
Abstract
BACKGROUND:
Even though the importance of leg length discrepancy (LLD), with its potential of causing several pathological conditions or gait deviations, is well known, measuring LLD is still challenging with limited reliability and validity.
OBJECTIVE:
To assess the capability of the dynamic leg length (DLL) measurement in detecting the presence of anatomic LLD.
METHODS:
A lower limb x-ray was performed on 15 participants with suspected LLD in addition to a gait analysis study using a motion analysis system to measure DLL (the absolute distance from the hip joint centre to the heel, to the ankle joint centre and to the forefoot). Average DLLs were compared between sides for symmetry by the paired
RESULTS:
No significant differences in DLLs between sides throughout the gait cycle were found. Significant differences between sides were found between the maximal stance and minimal swing phase DLLs.
CONCLUSIONS:
DLL measurement is capable of detecting an anatomic leg length difference based on functional changes in leg length and functional discrepancy.
Introduction
Anatomic leg length discrepancy (LLD) is a common orthopedic condition, defined as a structural deformity originating from true bony leg length differences, due to anatomical differences between the lengths of the two limbs from the femoral head to the distal tibia [1]. Anatomic LLD can be congenital or acquired. Congenital conditions include mild developmental abnormalities discovered at birth or childhood and/or various abnormal developmental disorders. Acquired conditions include trauma, fractures, orthopedic degenerative diseases and surgical disorders such as joint replacement. Studies have shown LLD to be very common, occurring in up to 70% of the population [2]. A systemic review evaluating the prevalence of LLD via radiographic measurements, revealed that 90% of the normal population have some differences in bony leg length, with 20% affected by a variance of
LLD has been found to be a significant factor in influencing several pathological and physiological conditions which in turn affect function and quality of life [4]. An association between LLD and foot pathologies [5, 6], low back pain [7, 8, 9], and functional scoliosis in children [10], has been suggested. Some researchers have reported a strong association between LLD and hip and knee osteoarthritis [11]. LLD after a total hip replacement has been found to impair functional outcomes and patient satisfaction [4, 12]. Several studies have also found a higher incidence of stress fractures and running injuries in the lower extremities of athletes with LLD [13].
There is a divergence of opinion in the literature as to the extent of the discrepancy associated with pathological conditions. However, recent evidence has emerged as to the significance of
Despite the importance of LLD as a clinical finding, with its potential of causing symptoms or gait deviations, measuring LLD in a clinical setting is still challenging with limited reliability and validity [19]. Imaging is considered the most reliable and valid method [20], however, it is expensive and exposes the subject to radiation, thereby, its impractical use in a clinical setting. Studies have found LLD to be compensated by dynamic strategies aimed at achieving functional equalizations [1, 14, 21]. Compensatory gait deviations can occur simultaneously in both the longer and shorter lower limb. Compensations of the shorter lower limb during the stance phase, functionally elongates the limb, whereas the longer leg utilizes deviations that functionally shorten the lower limb during the stance and swing phase.
Based on the kinematical compensation for LLD, dynamic leg length (DLL) measurement, a recently proposed method for measuring the dynamic changes in leg length throughout the gait cycle, has been suggested as a means of detecting asymmetry due to LLD [18, 22, 23]. DLL is the dynamic length of the lower extremity and a resultant factor of true bone leg length and lower limb movement during the gait cycle. The aim of the present study was to assess the capability of the DLL measurement in detecting mild anatomic LLD achieved by comparing the impact of anatomic LLD on the biomechanics of the lower limb through DLL measurements.
Methods
Participants
Fifteen participants diagnosed with idiopathic or post traumatic LLD were evaluated in order to determine the need for a corrective heel or shoe lift. The average age was 27 years (SD 13), mass
Measures
Lower limb x-rays for measuring anatomic LLD were performed either by a standing calibrated x-ray using a 2.54 cm metal ball and TraumaCad
Gait data were recorded using a three-dimensional motion analysis system (Vicon
Clinical evaluation was performed by the main investigator to exclude any clinical limitation other than anatomic LLD and included joint range of motion (ROM) and muscle-tendon length measurements (using a plastic goniometer and manual muscle testing) [27].
