
Abstract
BACKGROUND:
Digital complete dentures (CDs) by computer-aided designing and computer-aided manufacturing (CAD-CAM) techniques (milling and three-dimensional (3-D) printing) have been evaluated clinically and provided satisfactory results. But clinical studies assessing occlusal forces by digital dentures are lacking.
OBJECTIVES:
To compare the occlusal force parameters in complete dentures (CDs) fabricated by milling, 3-D printing and conventional techniques having 3 commonly used occlusal schemes, using computerized occlusal force analysis system (Tech-Scan III- T-Scan III).
METHODS:
A total of 45 CDs were fabricated for 5 patients. Nine sets of CDs were made for each patient and were divided into 3 groups: Conventional CDs (CCD), Milled CDs (MCD), and 3-D printed CDs (3-DP CD). The CDs in each group were further divided into 3 sub-groups based on occlusion schemes – bilateral balanced (BBO), lingualized (LO) and mono plane (MP). Occlusal force analysis [percentage (%) of occlusal force applied on the right and left sides of the arch difference between them, centralization of forces and % of maximum occlusal/bite force] was done using computerized occlusal analysis system (T-Scan III) at the time of denture insertion. Univariate regression analysis and logistic regression analysis were performed (
RESULTS:
The intergroup comparison of force distribution on right and left side in CDs fabricated by various techniques showed insignificant differences (
CONCLUSIONS:
The occlusal parameters in CDs were affected by the fabrication techniques and occlusal schemes of CDs. The digital CDs retain adjusted occlusal schemes better and 3-DP CDs with BBO and LO occlusal schemes provided centralization of forces, better distribution and high maximum occlusal force % respectively.
Introduction
Computer-aided design/computer-assisted manufacture (CAD/CAM) has evolved as a game changer in almost every aspect of life. In dentistry, it was first introduced in 1970s by Duret and Preston [1]. Initially, its use was limited to fixed dental prosthesis but with expanding horizons of digital dentistry it is now frequently used in complete dentures (CDs) fabrication [2, 3]. Steps involved in fabrication of these digital CDs include: Acquisition of data (scanning), computer-aided design (CAD), and computer-assisted manufacture (CAM). The CAM part basically has two methods: Milling (Subtractive method) and three-dimensional printing (3-DP) (Additive method) [4, 5]. In the milling method, resin blocks are pre polymerized and minimal monomer is released, while in 3-DP method, polymerization of photosensitive liquid polymer layers (usually 5 to 20 per milli-meter of material in a layer) with ultraviolet light beam is done to produce definitive CD [6, 7]. These CDs have potential benefits over CDs fabricated by conventional methods: standardized fabrication techniques, high accuracy, high-value, quality-controlled materials, with superior mechanical properties, biocompatibility, smooth surface finish, fewer clinical appointments, similar or better fit of the tissue surfaces [2, 3, 4, 5, 6, 7, 8, 9, 10], overall improved cost-effectiveness [6] and enhanced patient satisfaction [6, 11].
In the present dental market, milling method is more popular than 3-DP, but soon this might reverse as subtractive method has inherent limitation of machining tools resulting in wastage of a large amount of denture base material [6, 7, 10]. In addition, 3-DP could be more economical as there is practically no loss of material and even unused material can be processed in the future, also multiple dentures can be printed at a time with fine detail reproduction [4, 5].
Various aspects of the digital and conventional CDs have been evaluated and reported in previous in vivo and in vitro studies viz. retention [9], trueness [4, 8], patient and dentist satisfaction [6, 11], ease of fabrication [4, 6], material properties and even mechanical behaviour [4, 10, 12] but occlusion was not much reviewed, which in no doubt should be highly precise for successful digital CDs. The presence of deflective occlusal contacts, poor occlusal force summation and unseen collection of unbalanced forces might result in torque and dislodgement of complete dentures affecting stability, comfort and patient acceptance [13, 14, 15].
Several occlusal scheme has been recommended for CDs mainly bilateral balanced occlusion (BBO), lingualized occlusion (LO) and neutral-centric or mono plane occlusion (MO). These schemes had been extensively assessed for conventional dentures for mastication, stability, esthetics, satisfaction etc. [16, 17, 18, 19, 20]. However, no clinical study has been performed till date for occlusal force analysis in digital dentures, which is essential as there is variation in the techniques of fabrication, use of modified varied materials and most of the time there are differences in the mode of teeth attachment to denture bases of digital dentures. Thus, this in vivo study was conducted to compare the occlusal force parameters (maximum bite force %, % of force on right and left side, difference between forces on right and left side and centralisation of forces) in CDs fabricated by milling, 3-DP and conventional techniques having 3 commonly used occlusal schemes (BBO, LO, MO), using computerized occlusal force analysis system (T-Scan III). The null hypothesis formulated was that there would be no difference in the occlusal forces parameters of CDs fabricated by either technique with any occlusal schemes inconsideration.
A computerized occlusal analysis system such as the T-Scan has enormous benefits over the articulating paper. It provides an intuitive graphic that identifies the position of contacts and the corresponding occlusal pressure intensity in percentage and shows distribution of the force bilaterally in the arch with the help of digital sensors. It also helps in recording the first contact, maximum intercuspation, applied maximum force moment, last contact, etc., against the time. This digital way of quantitative estimation of occlusal parameters makes T-Scan III a very effective tool in research and clinical practice [21, 22, 23, 24].
