
Abstract
BACKGROUND:
The early diagnosis of thyroid cancer depends on the popularisation and development of diagnostic imaging techniques and the continuous improvement of physician diagnosis.
OBJECTIVE:
To investigate the clinical value of multi-parameter magnetic resonance imaging (MRI) and colour B-ultrasound elastography in thyroid nodules.
METHODS:
The clinical and imaging data of 252 patients with thyroid nodules who were admitted to our hospital were collected. All patients underwent preoperative colour B-ultrasound elastography and MRI. The postoperative pathological results were the gold standard for diagnosing benign and malignant thyroid nodules. The accuracy, sensitivity and specificity of MRI, colour B-ultrasound elastography and their combination for diagnosing benign and malignant thyroid nodules were compared.
RESULTS:
This study included 252 patients with 388 nodules. There were 169 patients with solitary nodules and 83 patients with multiple nodules. The maximum diameter of the thyroid nodules was 0.32–1.00 (0.75
CONCLUSION:
Combined ultrasound and MRI have high diagnostic accuracy and specificity for benign and malignant thyroid nodules. This diagnostic method can be applied in clinical practice.
Keywords
Introduction
Since the 1970s, the incidence of thyroid cancer has been steadily increasing, most significantly in middle-aged women [1]. According to relevant statistics, in Canada, the United States and other countries, the most common cancer in women aged 20 to 34 is thyroid cancer [2]. The early diagnosis of local recurrence or distant metastasis of thyroid malignancies is an essential factor affecting the prognosis of the disease.
The early diagnosis of thyroid cancer depends on the popularisation and development of diagnostic imaging techniques and the continuous improvement of physician diagnosis. Routine colour Doppler ultrasound and magnetic resonance imaging (MRI) are convenient, intuitive and primary methods for examining thyroid diseases. The diagnostic criteria of benign and malignant thyroid nodules based on the size, shape, capsule, boundary, aspect ratio, posterior acoustic halo, internal echo, calcification type, presence or absence of posterior acoustic attenuation and peripheral lymph node metastasis of thyroid nodules are based on routine Doppler ultrasound. However, many factors limit its diagnostic accuracy for benign and malignant lesions [3].
Colour B-ultrasound elastography is an ultrasonic method that reflects the hardness characteristics of lesions by detecting the hardness of different tissues. It provides a new concept for the clinical identification of benign and malignant thyroid nodules [4, 5]. The former can give the blood perfusion characteristics of the nodule and even small vessels, while the latter can reflect the tissue hardness and other information in the nodule. Magnetic resonance imaging has the attributes of multi-parameter imaging and high soft-tissue resolution and can display lesions from multiple levels and directions, enabling a complete understanding of those lesions. Moreover, it is non-invasive and has no radiation risk [6]. Some studies suggest that diffusion-weighted imaging (DWI) can effectively differentiate benign from malignant thyroid nodules with a short diameter of
However, there are few studies on the use of MRI, colour B-ultrasound elastography and a combination of the two methods for diagnosing thyroid nodules. In this study, the clinical and imaging data of patients with thyroid nodules in our hospital were analysed retrospectively. All patients underwent preoperative ultrasonography and MRI. The postoperative pathological results were the gold standard for diagnosing benign and malignant thyroid nodules. The accuracy, sensitivity and specificity of MRI, colour B-ultrasound elastography and their combination in diagnosing benign and malignant thyroid nodules were compared, and the clinical value of these three methods for diagnosing thyroid nodules was examined.
Materials and methods
Study subjects
The clinical and imaging data of patients with thyroid nodules who were admitted to our hospital from December 2018 to December 2021 were collected. All patients underwent preoperative B-ultrasound elastography and multi-parameter MRI. A total of 252 patients (388 nodules) were included in this study, including 119 females and 33 males aged 30–87 years, with an average age of 57.1
The inclusion criteria were as follows: (1) patients who underwent thyroid surgery and whose postoperative pathological results were available, (2) patients who had thyroid multi-parameter MRI and colour B-ultrasound elastography performed within one week before surgery and (3) the maximum diameter of the thyroid nodule was
The exclusion criteria were as follows: (1) patients whose image quality was poor, (2) diffuse nodules that could not be evaluated, (3) patients where the pathology report showed other pathological types, such as lymphoma and metastases and (4) patients with a history of thyroid surgery or neck chemoradiotherapy.