Design and procedures
Three DLLs were measured as the absolute distance from the hip joint center to the heel marker (HDLL), to the ankle joint center (ADLL) and to the forefoot marker (FDLL) during the gait cycle (Fig. 1) [22]. Virtual trajectories of the hip and knee joint centers were determined by the PGM [27].
a. Hip joint center (HJC) to heel (HEEL) distance during the gait cycle; b. HJC to ankle joint center (AJC) distance during the gait cycle; c. HJC to fore foot (FF) distance during the gait cycle.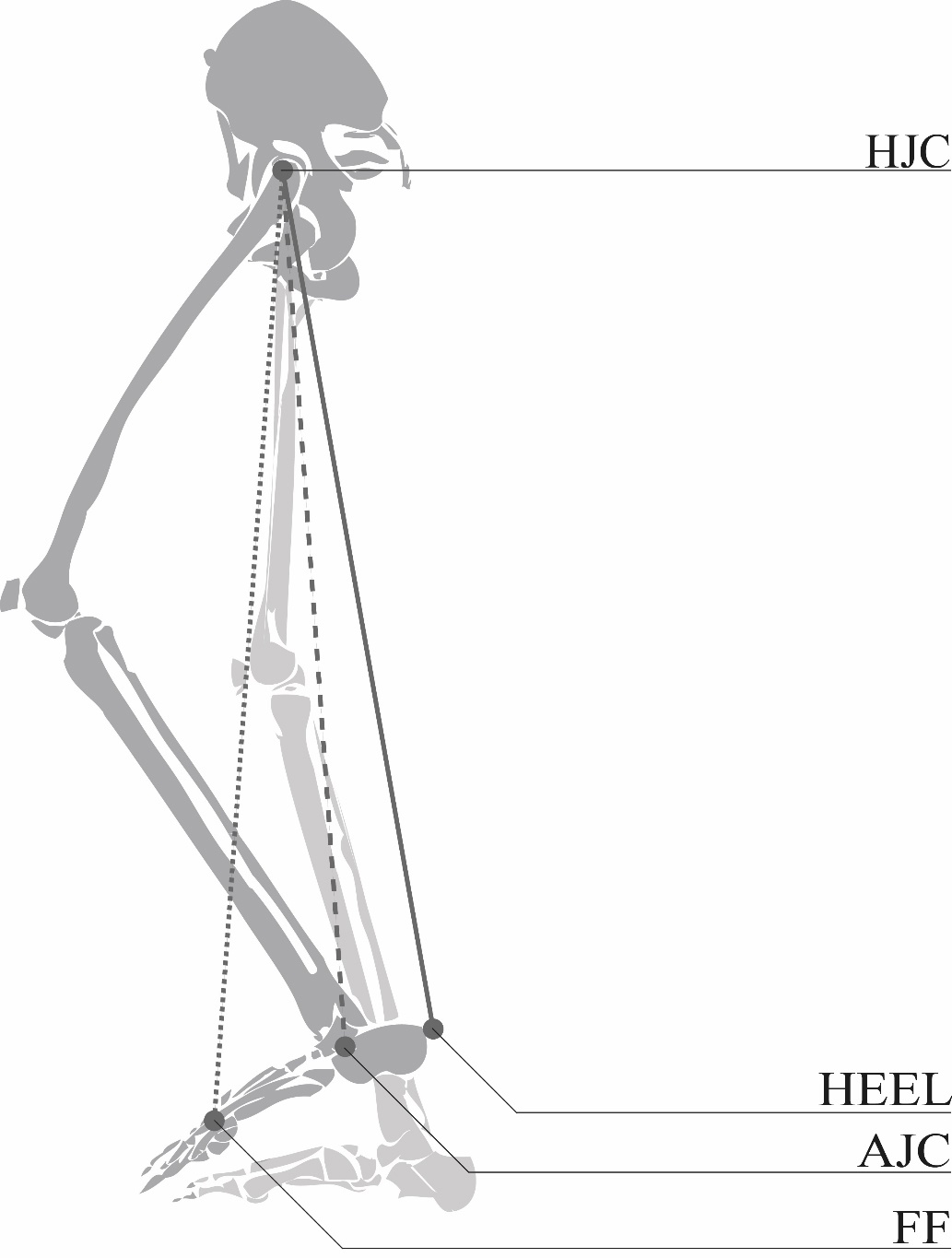
Three DLL components were analyzed:
Differences in DLLs between sides throughout the gait cycle in order to detect time of significant differences for assessment of symmetry [18, 23]; Change in the functional length of each lower limb was defined as the ratio between maximal stance and minimal ipsilateral swing phase DLLs [18, 23]; Clearance index was defined as the difference between maximal stance and minimal contralateral swing phase DLLs in order to evaluate the interaction between sides [18]. The clearance index was determined according to the side of the swing limb and was found symmetrical amongst the 40 healthy participants evaluated in the same gait laboratory [23]; Functional discrepancy was defined as the difference between the right and left clearance indices.
