
Abstract
OBJECTIVE:
This study was performed to illustrate the potential relationship between reduced serum and local LncRNA MALAT1 expressions with disease severity in patients with non-traumatic osteonecrosis of the femoral head (ONFH).
METHODS:
A total of 104 patients with non-traumatic ONFH and 100 healthy controls were consecutively recruited from our hospital. Serum and local LncRNA MALAT1 expressions were detected using real-time polymerase chain reaction (RT-PCR). Radiographic progression was defined by Ficat classification. Clinical severity was evaluated by Visual Analog Scale (VAS) and Harris Hip Score (HHS). Receiver operating characteristic (ROC) curve was carried out to determine the diagnostic value of MALAT1 in the radiographic progression.
RESULTS:
Serum LncRNA MALAT1 expressions were significantly lower in non-traumatic ONFH patients than in healthy controls. In addition, local MALAT1 expressions in non-traumatic ONFH tissue were significantly lower in the affected area than in the non-affected area. Ficat grade 4 has significantly lower serum and local LncRNA MALAT1 expressions in comparison with grade 3, and Ficat grade 3 showed markedly decreased serum and local LncRNA MALAT1 expressions compared with grade 2. Serum and local LncRNA MALAT1 expressions were significantly and negatively associated with VAS and positively related to the HHS. Further ROC curve analysis indicated that serum MALAT1 may act as a decent indicator in the diagnosis of non-traumatic ONFH.
CONCLUSIONS:
Decreased serum and local MALAT1 expressions may reflect disease severity in non-traumatic ONFH patients.
Introduction
Osteonecrosis of the femoral head (ONFH) is a bone-destructive disease which results from an imbalance of the coagulation and fibrinolysis system as well as insufficient blood supply [1]. ONFH usually causes progressive femoral head collapse and secondary arthritis necessitating total hip arthroplasty [2]. ONFH is a multifactorial and disabling disease that involves multiple genetic and environmental factors [3, 4]. The incidence of ONFH has increased over the past decade. It is estimated that 20,000 to 30,000 new patients are diagnosed with ONFH annually in the United States and 150,000 to 200,000 in China [5, 6].
ONFH can be divided into traumatic and non-traumatic conditions. As a subtype of ONFH, non-traumatic ONFH often occurs after the treatment of inflammatory diseases by steroid use [7]. It has been reported that the onset and development of non-traumatic ONFH is closely correlated with various factors including human immunodeficiency virus infection, autoimmune diseases, alcohol abuse, use of glucocorticoids and coagulopathies [8]. So far, the pathophysiological process of ONFH remains unclear. However, bone damage and insufficient blood supply are thought to be the two main final events in ONFH.
It has been reported that the development of non-traumatic ONFH is usually accompanied by changes in the expression of different types of non-coding RNA, such as microRNAs (miRNAs/miR) [9]. However, the involvement of long non-coding (lnc)RNAs, a subgroup of non-coding RNAs composed of
The long non-coding RNA (lncRNA) metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) [11], or Lnc-MALAT1, is an abundant and highly conserved lncRNA [12] and was first identified as a valuable indicator for lung cancer metastasis [13]. Lnc-MALAT1 is upregulated in various human cancers [14] and interacts with serine/arginine-rich proteins to regulate the subcellular localization of splicing regulatory proteins [15].
In recent years, lncMALAT1 has been proved to protect bone against damage and promote angiogenesis. On the one hand, previous studies demonstrated that MALAT1 was significantly down-regulated in the decreased osteogenic differentiation of BMSCs in steroid induced ONFH patients [16]. Moreover, lnc-MALAT1 could protect human osteoblasts from dexamethasone-induced injury through activation of Ppm1e-AMPK signaling [17].On the other hand, MALAT1 has been proved to promote angiogenesis in various conditions [18, 19]. For example, MALAT1 could promote angiogenesis in brain microvascular endothelial cells by upregulating VEGF-A and ANGPT2 [20]. It could furthermore promote angiogenesis of mesenchymal stem cells by inducing VEGF [21].