Methods
Colour B-ultrasound elastography
The patients were examined using a Supersonic Aixplorer colour B-ultrasound elastography diagnostic instrument and a linear array probe with a frequency of 6.0–12.5 MHz. The patient was placed in a supine position to expose the neck fully. After the lesions were visualised by the diagnostic instrument, the ultrasound elastography mode was activated, and the size of the region of interest (ROI) was adjusted to more than twice the size of the lesion. The patients were asked to hold their breath after the probe was pressed down slightly when the green diagnostic display bar stability 3–4 s after the image storage. After selecting a satisfactory image, the relatively hard area of the nodules was selected, and the ROI size was adjusted again. The application’s configuration software calculated the lesion tissue’s signal-to-noise ratio. Different-coloured codes represent different elastic tissues in the elastic diagram. Red denotes that the hardness of the tissue was lower than the average value, green indicates the average hardness, and blue denotes that the hardness of the tissue is higher than the average value. The thyroid nodule was thus graded according to the elastic grading method.
The criteria for ultrasound elastography were as follows [7]: The sonoelastography score comprised a total of 5 points: 1 point was given when all or most of the lesion was green, 2 points were given when the centre of the lesion was blue and the surrounding area was green, 3 points were given when the proportion of green and blue in the lesion was equal, 4 points were given when the lesion was blue overall or there was a small amount of green inside the lesion, and 5 points were given when the lesion was blue overall and the surrounding tissue was also blue. A score of
Multi-parameter MRI
Neck MRI scans were performed using a SIMENS MAGNETOM LUMINA 3.0TMR MR scanner with an eight-channel thyroid-dedicated surface coil (Medcoil TL80, Suzhou Zhongzhi Medical Technology Co., Ltd., China). All patients were supine, with the body lying naturally and the head advanced. During examination with the head- and neck-phased array coils, the patients were instructed to breathe calmly and avoid swallowing, coughing, shaking and other movements.
Conventional cross-sectional scans were performed under the following conditions: the turbo spin echo-T1 weighted image (T1WI-TSE) fat suppression repetition time (TR) was 716 ms, and the echo time (TE) was 12 ms. The TSE’s T2WI-TSE showed fat suppression with a TR of 3,000 ms, a TE of 88 ms, a slice thickness of 4 mm, a field of view of 240 Coronal scans were performed under the following conditions: a T2WI-TSE fat suppression TR of 3,000 ms, a TE of 89 ms, a slice thickness of 3 mm, a visual field of 220 Diffusion-weighted imaging was performed under the following conditions: a single-shot echo technique was used, with a b value of 300 s/mm
The diagnostic criteria for malignant nodules were as follows: a moderate or low iso-intensity on T1-weighted imaging and high signal intensity at the lesion site on T2-weighted imaging, blurred borders and an irregular shape [8].
Multi-parameter MRI and colour B-mode ultrasound elastography were combined to formulate diagnoses. When one or both modalities indicated a positive diagnosis of malignancy, it was considered positive; otherwise, it was negative. The examination equipment and method in the combination group were identical to the simple colour B-ultrasound elastography group and the simple multi-parameter MRI group. The ultrasound and MRI images of the three groups of patients were analysed by two ultrasound diagnostic physicians and two MR diagnostic physicians, and the clinical characteristics of the acquired image images were analysed to clarify the nature of the lesions. If there was disagreement on a diagnosis between two physicians, a consensus was reached by discussion.