Mid to terminal stance was defined as the stance phase; mid-swing was defined as the swing phase. The maximal stance and minimal swing phase DLLs values were chosen due to the mechanical requirements of gait. These values will be most affected when the maximal functional leg length during stance will be required to clear the contralateral side and the minimal swing phase length will be required to clear the foot off the ground. Our hypotheses was that dynamic equalization would occur with excessive dynamic shortening in the longer leg either during stance, swing or both, with the opposite effect occurring on the shorter limb. We believed that the effect would increase as the LLD increased, with a higher clearance index on the longer side leading to functional discrepancy and a greater change in the functional leg length of both the long and short lower limbs.
The Shapiro-Wilk test, adjusted to the Bonferroni correction for multiple comparisons, tested the normality assumption. Anatomical leg length for both sides, as measured by a standing x-ray or CT scanograms was compared by the paired
Results
Nine participants presented with a significant longer anatomical right lower limb (standing x-rays were performed on six of the participants; a CT scanogram was performed on the other three) (
Adjusted 95% confidence intervals of the mean average difference in DLLs between sides throughout the gait cycle (a. HDLL, b. ADLL, c. FDLL).
A boxplot representation of the ratio between the maximal and minimal DLLs measured during the gait cycle for the short and long lower limb.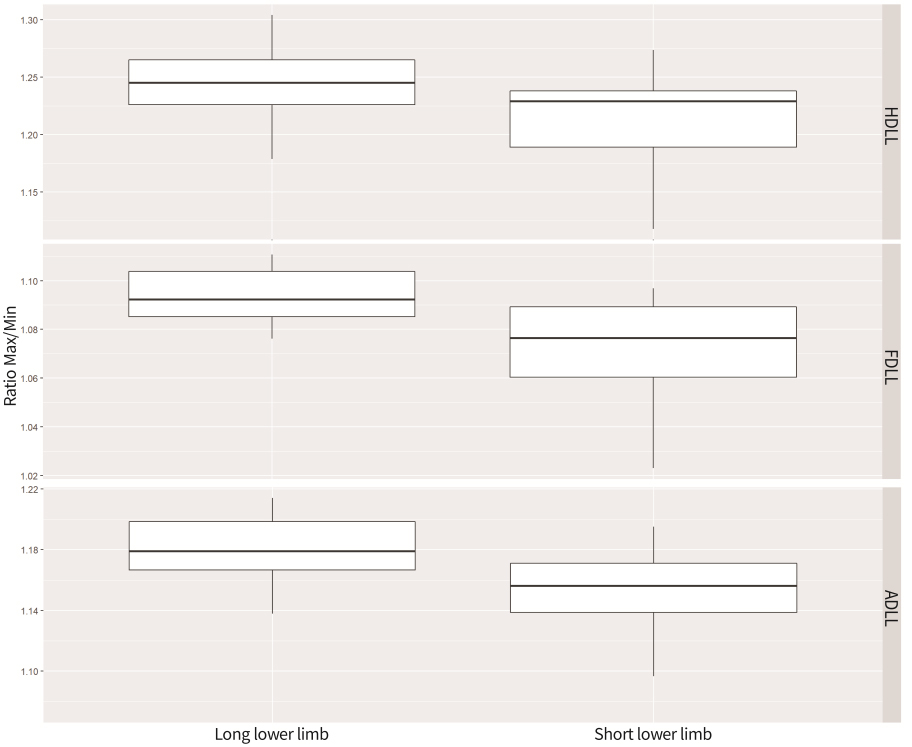
Correlation between the differences in ratios between the sides and LLD were significant (