The previous studies listed above indicate that APN may play a pivotal role in protecting non-traumatic ONFH patients against bone damage. However, to our knowledge, no studies explored the association of serum or local MALAT1 expressions and disease severity in ONFH patients. Therefore, the scope of our study was to examine whether serum and local MALAT1 expressions may be potential protective biomarkers of nontraumatic ONFH.
Patients and methods
Study participants
From October 2018 to December 2019, a total of 104 patients with non-traumatic ONFH mainly caused by steroid and alcohol use were enrolled in our study. All patients received total hip arthroplasty or hip preserving surgery including core decompression, vascularized bone grafting, femoral varus osteotomy, and femoral rotational osteotomy. The diagnosis, classification, and staging of ONFH were based on the 2001 Japanese Orthopaedic Association (JOA) classification, which refers to findings on anteroposterior and lateral plain radiographs or magnetic resonance imaging scans [22]. Meanwhile, 100 individuals attending the regular health examination served as age- and sex-matched healthy controls. The healthy controls were enrolled based on a physical examination, with no steroid-induced ONFH or other related diseases. All subjects were Han people living in or near Linyi City in China.
The inclusion criteria were: ONFH was diagnosed based on X-ray, MRI and CT scanning; Steroid-induced ONFH patients were diagnosed on the basis of taking a mean daily dose of 16.6 mg or an equivalent maximum daily dose of 80 mg of prednisolone within one year; Alcohol-induced ONFH patients must have a history of alcohol intake
Sample preparation and quantitative real-time polymerase chain reaction (qRT-PCR)
Venous blood samples were collected from patients prior to surgery or other treatments. All serum samples were processed within 4 h after blood drawing. In short, whole blood was drawn into blood vessels without adding anticoagulants and was separated to obtain serum by centrifugation at 1,500 g for 15 min. For tissues, 104 pairs of affected tissues and adjacent non-affected tissues were obtained from patients. Total RNA was reverse-transcribed to cDNA using PrimeScript RT reagent kit with gDNA Eraser (TaKaRa, Japan) according to the manufacturer’s instructions. qRT-PCR was performed using FastStart Universal SYBR Green Master (ROX) (Roche, Basel, Germany) in an Applied Biosystems 7500 Fast Real-Time PCR System (Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s protocol. The data were normalized to the expression of glyceraldehyde-3-phosphate dehydrogenase (GAPDH), and the relative expression levels of each gene were analyzed using the 2
Radiographic assessment
Radiographic progression was evaluated using the Ficat and Arlet classification system [23], which comprises four grades. Grade 1: Normal or, at most, minor changes; Grade 2: Diffuse or localized osteoporosis, sclerosis, or cysts of the femoral head; Grade 3: Sequestrum, break in articular cartilage, normal or increased joint space; Grade 4: Decreased joint space, collapse of the femoral head, acetabular osteoarthrotic changes. Patients with grade
Clinical severity assessment
The clinical severity of ONFH patients was evaluated by the Visual Analog Scale (VAS) and Harris Hip Score (HHS). The VAS was 10 mm long with three anchors dividing three zones (green, yellow, and red). For each symptom, the green zone (0–30 mm) was labeled “mild symptoms”, the yellow zone (30–60 mm) “moderate symptoms” and the red zone (61–100 mm) “bad symptoms”. Patients were asked to mark any point on the zone according to their perception of the symptoms. The distance between the 0 mm mark and the placement of the “X” was measured to provide a numeric interpretation of their symptom perception [24]. The HHS questionnaire includes questions about pain, lameness, ability to walk and to get up from/sit down on a chair, range of motion and limb length discrepancy. The scores range from 0 to 100. In this study, scores of less than 70 (poor), 70–79 (average), 80–89 (good) and 90–100 (excellent) were found [25].