Materials and methods
The present cross-sectional study was conducted in the Department of Prosthodontics, College of Dentistry, King Khalid University, Abha, KSA and was approved by the institute’s ethical committee (IRB/KKUCOD/ETH/2019-20/069). To standardize the study protocol, a synchronized flowchart was prepared for fabrication of various complete dentures (Fig. 1).
Flowchart of the study design.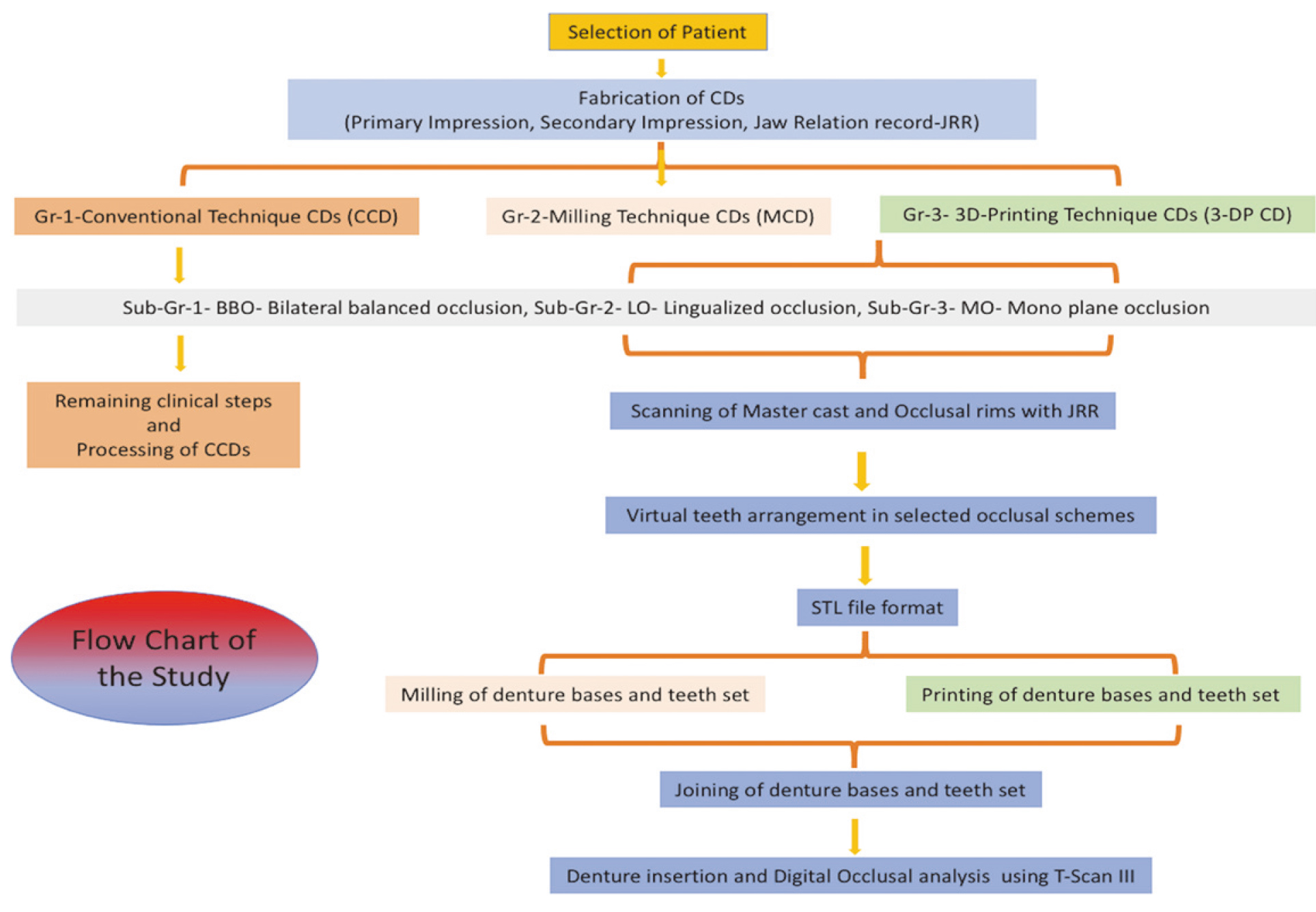
The participants were recruited from the outpatient department, reporting for the complete denture prosthetic treatment. All participants were explained about the study and written consent was obtained before inclusion in the study. Participants were screened by a single examiner with the following inclusion criteria: good neuromuscular control, high well rounded, completely healed maxillary and mandibular ridges with class I relation, in accordance with the American College of Prosthodontists type A classification of residual ridge morphology [25] and completely edentulous for at least 3 months. Exclusion criteria were uncontrolled systemic disease, mental problems, muscular dystrophy and temporomandibular disorders and any history of fractured jaw.