Differences between maximal DLLs during the stance phase and contra lateral minimal DLLs during the swing phase categorized according to anatomic LLD.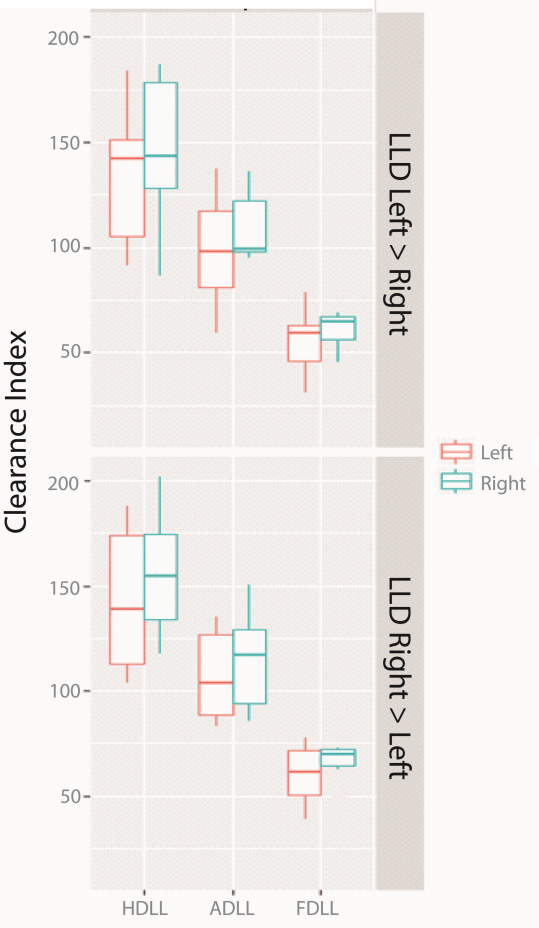
Difference between the right and left clearance indices categorized according to anatomic LLD.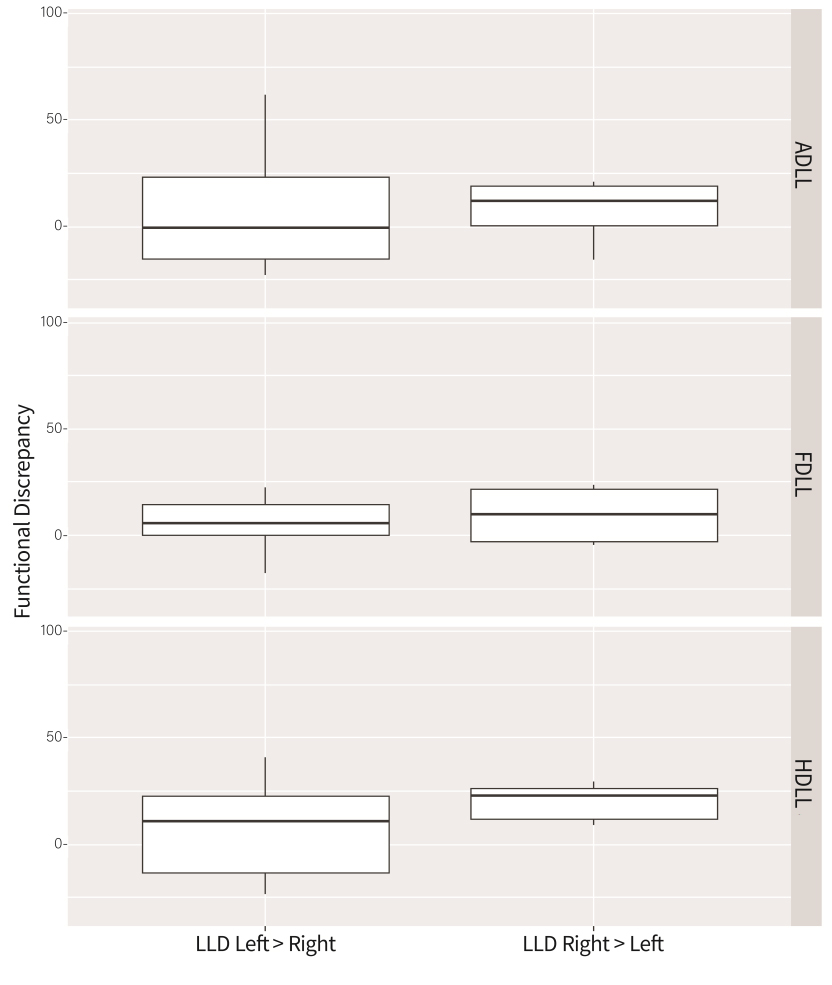
The functional discrepancy was in agreement with the anatomical LLD findings and was found to be higher when the right anatomical leg length was longer (Fig. 5), indicating that the functional discrepancy was in agreement with the anatomical LLD x-ray discrepancy findings (where the right lower limb was also found longer than the left). This difference was found in all three DLLs, HDLLs, ADLLs and FDLLs (Fig. 5).
We propose that the DLL measurement can identify anatomic LLD, which causes compensatory gait deviations, thus, altering functional leg length during the gait cycle. Anatomical LLD can be identified by asymmetric changes in the DLLs based on the difference between sides in the ratio between the maximal stance phase and the ipsilateral minimal swing phase DLLs and the clearance index, based on the difference between the maximal stance phase and the contra lateral minimal swing phase DLLs. DLL measurement appears to measure the anatomic LLD, hence we believe that the DLL measurement is a valid method which can be integrated into a gait analysis study, thus, assessing the presence of anatomic LLD.
Studies have found that LLD is compensated by opposite kinematic strategies to functionally lengthen the shorter limb and shorten the longer limb, mainly in the sagittal plane [13, 14, 16, 17]. The shorter limb is compensated by the increased plantar flexion and knee extension during stance as well as the decreased knee