Data collection and analysis
Basic information, such as the gender and age of the subjects, was collected. The results of the multi-parameter MRI and the colour B-mode ultrasound elastography and postoperative pathology reports were also recorded. The postoperative pathological results of the nodules were considered the gold standard. The results of the postoperative pathological examination were compared with those of colour B-ultrasound elastography, multi-parameter MRI and a combination of the two. The diagnostic accuracy, sensitivity and specificity of the three detection methods were evaluated. The sensitivity and specificity were calculated as follows: sensitivity
Statistical methods
All data were analysed using SPSS for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). Enumeration data were expressed as a percentage (%) and analysed using a Chi-squared test. Measurement data following a normal distribution were expressed as mean
Results
General characteristics of study subjects
This study included 252 patients (388 nodules), including 119 females and 33 males aged 30–87 years, with a mean age of 57.1
Consistency analysis between the three diagnostic methods and the pathological results
Of the 334 malignant thyroid nodules diagnosed by multi-parameter MRI, 318 were pathologically confirmed as malignant, and 16 were benign. Of the 54 nodules diagnosed as benign by multiparametric MRI, 24 were pathologically confirmed as malignant, and 30 were benign. Of the 318 malignant thyroid nodules diagnosed by colour B-ultrasound elastography, 302 were pathologically confirmed as malignant, and 16 were benign. Of the 70 benign thyroid nodules diagnosed by colour B-ultrasound elastography, 40 were pathologically confirmed as malignant, and 30 were benign. Of the 342 thyroid nodules, 336 were pathologically confirmed as malignant, and 6 were benign. Among the 46 benign thyroid nodules, 6 were pathologically confirmed as malignant, and 40 were benign. The consistency of the three diagnostic methods with the postoperative pathological diagnosis and the kappa values of multi-parameter MRI, colour B-ultrasound elastography and combined diagnosis was 0.541, 0.437 and 0.852, respectively. The consistency of the combined diagnosis was significantly higher than the two detection methods individually. The difference between the three methods and the pathological results was statistically significant (
Consistency of three diagnostic methods with postoperative pathological diagnosis
Consistency of three diagnostic methods with postoperative pathological diagnosis
Note:
Pathological staining of thyroid nodules. A is papillary thyroid carcinoma (HE staining, 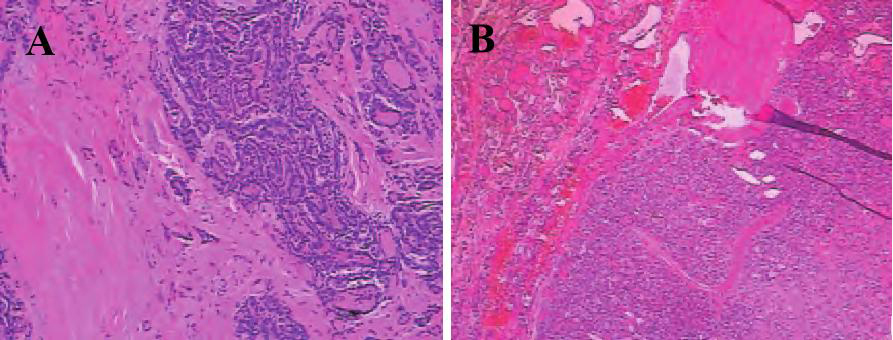
The accuracy of MRI diagnosis was 89.69%, the sensitivity was 92.98%, and the specificity was 65.22%. The diagnostic accuracy of colour B-ultrasound elastography was 85.57%, the sensitivity was 88.30%, and the specificity was 65.22%. The combined diagnostic accuracy was 96.91%, the sensitivity was 98.25%, and the specificity was 86.96%, which was higher than MRI and colour B-ultrasound elastography alone. The false negative rates of multi-parameter MRI, colour B-mode ultrasound elastography and combined diagnosis were 7.02%, 11.70% and 1.75%, respectively. The Youden indices were 58.20%, 53.52% and 85.21%, respectively, as shown in Table 2.