Total 45 CDs were fabricated in the study for 5 patients. For each patient, 9 sets of CDs were fabricated and were divided into 3 groups based on method of fabrication of CDs: Conventional techniques CDs (CCD), Milled/Subtractive CDs (MCD), and 3-D printed/Additive CDs (3-DP CD) techniques. Each Group CDs were further divided into 3 sub groups based on occlusion schemes-bilateral balanced occlusion (BBO), lingualized occlusion (LO) and mono plane occlusion (MO). During fabrication of CDs clinical steps were performed by chief researcher of the study and laboratory work was done by a single technician (blinded from the study) under the supervision of chief researcher. All researchers and involved technicians were trained and calibrated for conventional and digital CDs. The lottery system was used to decide which type of CDs with which type of occlusion had to be fabricated first for the patient
Conventional CDs (CCD) techniques
The conventional CDs were fabricated following the routine procedure. Since for each patient 3 CCDs had to made in 3 different occlusal schemes so, master casts of each patient were duplicated using duplicating material and secondary casts were poured with type IV die stone (GC Fujirock EP; GC Europe), to be used in further steps. Clinical steps involved were- primary impressions border molding with definitive impressions jaw relations using face bow (Hanau Spring-Bow; Whipmix, Louisville, KY, USA) and inter-occlusal bite record by polyether bite registration material (RAMITEC, 3M ESPE, St. Paul, MN, USA) teeth selection, wax trial placement, denture adjustment (expect occlusal surface adjustments) and insertion. Laboratory steps were-master cast and special tray fabrication, mounting on a semi-adjustable articulator (Whipmix 2000 Serise-2240, Louisville, KY, USA), teeth arrangement into predecided occlusal schemes (by single technician with the help of jig) and fabrication of CDs with conventional compression molding technique, lost wax technique and long polymerization cycle (9 hours in a water bath at 73
Milled CDs (MCD) and 3-D printed CDs (3-DP CD) techniques [2, 3, 4, 27, 28, 29] (Fig. 2).
Schematic illustration of digital denture fabrication. (a) Scanned images of maxillary master cast. (b) Scanned images of mandibular master cast. (c) Occlusal rims with jaw relation record. (d) Virtual teeth arrangement with the help of CAD software. (e) CAM fabrication of complete dentures by 3-D printing method. (f) CAM fabrication of complete dentures by milling method. (g) and (h) Representative completed denture.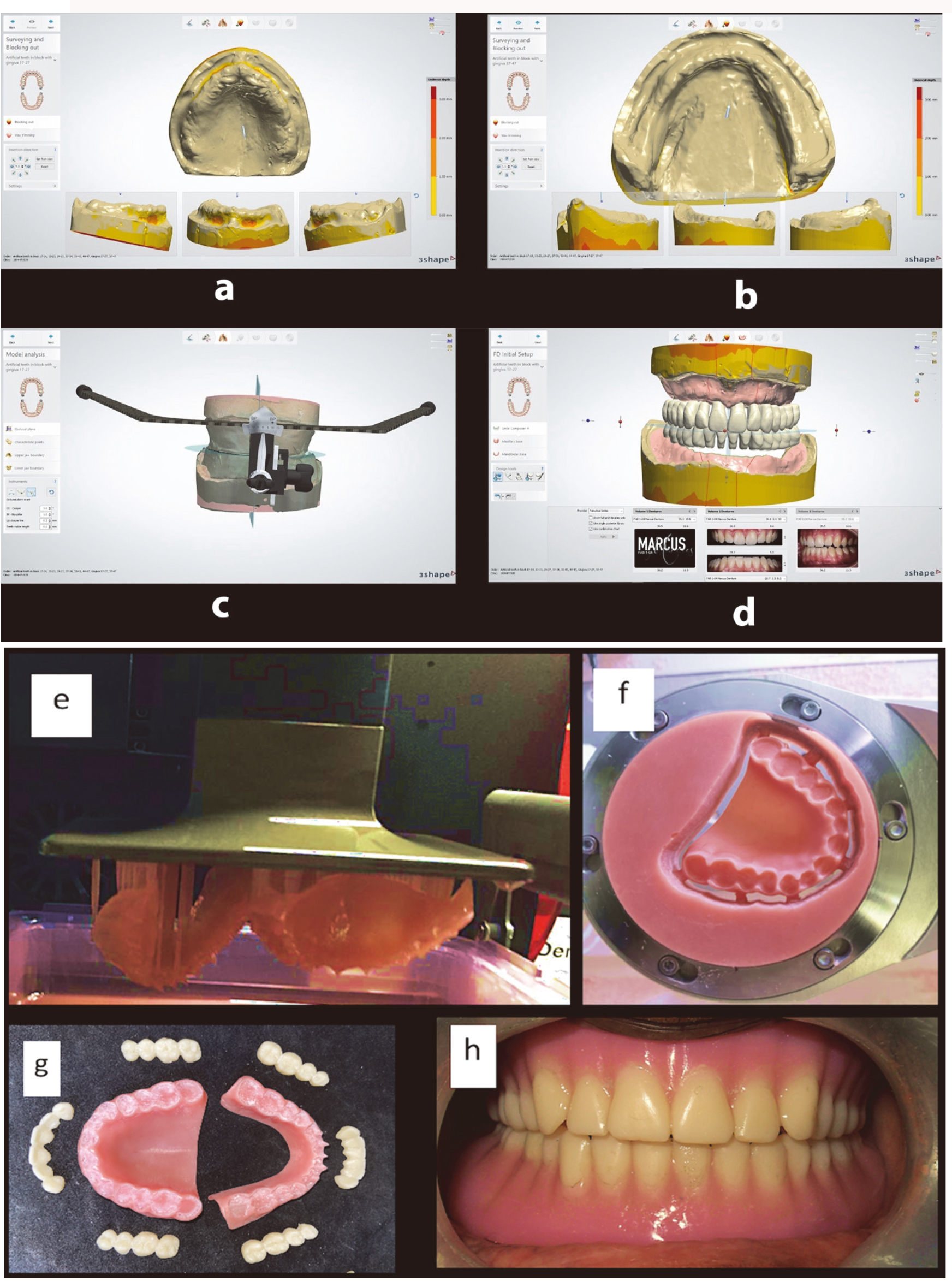
In the fabrication of digital CDs by milled or 3-D printing technique, the basic initial steps remained same i.e., acquisition of data (scanning) and computer-aided design (CAD). The difference was at manufacturing step. For data acquisition, the records obtained from the previously performed clinical steps for conventional techniques CDs (from primary impressions to jaw relation) were used and the secondary cast and occlusal rims with jaw relation record were scanned for digital dentures (if CCD was fabricated first, then same data was scanned before proceeding to next step of Conventional CD processing).
