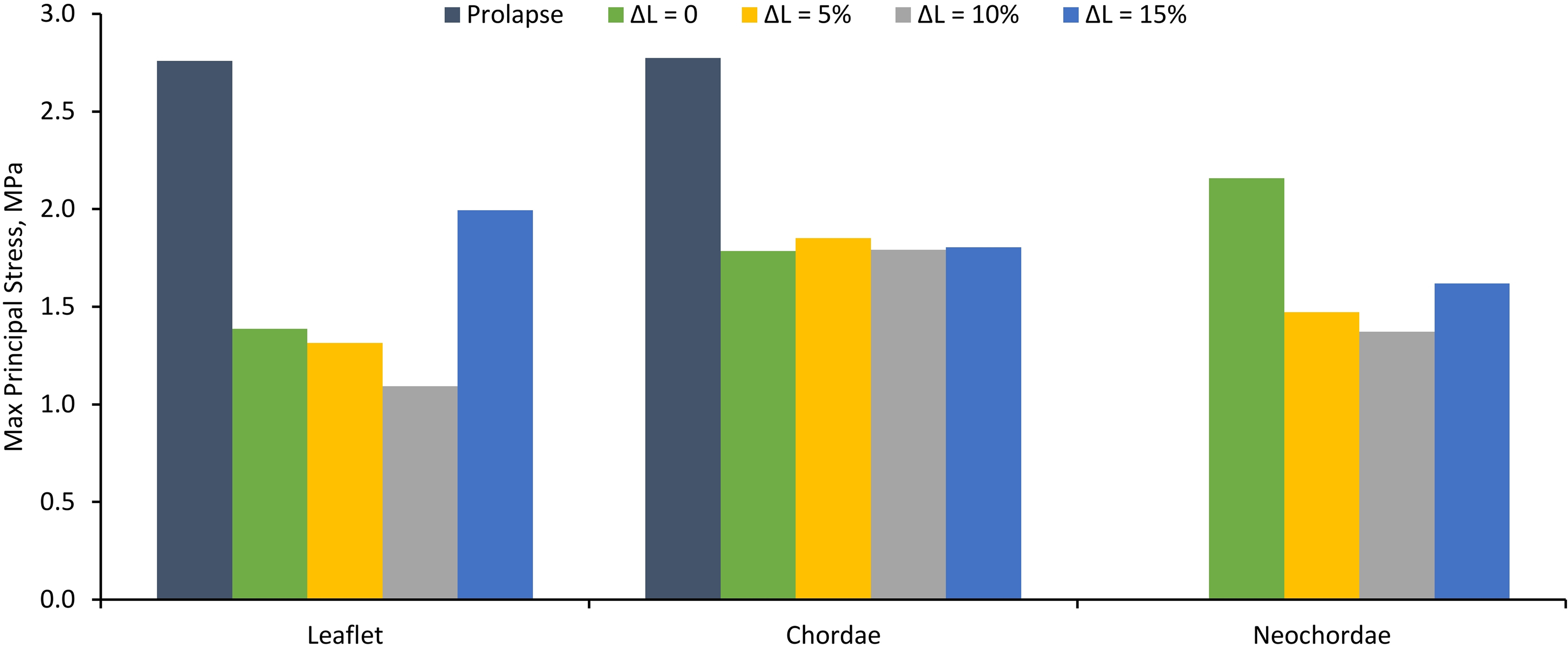
While the virtual repair procedures haven’t influenced stress distribution across the non-prolapsing segments of the MV much, stresses on the prolapsing segment changed considerably compared with the MV prior to virtual repair. Large maximum principal stress concentration on the P2 segment was reduced in all post-repair cases (Fig. 7), although stresses slightly increased along the free margin of the segment near the attachment points of the neochordae. This increase was inverse to the length of the neochordae – highest stress values occurred after the implantation of the shortest neochordae (
The maximum stress value of 2.77 MPa during the PS occurred on the native marginal chordae neighboring the prolapsing P2 segment of the MV prior to virtual repair. In all post-repair cases, this value was reduced as stress was partially transferred from native chordae to neochordae (Fig. 8).
The MV repair using chordae replacement with ePTFE sutures has become widely used for correction of MR caused by chordae tendineae rupture [10], thus inducing the interest in the numerical simulation of this surgical technique [17, 18, 19, 20, 21].
The desire to perform chordae replacement through minimally-invasive approach encouraged to emerge new technique of MV repair, allowing transapical off-pump implantation of neochordae [30]. As this technique relies solely on the echocardiographic determination of the proper length of the neochordae [10], the numerical simulation could be used to evaluate the effect of the neochordal length on the post-repair MV function. However, though this surgical technique was introduced in 2009 [31], no numerical simulation studies on the outcomes of such procedure have been done up to now.
In the present study, the effects of transapical MV repair were investigated, in particular, the effect of the neochordal length on the function of prolapsing MV. Virtual repairs using sutures of different length (
While all virtual repair procedures considerably increased the coaptation area, the coaptation length on septal-lateral diameter was insufficient after the implantation of the shortest (
Moreover, patients with the tenting height of more than 10 mm can be identified as high-risk patients [33]. After the implantation of the shortest neochordae, the obtained tenting height of 10.2 mm slightly exceeded this limit, while in all other cases the tenting height was lower than the specified value.
These results showed that after the implantation of the shortest neochordae the movement of the PL was partially restricted, thus preventing adequate leaflet apposition. On the other hand, the implantation of the longest neochordae caused the opposite effect – the movement of the PL was not restricted enough and some bulging remained, therefore, though tenting height became adequate, the coaptation length stayed insufficient. Meanwhile, neochordae with
Stress analysis of the prolapsing MV showed large maximum principal stress concentration on the bulging section of the P2 segment and on the native marginal chordae neighboring this segment. Such excessive stresses over a longer period of time can cause an additional chordal rupture [18]. All virtual repair procedures reduced these excessive stresses. After the implantation of the neochordae with
To sum up, the evaluation of the effect of the neochordal length on post-repair MV function showed that the length of the implanted neochordae has a significant impact on the correction of MR caused by chordae tendineae rupture. Therefore, special consideration on the length of the sutures should be given, as implantation of either too short or too long neochordae can result in inadequate post-repair MV function.
Conclusions
The current study introduced computational evaluation of the outcomes of transapical MV repair. Simulation of post-repair MV function demonstrated eliminated MV prolapse, restored leaflet coaptation and reduced stresses on the prolapsing leaflet and native chordae. The presented results can improve the understanding of the effects of transapical MV repair.
Footnotes
Conflict of interest
None to report.