flexion during the swing phase. However, the longer limb is compensated by the increased flexion during the stance phase. During the swing phase, significantly greater knee and hip flexion have been observed on the longer side. These changes in kinematics have led to changes in the DLL [18] and can explain the symmetry in DLL found in our study, when comparing DLLs throughout the gait cycle.
In our study, a non-significant change was found in DLL throughout the gait cycle between the longer and contralateral shorter lower limb implying that mild anatomic LLD does not lead to significant asymmetric compensations in DLLs, when comparing DLLs at the same event in the gait cycle. Mild LLD can be compensated by the lower limbs, thus, achieving symmetrical DLLs by shortening the longer lower limb’s DLL and by elongating the shorter limb’s DLL. Anatomic LLD might manifest in asymmetrical DLL, if a higher discrepancy in LLD is present [18]. Khamis and Carmeli found that significant asymmetrical DLL, through most of the gait cycle, began in a simulated LLD condition using a 20 mm shoe lift, thus, leading to a change in all three DLLs in a 30 mm shoe lift. This might explain why participants with mild LLD, on an average of 12.66–17.4 mm, could still dynamically compensate and achieve symmetry. However, it should be noted that the effect of true LLD or simulated LLD on strategies used to equalize the limb lengths and DLL may slightly differ. Moreover, with respect to these findings, clinicians should be cognizant that patients presenting with mild LLD, even as small, on average of 12.66–17.4 mm, could compensate during gait and subsequently, explain the patients’ asymmetrical lower limb alignment or kinematics and their symptoms.