The procedure involved for scanning secondary casts, occlusal rims with jaw relation record was done by using desktop laboratory scanner (D800, 3Shape, Copenhagen, Denmark). This scanner had a high resolution and was calibrated to a precision of 8
For MCD group, the advanced CAM software (3-Shape Dental System – Complete Restorative – Complete denture module, Copenhagen, Denmark) was used to mill the samples. The denture bases were milled from highly cross-linked, industrially polymerized, monomer-free PMMA (Polymethyl-methacrylate) blank (Vipi Block Gum CAD/CAM Blank,
Similarly, for 3-DP CD group, same STL files of designed CDs were used, to print the samples. The CAM STL files of designed CDs were transferred to a software (PreForm, Formlabs Inc., USA) for print preparation and then send them to a 3-D printer (Form 2
After fabrication of digital CDs, the finishing and polishing was carried-out but laboratory/clinical remount procedures were not performed either for CCD or MCD, 3-DP CD groups. At the denture insertion appointment, stability and retention, over-extension, lack of frenal relief, any areas of soft tissue pressure or hard tissue problems related to dentures were solved. No occlusal corrections were done, and patients were informed about possible occlusal discrepancies. After that occlusal force analysis was done for each patient using computerized occlusal analysis system – T-Scan III (Tekscan Inc., South Boston, MA, USA). T-Scan III system was used to evaluate the pre-adjusted occlusal force imbalance. In the present study, the occlusal force parameters of CDs were assessed immediately after processing without laboratory/clinical remount and after finishing of study the occlusal adjustments were performed following basic protocols of remounting to satisfy the patients and make CDs comfortable.
The chief researcher and one of the co-researchers were trained for T-Scan III use and calibrated before the start of study for data collection. After denture insertion patients were asked to sit in upright position and digital registration of occlusal contacts was performed with 100