Statistical analyses
All statistical analyses were performed using GraphPad 6.0 software (GraphPad Software Inc., San Diego, CA, USA). Analysis was expressed as mean
Results
Demographic statistics
Table 1 describes the demographic data and etiology of the 104 enrolled ONFH patients and 100 healthy controls. The age of the patients (44 females and 60 males) was 51.7
Demographic data
Demographic data
All data are given as mean
Serum relative MALAT1 expressions in patients with non-traumatic ONFH were significantly lower than in the healthy control group (0.60
A. Relative MALAT1 expression between ONFH patients and healthy controls. B. Relative MALAT1 expression between affected and non-affected tissue in ONFH patients. C. Relative MALAT1 expression between steroid-induced ONFH and alcohol-induced ONFH. Data were expressed as mean 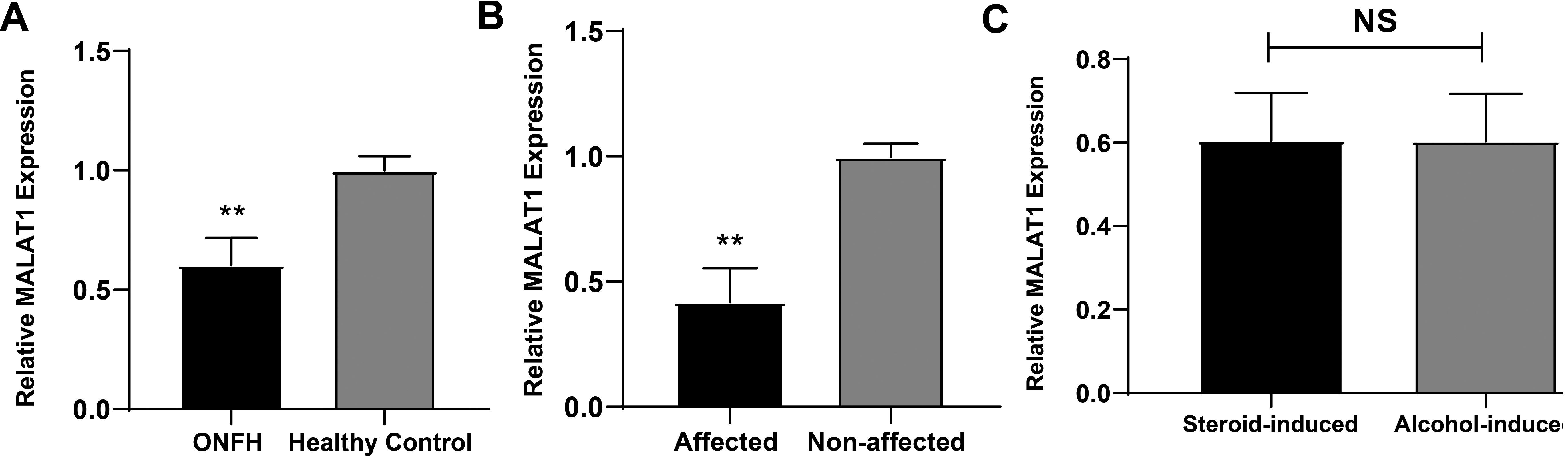
Plain X-ray of ONFH from Ficat grades 1–4.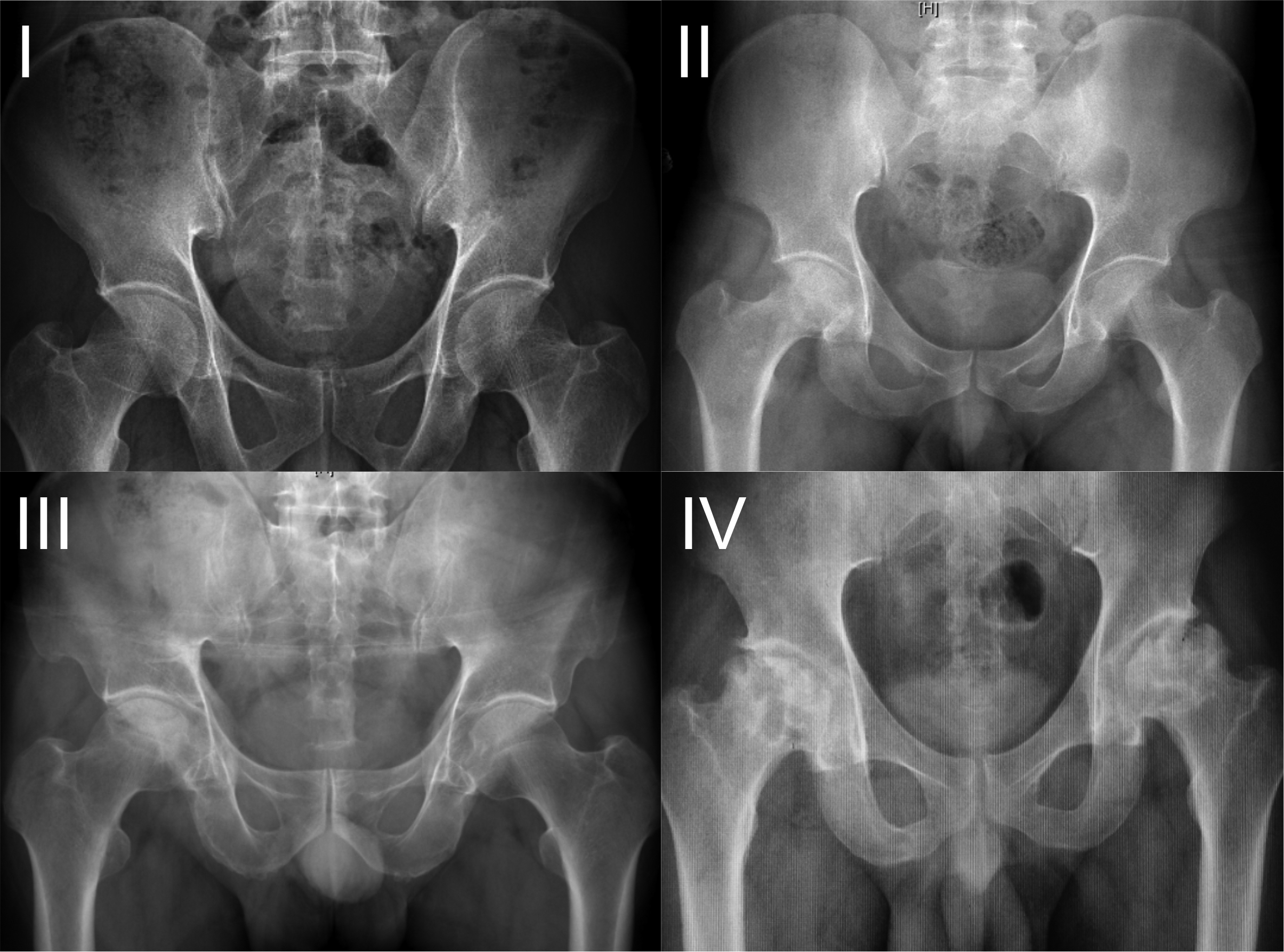
The serum and local MALAT1 expressions of 104 non-traumatic ONFH patients with different Ficat grades are depicted in Fig. 3. Accordingly, the ONFH patients were divided into three groups based on the Ficat grading system. The ONFH group included 33 patients with grade 2, 37 patients with grade 3, and 34 patients with grade 4. Representative figures of ONFH from Ficat 1–4 were demonstrated as Fig. 2. ONFH patients with Ficat grade 4 had significantly lower serum relative MALAT1 expressions than grade 3 (0.54