Khamis and Carmeli also found a significant difference between sides in the ratio between maximal stance and the minimum ipsilateral DLLs during the swing phase. The ratio increased on the longer side which might have been due to compensational shortening during the swing phase [18]. However, it decreased on the shorter side, which appears to be due to the increased dynamic length during the swing phase [18]. This is in agreement with others who found that the functionally shorter lower limb also presented with lower ratios than the longer lower limb [23].
The clearance indices quantify the dynamic discrepancy when a higher index value occurs during the longer limb swing phase due to excessive functional shortening of the longer limb during the swing phase and/or functional elongation of the shorter limb during the stance phase [18]. A lower index value occurs during the shorter limb swing phase due to excessive functional shortening of the longer limb during the stance phase and decreased functional shortening of the shorter limb during the swing phase [18].
According to these results, clinicians are encouraged to assess gait in a clinical setting, yet focus their evaluation specifically to the mid to terminal stance and mid swing phases, where gait deviation altering DLLs were found to occur. The awareness as to where during the gait cycle and which specific gait deviations to expect [16], renders it easier to conduct a gait evaluation in a clinical setting. If these specific gait deviations occur and appear in the appropriate phases of the gait cycle, clinicians should therefore, suspect the presence of anatomic or functional LLD.
Clinically, two methods are used to measure LLD: the direct method, which measures the distance between two anatomical points while lying in a supine position (using a tape measurement) and the indirect method, measuring LLD in a standing position, utilizing lifts to level the pelvis. There are still differences of opinion in the literature as to the reliability and validity of these methods [16]. Therefore, we cautiously suggest a different approach to detect the presence of LLD in clinical settings. Asymmetrical lower limb alignment that might be observed during standing, which is easier to observe than during gait, might indicate the presence of anatomic LLD, i.e., the presence of unilateral foot hyperpronation, excessive knee flexion, or upward pelvic obliquity, might denote the presence of a longer lower limb on the same side. On the other hand, opposite lower limb alignment might imply a shorter lower limb. However, this was not the scope of our study, and further research evaluating the presence of asymmetric lower limb alignment, anatomic LLD and DLL measurement is recommended.
The advantage of this method is its simplicity. It can be applied to any gait analysis study. DLL measurement can be added to the kinematic data output, thus, presenting the clinician with more data necessary for decision making. Thus, the authors recommend that if gait analysis studies are being performed to detect kinematic asymmetry compensating for LLD, adding DLL to measure the amount of LLD might assist in avoiding excessive exposure to x-ray radiation. Furthermore, DLL can also measure functional LLD when additional abnormal clinical findings are present [28].
In our study, the clearance indices were found to be higher on the right when the right lower limb was anatomically longer. On the other hand, the clearance indices were relatively symmetrical when the left lower limb was longer. This might be explained by the smaller anatomic discrepancy found amongst only 6 participants with a longer left lower limb, a difference of 12.66 mm (2.28–23.04) (average (95% CI)). In addition, the functional discrepancy measured as the difference between the clearance indices was found to be higher for the longer right lower limb, indicating that the functional discrepancy was capable of detecting the differences between right and left anatomic LLD, when the discrepancy between them was only on average 4.74 mm. These findings suggest that functional discrepancy is highly sensitive and can be indicative of the magnitude of the LLD.
Conclusions
DLL measurement is a method which can potentially be integrated into gait analysis studies. It is capable of detecting anatomic leg length differences based on functional changes in leg length and functional discrepancy, altered due to kinematic compensatory strategies. DLL measurement enables the clinician to further improve the detection of mild LLD, provide a more precise measurement, and thus a more reliable recommendation for intervention. Furthermore, this measurement can be used to evaluate the accuracy of a shoe or heel lift adjustment during walking. It is known that kinematic strategies are frequently employed to functionally lengthen the shorter limb and simultaneously shorten the longer limb DLL. However, these kinematics variations might be slight or non-significant at each joint; but, their total effect might lead to a significant effect on the DLL, thus detecting the presence of mild anatomical LLD. However, further studies with a larger number of participants and a higher range of LLD are recommended to validate this process.
Footnotes
Conflict of interest
The author has no conflict of interest to report.