The T-Scan sensor was inserted between the occlusal surface of the denture teeth intraorally by resting the T-Scan sensor support within the facial central incisor embrasure of the maxillary denture’s central incisor teeth (Fig. 3). Then recording was activated and force levels were recorded starting with zero loads and ending with the maximum load. The patient was asked to firmly intercuspate into the sensor using their complete denture’s occlusion and hold their teeth together for 1–3 s once maximum intercuspation is reached. This procedure was repeated three times, considering the first two trials as accommodation attempts, only the last recording was used for statistical analysis. The T-Scan III provided the occlusal contact time-sequence from 1st tooth contact through to complete intercuspation and the percentage of occlusal force applied on the right and left sides of the arch producing a quantitative analysis of the distribution of occlusal contacts. Using this feature, the total amount of percentage of occlusal force of CDs of different groups were observed and centralization of forces were obtained by viewing the location of diamond icon inside or outside the eclipse.
Placement of T-Scan III handpiece in the patient mouth between the dentures for recording occlusal parameters.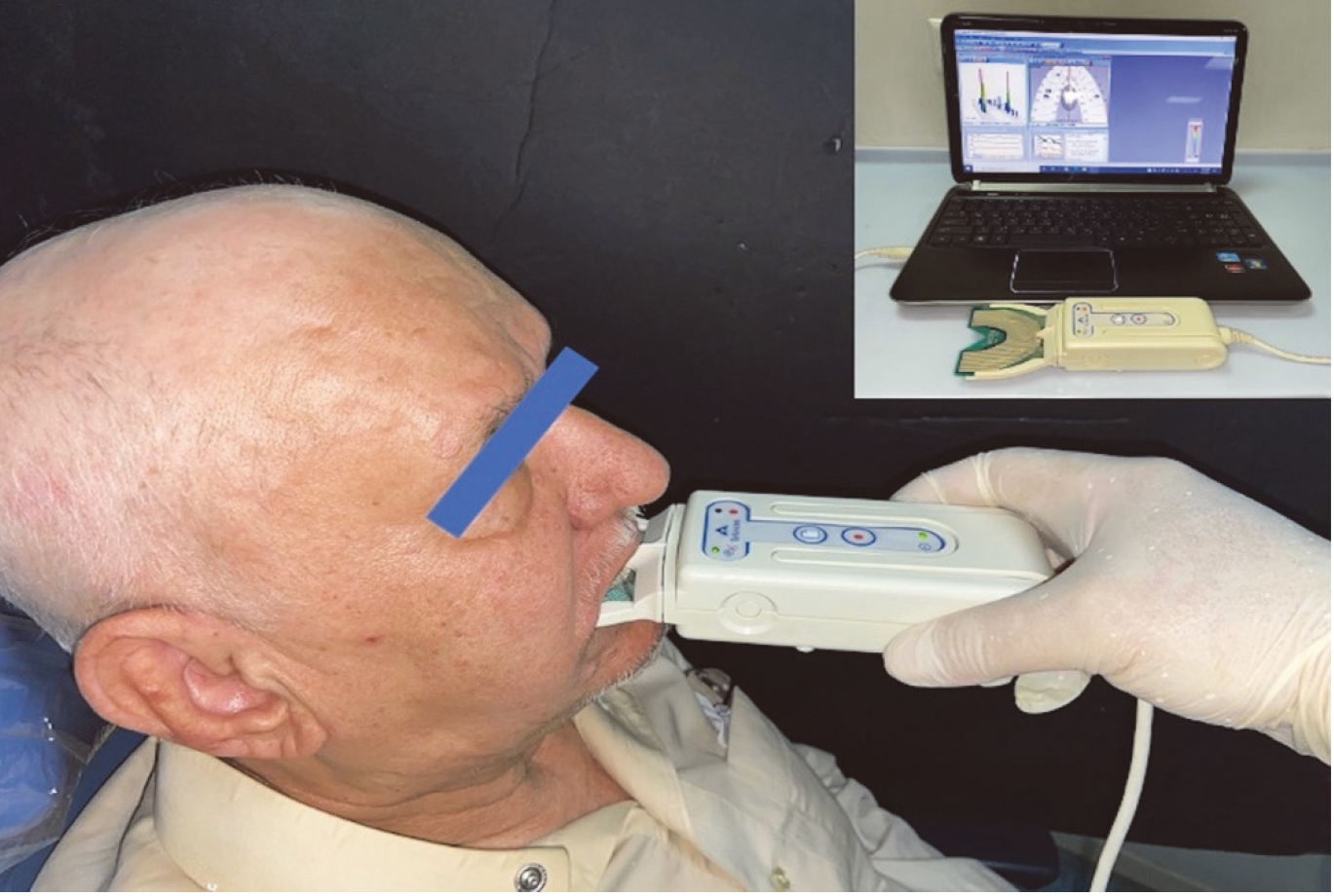
To verify the possible changes, the percentage of the right side of the arch was selected considering that a possible reduction in percentage would reflect an increase on the contralateral side, because they were complementary (the total of the sides results in 100%) (Fig. 4). The data so obtained was tabulated under headings of percentage of maximum bite fore, % of force on right and left side difference between them and position of diamond icon inside or outside the eclipse coded as 1 and 2 respectively and statistical analysis was done using statistical analysis software (IBM SPSS Statistics for Windows v22; IBM Corp, Armonk, NY, USA). The results were analysed using descriptive statistics (mean and SD) and intergroup comparisons were performed. Univariate regression analysis was used to find effects of technique of fabrication and occlusion scheme over the occlusal parameters. 95% confidence limits were applied to see the significantly higher or lower values of occlusal forces for various pairs of technique of fabrication and occlusion schemes. Logistic regression analysis was used to show the relationship of centre of force location with various techniques of fabrication and occlusion schemes. The p-value was taken significant when less than 0.05 (