A. Comparison of serum MALAT1 expression among different Ficat grades. B. Comparison of local MALAT1 expression among different Ficat grades. C. Correlation of serum MALAT1 expression with Ficat grades. D. Correlation of local MALAT1 expression with Ficat grades.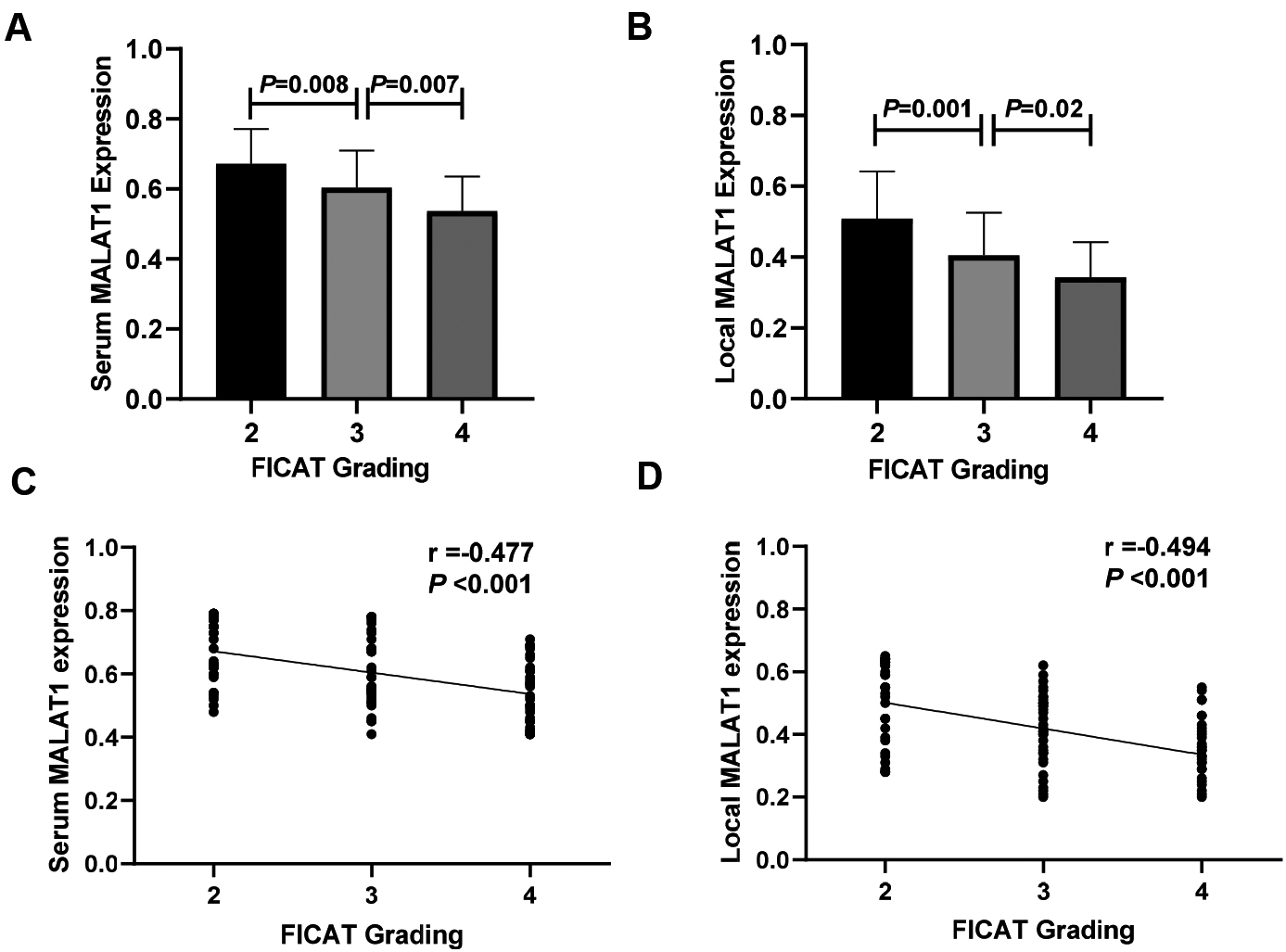
In contrast, ONFH patients with modified Ficat grade 4 had markedly lower local MALAT1 expression than in Ficat grade 3 (0.34
A ROC curve analysis was conducted to explore the diagnostic value of whether serum MALAT1 could be used as a diagnostic marker for radiographic progression of ONFH. As shown in Fig. 4, for Ficat grade 2 vs grade 3 and Ficat grade 3 vs grade 4, MALAT1 exhibited both significant AUCs (Ficat grade 2 vs grade 3: AUC