Test power of three diagnostic methods
Test power of three diagnostic methods
Typical ultrasound real-time tissue elastography of thyroid nodules. A is a thyroid nodule, characterized by irregular shape, with calcification, and posterior attenuation; B is papillary carcinoma, characterized by thyroid nodules with calcification, with blood flow signals.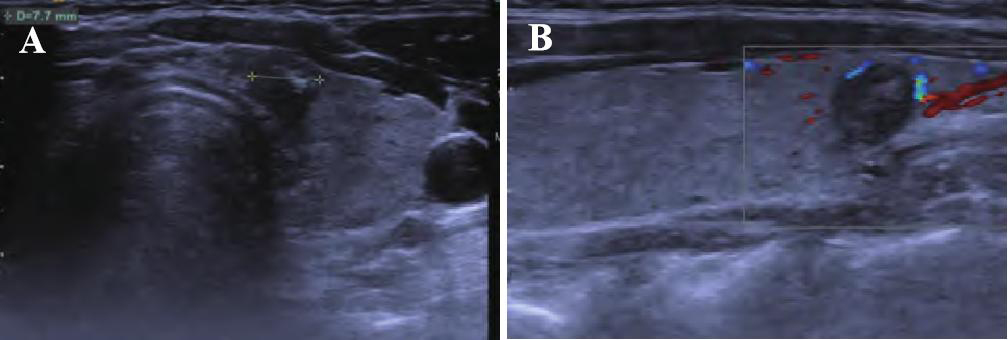
Typical magnetic resonance weighted imaging of thyroid nodules. A is T1WI showing papillary carcinoma, characterized by isointense signal in the middle, uneven; B is papillary carcinoma on T2WI, characterized by slightly higher signal with punctate slightly lower signal.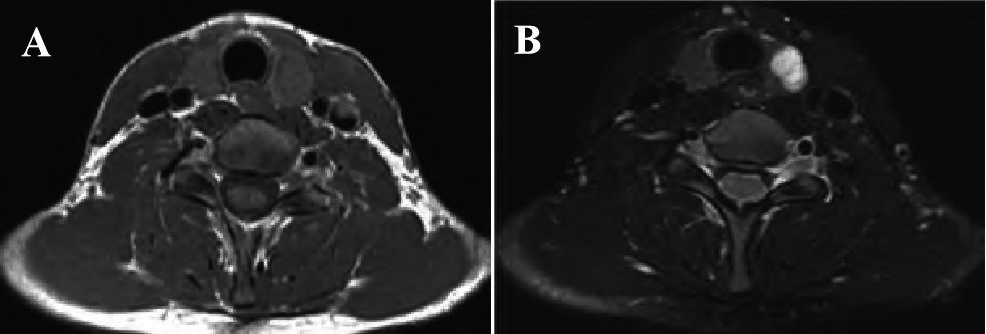
The AUC of MRI, colour B-ultrasound elastography and combined diagnosis were 0.768, 0.791 and 0.926, respectively. The AUC of the three diagnostic methods was
Comparison of AUC in three diagnostic methods
Comparison of AUC in three diagnostic methods
ROC curves of three diagnostic methods for the diagnosis of benign and malignant small thyroid nodules.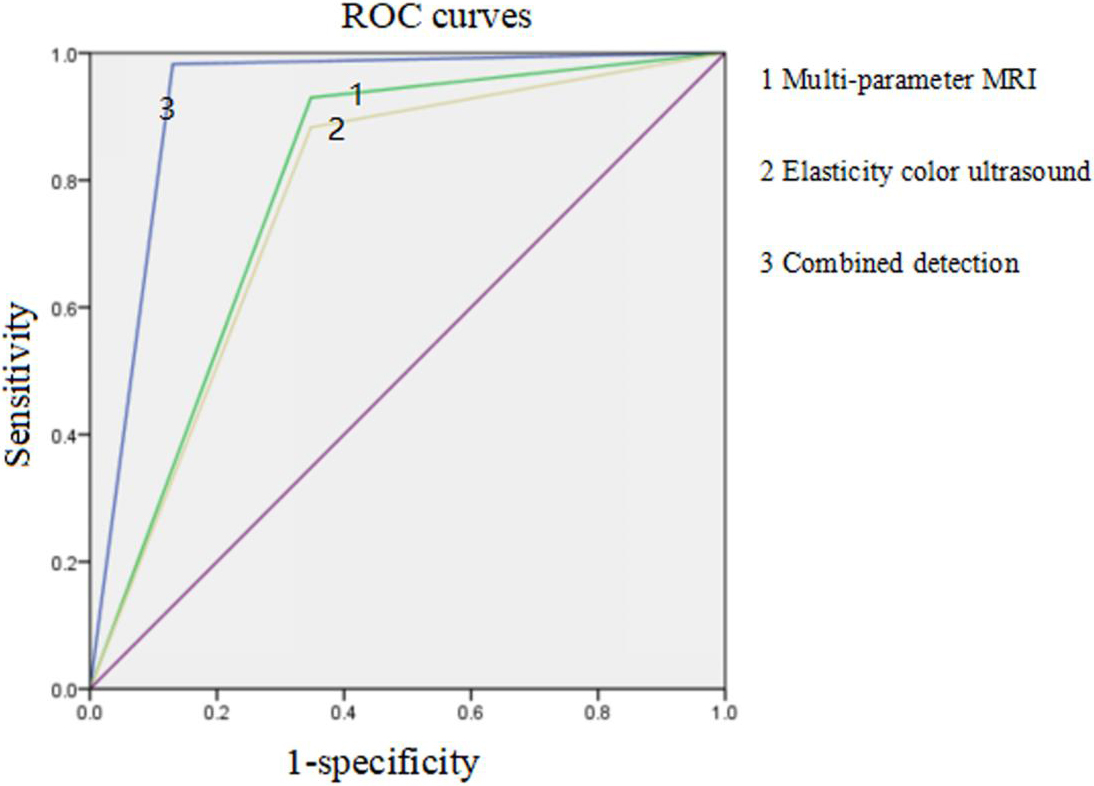
TMC has no obvious clinical manifestations and is also known as occult carcinoma [9]. The thyroid nodules in TMC are usually small and easily missed; some will cause cervical or distant lymph node metastasis, whereas some will show aggressive development [10]. Early diagnosis and timely treatment are the keys to improving the quality of life and prognosis of patients with TMC.
The hardness of thyroid nodules is closely related to the nature of the nodules. Benign nodules are composed mainly of follicular cells filled with glial components and have a soft texture. In contrast, malignant nodules are primarily composed of fibrous tissue, blood vessels and more calcified bodies, and they have a hard texture [8]. Currently, imaging methods are the main way to determine benign and malignant thyroid nodules, and the main detection techniques include B-ultrasound and MRI. Elastography is a new method for diagnosing benign and malignant superficial organ nodules. With the help of a probe, an external force is applied to the lesion. The hardness of the reaction tissue is determined by detecting the deformation degree of the lesion under the action of external pressure. Thyroid cancer has hard tissue because it is rich in fibrovascular bundles and psammoma bodies. At the same time, benign nodules are dominated by softer components, such as follicles and glia, so the tissue stiffness is low, and the texture is soft.