The intergroup comparison of force distribution on right and left side in CDs fabricated by various techniques showed insignificant differences (
Intergroup comparison of right and left forces for various techniques of fabrication and occlusion schemes – (Univariate regression analysis)
Intergroup comparison of right and left forces for various techniques of fabrication and occlusion schemes – (Univariate regression analysis)
Representative image of T-Scan III desktop data of a complete denture sample illustrating; (a) percentage of forces on left and right side (66.1% left–33.9% right), 3-D column view; (b) 2-D contour view, housing center of force (COF) trajectory, summation diamond-shaped icon and COF ellipse, outside; (c) Zoom graph; (d) force versus time graph with black curving line showing percentage of maximum occlusal force (93.7%).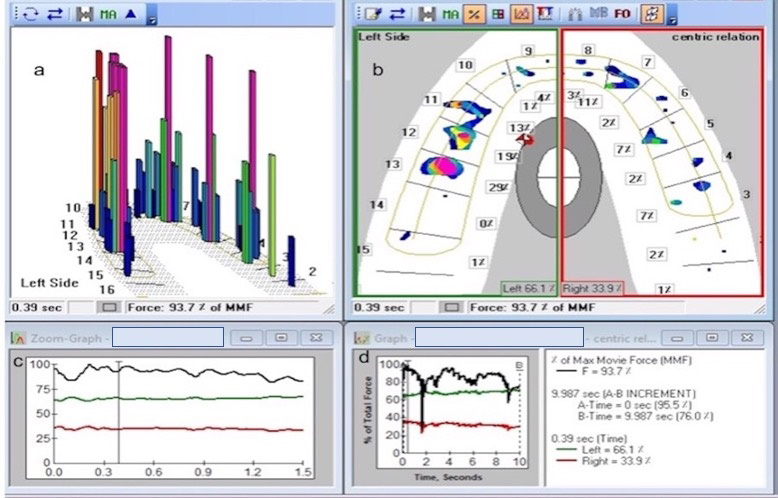
The intergroup comparison of right-left side force difference in CDs fabricated by various techniques (
The intergroup comparison of maximum bite force % showed highly significant differences according to technique of fabrication, occlusion schemes and their interaction effect (
Intergroup comparison of force differences (right-left) for various techniques of fabrication and occlusion schemes – statistics
(a) Intergroup comparison of right and left forces techniques of fabrication and occlusion schemes. (b) Intergroup comparison of force differences (right-left) for various techniques of fabrication and occlusion schemes.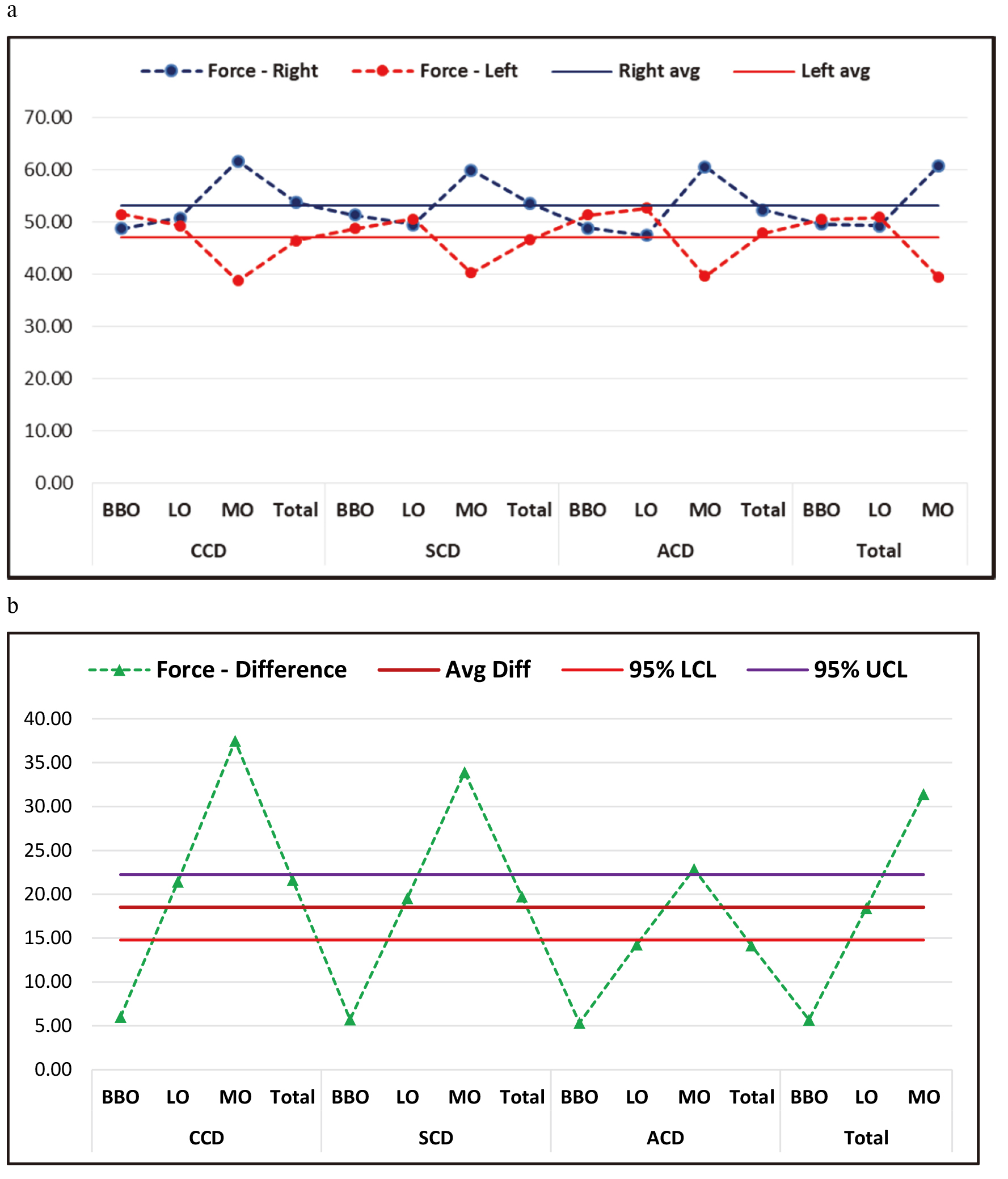
Intergroup comparison of maximum force for various techniques of fabrication and occlusion schemes – statistics
Continued, (c) Intergroup comparison of maximum force for various techniques of fabrication and occlusion schemes. (d) Intergroup comparison of center of force for various techniques of fabrication and occlusion schemes.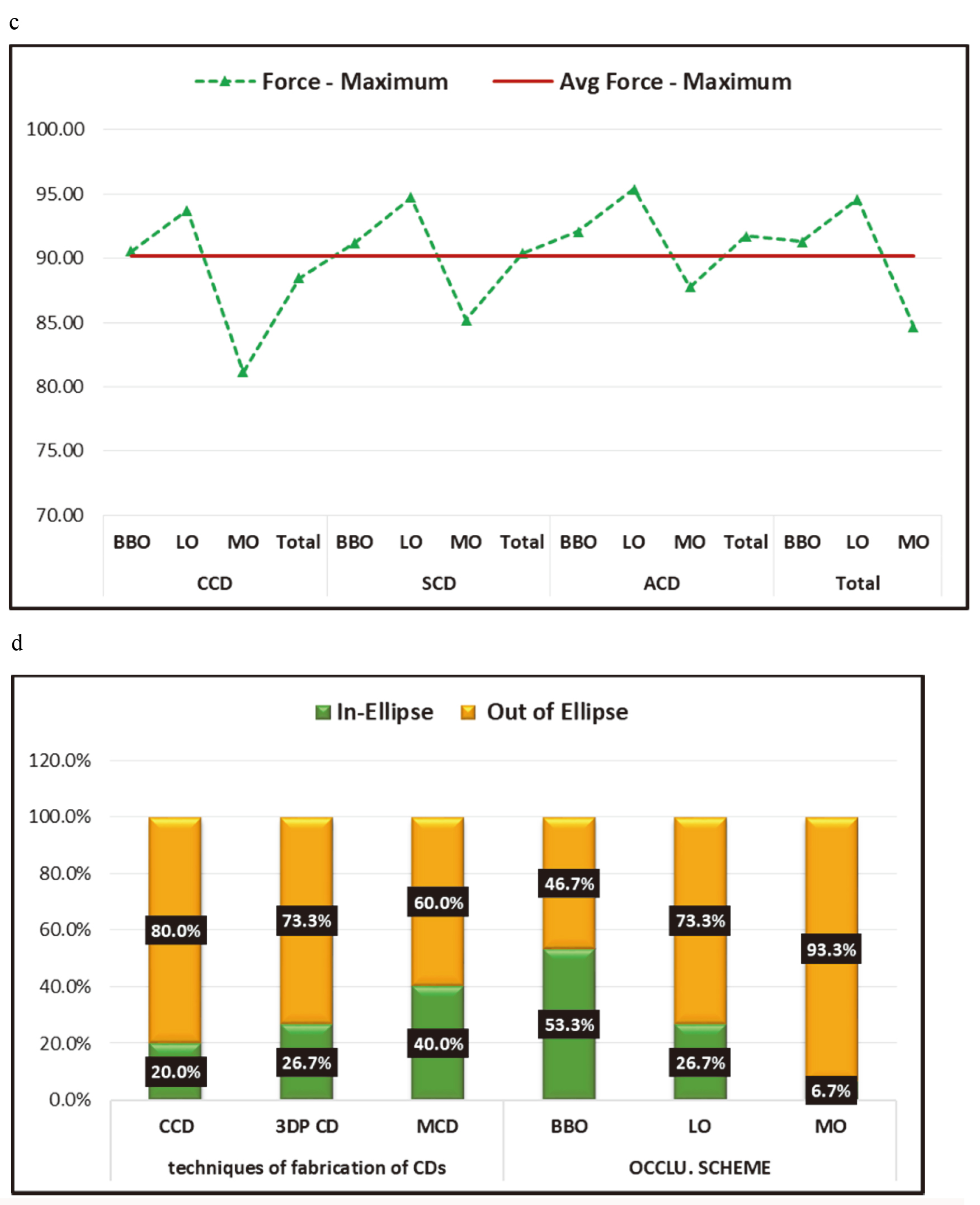
In comparison to 3-DP CD, the chances of centre of force out of ellipse was more in CCD (OR
Logistic regression analysis to show relationship of center of force condition with various techniques of fabrication and occlusion schemes
*B-Beta coefficient, SE- Standard error, OR- Odds ratio, CCD- Conventional Complete denture, MCD- Milled Complete denture, 3-DP CD- 3-Dimentional Printing Complete denture, BBO- Bilateral balanced occlusion, LO- Lingualized occlusion, MO- Mono plane occlusion.