Area under curve of serum MALAT1 for evaluating radiographic progression by ROC curve analysis A. Ficat grade 2 vs grade 3. B. Ficat grade 3 vs grade 4.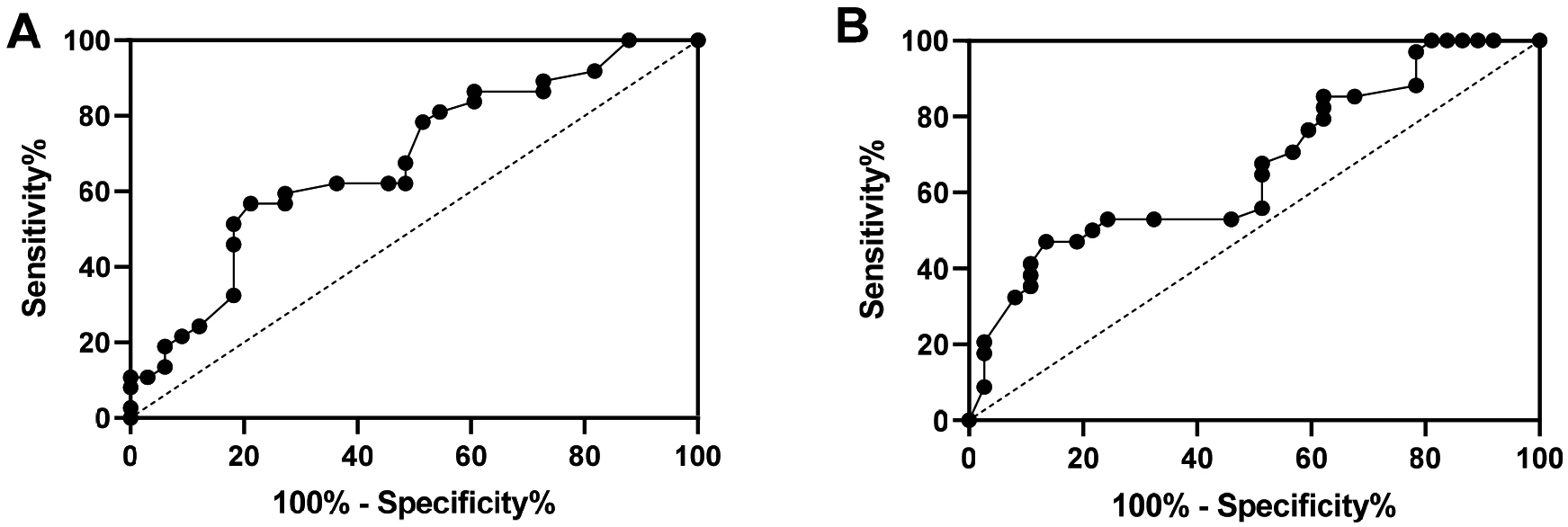
The correlation of serum and local MALAT1 expressions with clinical severity determined by VAS and HSS scores were examined. We found that both serum MALAT1 and local expressions were negatively associated with VAS scores (serum
A. Correlation of serum MALAT1 expression with VAS. B. Correlation of local MALAT1 expression with VAS. C. Correlation of serum MALAT1 expression with HSS. D. Correlation of local MALAT1 expression with HSS.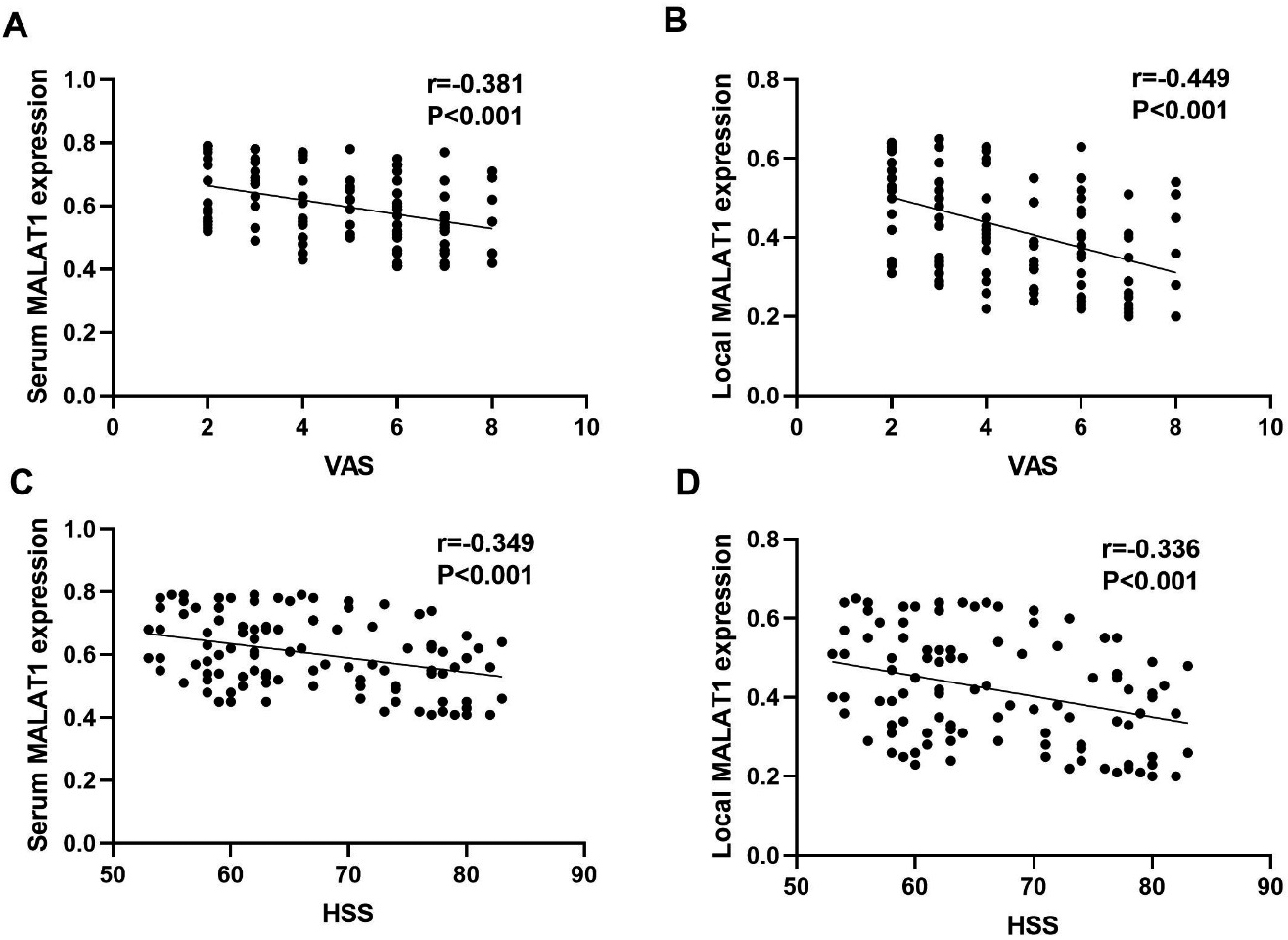
The present study explored the potential involvement of serum and local MALAT1 expression in patients with non-traumatic ONFH. To the our best of knowledge, this is the first investigation of serum and local MALAT1 expression involved in the progression of non-traumatic ONFH. We found that serum MALAT1 expression was significantly lower in non-traumatic ONFH patients than in sex- and age-matched healthy controls. In addition, local MALAT1 expression in ONFH tissue was significantly lower in the affected area than in the non-affected area. Moreover, serum and local MALAT1 expressions were negatively associated with radiographic progression and clinical severity. Further ROC curve analysis indicated that serum MALAT1 may act as a decent indicator in the diagnosis of non-traumatic ONFH.