Some studies have pointed out that using colour B-ultrasound elastography combined with thyroid-imaging reporting and data-system grading helps sonographers reduce the determination of clinical subjectivity and effectively improves the accuracy of diagnosis compared with standard colour B-ultrasound [11]. In this study, the accuracy of colour B-ultrasound elastography was 85.57%, the sensitivity was 88.30%, and the specificity was 65.22%, which was consistent with the postoperative pathological diagnosis. The main reason is that colour B-ultrasound elastography technology can effectively show the deformation characteristics of parts with different hardness when lesions are compressed [12]. It has also been found that compared with standard colour Doppler ultrasound, colour B-ultrasound elastography diagnoses a lower proportion of benign thyroid tumours and a higher proportion of malignant thyroid tumours. Thus colour B-ultrasound elastography is more precise than standard colour B-ultrasound in distinguishing benign from malignant thyroid tumours because colour B-ultrasound elastography can analyse and determine the lesion from multiple perspectives, including the deformation and colour of the lesion [13]. Using color-coded virtual touch tissue imaging in acoustic radiation force pulse technology, Lian et al. studied the ability of color-coded VTI (CV) to distinguish between benign and malignant nodules, improving diagnostic accuracy [14]. Studies have also shown that gray-scale ultrasound combined with shear wave elastography and conventional ultrasound combined with color-coded virtual touch tissue imaging can improve the accuracy of diagnosis for benign or malignant of thyroid nodules [14, 15]. However, due to equipment limitations, these two methods were not used in this study. We will include these two methods for comparison in subsequent studies.