In the present study, digital CDs were superior in each tested occlusal parameter compared to CCDs. Thus, the proposed null hypothesis was rejected. The outcomes of the study revealed statistically significant difference in mean maximum force %, in centralization of forces and also in difference between forces on right and left side of the arch between the dentures fabricated by various techniques having different occlusal schemes. This was in association with the different previous studies on CD occlusal trueness [14, 30, 31, 32, 33], reporting a discrepancy in digital CDs with a maximum value of 0.64 mm in Milled CDs, whereas in the conventional injection molding method the maximum value was 1 mm [32]. Tooth displacement is inevitable in conventional processing method of CDs fabrication as reported in many studies [14, 34, 35, 36]. An increase in occlusal vertical dimension up to 1 mm was considered acceptable in CDs as was reported in a study investigating the increase in the vertical dimension of occlusion (OVD) in CDs after processing with a conventional method [14, 37].
With the advancement in CAD-CAM technology , the frequency of use of digital CDs has increased, leading to the increase in number of studies evaluating various aspects of digital CDs retention [9], adaptation of digitally made denture bases (ranged between 0.058 mm [9, 14] and 0.29 mm [14] for digital methods and between 0.105 mm [9, 14] and 0.30 mm [14] for conventional technologies), trueness [8, 4], patient and dentist satisfaction [6], ease of fabrication [6], and material properties and even mechanical behaviour [4, 10, 12] but occlusion was not much reviewed. In the present study, occlusal force parameters of conventionally and digitally (by milling and 3-DP techniques) fabricated CDs with different BBO, LO, MO occlusal schemes, were evaluated using computerized occlusal force analysis system (T-Scan III). The T-Scan III system proved to be beneficial as it could accurately evaluate occlusal contact distribution (occlusal force %) in maximum intercuspation with sequence of occlusal time. The method was precise reliable and repeatable and had been used in previous studies. It provided a quantitative assessment of occlusal contacts pressure which would be impossible with the conventional methods of detecting occlusal discrepancies like articulating paper [21, 22, 23].