Up to date, the normal diagnosis methods of non-traumatic ONFH consist of complaints of symptoms, worse function and radiographic alternations including X-ray, CT and MRI [26]. The complaints of non-traumatic ONFH include hip pain and restricted hip joint activity. However, non-traumatic ONFH at an early phase may develop with no manifestations of symptoms. Besides, radiographic progressions including decreased joint space, collapse of the femoral head and acetabular osteoarthritic changes are mostly indicators of late phase ONFH [27]. Therefore, brief and more effective methods that use valuable biomarkers may make a great difference for the diagnosis, treatment and prognosis of non-traumatic ONFH.
Epigenetics, an effective method for studying the interplay between environmental signals and the genome, has received a great deal of attention recently [28]. It has become apparent that non-coding RNAs play an important epigenetic role in non-traumatic ONFH including miRNA, lncRNA and circRNA. For example, HOTAIR acts as regulator on osteogenic differentiation and proliferation through modulating miR-17-5p and its target gene SMAD7 in non-traumatic ONFH [29]. MiR-181d can inhibit the differentiation of hBMSCs into osteoblasts by regulating the expression of SMAD3 [30]. hsa_circ_0000219 and hsa_circ_0005936 may regulate the progression of ONFH by mediating the proliferation and differentiation of BMSCs by sponging corresponding miRNAs [31]. However, none of these studies explored the relationship between their expressions with disease severity and progression in non-traumatic ONFH.
Circulating lncRNAs in serum or plasma have a good potential to serve as diagnostic or prognostic markers in various diseases, because they are stable, accessible and closely related to various diseases [32]. In our study, we comprehensively evaluated the serum MALAT1 levels in non-traumatic ONFH patients. We demonstrated that serum MALAT1 expressions were significantly lower in ONFH patients compared to healthy individuals. We also found that in non-traumatic ONFH patients, MALAT1 expression was more downregulated in the affected area than in the non-affected area. In addition, both serum and local MALAT1 expressions were negatively related to radiographic progression in ONFH patients.
Decreased bone formation and aberrant osteoclastic activity have been implicated in non-traumatic ONFH . A previous study showed dexamethasone-inhibited osteogenic differentiation of BMSC in a dose-dependent manner, leading to decreased MALAT1 [33]. Another study demonstrated that BMSCs-derived exosomal MALAT1 enhances osteoblast activity in osteoporotic mice by mediating the miR-34c/SATB2 axis [34]. Yi et al. found MALAT1 promoted Runx2-mediated osteogenic differentiation of adipose-derived mesenchymal stem cells by targeting miR-30 [35]. Bone repair involves bone resorption through osteoclastogenesis and the stimulation of neovascularization and osteogenesis by endothelial progenitor cells, suggesting that EPC-derived exosomes can promote bone repair by enhancing recruitment and differentiation of osteoclast precursors through LncRNA-MALAT1 [36].
Although some novel findings were revealed in the current study, there are still some limitations that should be taken into account when interpreting the results. First, our study did not include an intensive analysis of biological functions, which will be crucial for elucidating the role of MALAT1 in protecting non-traumatic ONFH. Second, this is a cross-sectional study with a relatively small sample size, which might influence the present findings. A larger case-control study is necessary to solve those problems, which could make our conclusions more powerful. Although we obtained evidence for the association between MALAT1 and ONFH disease progression, the pathogenesis of non-traumatic ONFH was still not completely understood. Further studies should be carried out to verify the results in other ethnicities.
Conclusion
In conclusion, this study is the first to report the aberrant expression of MALAT1 in relation to non-traumatic ONFH patients. We found that reduced serum and local LncRNA MALAT1 expressions are linked with disease severity in patients with non-traumatic ONFH. These findings offer a new insight into understanding the pathogenesis, facilitating early diagnosis and guiding the treatment of the disease.
Footnotes
Acknowledgments
This work was supported by the Natural Science Foundation of Heilongjiang Province of China (JJ2018ZZ0082) and the National Natural Science Foundation of China (31872980). The authors thank LetPub (www.letpub.com) for their linguistic assistance during the preparation of this manuscript.
Conflict of interest
None to report.