In recent years, artificial intelligence aided diagnosis system in thyroid ultrasound diagnosis play a unique advantage, can significantly reduce the work intensity, improve work efficiency and diagnostic accuracy [16]. The computer aided method based on geometric texture features can improve the accuracy of fetal hydrocephalus detection in ultrasonic images [17]. An expert diagnostic system that automatically identifies asthma and chronic obstructive pulmonary disease has high clinical value and can also reduce the need for additional tests and reduce financial costs [18]. However, in artificial intelligence diagnosis, it is not compared with the normal thyroid tissue of the patient, and can be affected by the diameter, location, adhesion or medium echo of the nodule, which reduces the nodule recognition rate. Color B-ultrasound elastography diagnoses benign and malignant thyroid nodules by obtaining the hardness information of the lesion tissue. The strain rate ratio (SR) is more objective in diagnosing the nature of thyroid nodules, and can quantitatively evaluate the elasticity score of the lesion tissue [19]. The combined diagnosis of artificial intelligence and SR can achieve complementary advantages. Based on the morphological characteristics of nodules, the hardness information of the lesion tissue is combined to determine the nature of nodules, thereby improving the diagnostic accuracy.
In routine MRI imaging, there is no specific difference in the signal between the thyroid gland and the surrounding soft tissues. Diffusion-weighted imaging and magnetic resonance spectroscopy are two new methods for diagnosing and treating thyroid diseases. The diffusion coefficient is an important observation index in DWI. Due to the denser connectivity of malignant cells, the increased nuclear-cytoplasmic ratio leads to the limited diffusion of water molecules in tissues and a reduced diffusion coefficient. Diffusion-weighted imaging is currently the only means to quantitatively reflect the diffusion movement of water molecules in living tissues by measuring the apparent diffusion coefficient (ADC) to differentiate benign from malignant tissues.
The mean ADC value of malignant thyroid nodules was lower than that of benign thyroid nodules. When the ADC value cut-off was 1
Multi-parameter MRI and ultrasonic elastography have high value in the identification of benign and malignant thyroid nodules, but both have no low false positive and false negatives. This study fully applied the characteristics of contrast-enhanced ultrasound and elastography, and thyroid nodules were analysed from different aspects. The detection methods of the two were complementary. After combined detection, the accuracy was 96.91%, the sensitivity was 98.25%, and the specificity was 86.96%, which were higher than with single detection. However, misdiagnosis still occurred. In this group, the size of the nodule was 11 mm. Contrast-enhanced ultrasound showed that the enhancement was slightly earlier than the surrounding glandular tissue, while most of the central contrast agent was not filled. Elastography green accounted for
This study has some limitations. First, because the data collection unit was a specialist cancer hospital, malignant nodules were significantly more common than benign nodules, and micropapillary carcinomas were more common among malignant nodules. Hence, there was a certain degree of selection bias. Second, in this study, the pathological type of benign and malignant nodules was not used as a factor in the multivariate prediction model.
Conclusion
The combination of multi-parameter MRI and ultrasound elastography has higher clinical value than a single detection modality in improving the diagnosis rate of benign and malignant thyroid nodules. The sensitivity, specificity, accuracy and kappa value of the combined diagnosis were 98.25%, 86.96%, 96.91% and 0.852, respectively. Ultrasonic elastography can differentiate benign and malignant thyroid nodules by elasticity grading and blood flow signal. Multi-parameter MRI can show the size, shape and internal signal changes of thyroid nodules. The combination of the two is helpful for the early diagnosis and clinical treatment of thyroid nodules.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Maanshan General Hospital of Ranger-Duree Healthcare. Written informed consent was obtained from all participants.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Funding
This study did not receive funding.
Author contributions
WF conceived the study. ZLP and JJX participated in the design, data analysis and statistics and helped draft the manuscript. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
Not applicable.
Conflict of interest
None of the authors have any personal, financial, commercial, or academic conflicts of interest.