In the present study, we tested the centralisation of forces, % of force on right and left side, difference between forces on right and left side of the arch and total maximum force % generated in complete occlusion, this was evaluated immediately after processing so as to assess the effect of fabrication techniques of CDs and to avoided any manual intervention or subsequent procedural effect on CDs occlusion. The values of each tested parameters were better for digital CDs compared to CCDs and differences were statistically significant. The force distribution on right and left side of arch in CDs fabricated by various techniques showed insignificant differences (
On analysing, the tested occlusal schemes irrespective of CDs fabrication techniques, BBO and LO appeared to be better that MO. In, BBO the distribution of the occlusal forces on either side of the arch was better than LO and MO while the maximum force percentage of LO was more than BBO and MO, which was in complete association of several in vitro and in vivo studies on occlusion of CDs [13, 16, 17, 18, 19, 20, 21, 22]. Results showed that 3-DP CDs with BBO had better centralization and bilateral distribution of forces followed by MCDs with BBO, 3-DP CDs with LO MCDs with LO, CCD with BBO and CCD with LO schemes. While maximum bite force % of 3-DP CD was highest overall, followed by MCDs and CCDs and specifically with LO schemes. This difference may be attributed to the basic difference in the technique of milling and 3-D printing.
In the milling technique, the CDs were fabricated at a milling station using a pre-polymerized PMMA blanks manufactured under high pressure, consequently no shrinkage during polymerization unlike in processing of CDs in conventional technique. Highly defined computerized controlled milling of recesses in the denture bases and corresponding tooth would had resulted in accurate fitting and bonding of teeth with base thus, maintaining the occlusal scheme in a precise way [4, 5, 6, 7, 8, 9, 10, 11, 12, 14].
While 3-D printing technique fabrication of CDs takes place from a photosensitive liquid resin, repetitively layered on a support structure and polymerized by an ultraviolet or a visible light source [3, 4, 5, 14, 27, 28, 31]. Later teeth and bases were bonded with each other in a precise manner. Thus, occlusion in both of these techniques was not subject to polymerization shrinkage either, thus it might had retained adjusted occlusal scheme in a better way than CCD.
The conventional technique of CDs fabrication has inherent drawbacks of the technique itself like shrinkage during polymerization, release of stresses incorporated in the modelling waxes during manipulation, high content of residual monomer, high pressure of packing and uncontrolled expansion of dental plaster resulting in movement of the teeth [34, 35, 36, 37]. These procedural errors alter the established occlusal scheme and the same was clearly evident by the results of the present study.
In our clinical study, 3-DP CD group had better occlusal parameter values than MCD group which was in contrast to an in vitro study by Kalberer et al. [4] that demonstrated the trueness of the CAD-CAM milled complete dentures was statistically better than that of the rapidly prototyped complete dentures. These differences in occlusal parameter values might be attributed to the milling of teeth and denture base separately for MCD group and later bonding together. Recently introduced single bi-coloured dual disk (Ivoclar Vivadent) for milling might be helpful in reducing these differences. It was also reported that during the 3-D printing, polymerization shrinkage is practically negligible, and no trimming of the teeth and denture bases was done, compared to MCDs and CCDs as verified in the results [3, 4, 5, 14, 27, 28, 31].
Although the same CAD files were used in both milling and printing techniques, they differ in method of fabrication. At present the use of printing method is commonly used for try-in CDs and milling technique is preferred for production of definitive CDs, but soon the printing CDs would be used as an alternative to MCD owing to its obvious benefit viz. economical, better accuracy, biocompatibility, mechanical properties and patient satisfaction and overall low material wastage over milled techniques, however, further studies are needed to quantify these findings clinically and objectively with regard to CDs.
Overall, the study upheld the importance of one of the most basic steps of CDs, the laboratory and clinical remounting. In the present study also, patients were not satisfied even with digital CDs due to minute occlusal discrepancies, so clinical remount was done in CD of patient choice and later delivered to the patients, who showed complete satisfaction in follow up visits. This is even proved by the fact that most of the authors recommend the laboratory/clinical remount for CDs to remove the processing errors [4, 41].
Limitations
The computerized occlusion analysis system T-Scan III provided only relative value of the occlusal force, the absolute values were not possible. The occlusal parameters were tested immediately after processing, so effect of oral adaptation of CDs fabricated with different techniques were not assessed. The patients were asked to apply the maximum occlusal force instead of regular masticatory forces with CDs, so it is recommended to evaluate the CDs with regular masticatory forces. Also, effect of different machines and different available software were not assessed in this study. Finally, future studies are recommended with bi-coloured dual disk (for milled CDs) randomized clinical trials with a larger sample size and longer observation period to further assess the effect of fabrication techniques on occlusion of CDs.
Conclusions
Based on the findings of this clinical study, the following conclusions were drawn: the occlusal parameters were affected by the fabrication techniques and occlusal schemes of CDs. The digital CDs retain adjusted occlusal schemes better the conventionally fabricated CDs. 3-DP CDs with BBO and LO occlusal schemes provided centralization of forces, better distribution with total high maximum occlusal force percentage.
Footnotes
Acknowledgments
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for funding this work through General Research Project under grant number (G.R.P.-125-41). The authors are very grateful to Dentaly Dental Clinic and Research Center, Advanced Dental Lab and Mr. Mahmoud Rashed, Laboratory Chief Technician, Abha, KSA for CAD/CAM support.
Conflict of interest
None to report.