
Abstract
BACKGROUND:
Edentulism conducts to a recognized impairment of oral function with both aesthetic and psychological changes. These patients suffer from a multiplicity of problems with their dentures, such as insufficient stability, retention and pain during mastication.
The rehabilitation of a part edentulous patient can be established using a wide range of prosthetic treatment options. The overdenture treatment uses a removable total denture that overlies retained teeth, tooth roots, or dental implants. In the literature it was shown that patients with removable overdentures supported and retained either by tooth roots or implants have more predictable prosthodontic outcomes.
OBJECTIVE:
The aim of this review is to provide an overview on the overdenture with a focus on the tooth-supported telescopic overdenture.
METHODS:
The literature research was performed in the Scopus, Web of Science, and Pubmed electronic databases. Document type was limited to papers written in English, without time restrictions. The Review was recorded in the international PROSPERO (International Prospective Register of Systematic Reviews) database with the following number CRD42022326415.
RESULTS:
A total of 256 articles published were found from electronic searches, Two independent reviewers carried out the screening and the selection process for the studies.
First, duplicate citations were eliminated. Then, the two Authors independently screened the retrieved articles by title and abstract of each citation to determine its suitability for inclusion. Finally, 13 full-text articles satisfied the inclusion criteria.
CONCLUSION:
Prostheses supported by Frictional telescopic crowns offer an effective treatment alternative for patients with Severely reduced dentitions who do not want implant treatment or complete dentures.
Introduction
Edentulism conducts to a recognized impairment of oral function with both aesthetic and psychological changes [1]. The prevalence of Removable Dental Prostheses (RPDs) among adults in Europe varied between 13% and 29%, with 3% to 13% of edentulous patients wearing complete dentures [2]. Edentulous patients with complete dentures are usually satisfied, but up to 30% of the patients have complaints [3]. They suffer from a multiplicity of problems with their dentures, such as insufficient stability, retention and pain during mastication [3]. Also, the patients who have originally adapted to wearing complete dentures may become maladaptive with time due to the continual residual ridge resorption, intraoral physiological changes and the development of an altered muscle pattern [4, 5, 1, 6].
In the past, patients were often rendered completely edentulous with fabrication of complete dentures [7, 1], but several studies have shown that removal of natural teeth and provision of conventional dentures results in alveolar bone loss [7, 3, 8, 9, 10], so this resorption can be prevented by retaining roots as overdenture abutments [8, 11, 12, 13, 14, 15].
The rehabilitation of a part edentulous patient can be established using a wide range of prosthetic treatment options [16, 4, 17], the available prosthetic options depend on the strategic decision to preserve a certain number of teeth with a good prognosis, or to removing all remaining teeth in a jaw, or to place implants [18, 19, 20, 21, 22, 23] at prosthetically favorable positions [24, 2, 25, 26].
Financial constraints and other priorities may limit the patient from choosing the most desirable treatment [27, 28, 29, 2], moreover only few patients are suitable for fixed implant-supported prostheses with crown design due to moderate or advanced maxillary atrophy [30, 31, 32]. In addition, often, a fixed prosthesis may be contraindicated due to few remaining teeth, abutments with an uncertain prognosis [2], or the need to reconstruct a large volume of lost hard and soft tissues [2, 30, 33, 34, 35, 36]. In fact, in a situation where there may be significant soft tissue loss and restoring the soft tissue is necessary for esthetics [37], the use of a full acrylic flange extension is mentioned for esthetic advantages and for facial support [30].
The advantages of overdentures over fixed prosthesis are lower cost, high esthetics, improved access to oral hygiene [30, 38, 39], and better distribution of occlusal forces [40, 41, 42, 43, 44, 45].
The aim of this review is to provide an overview on the overdenture with a focus on the tooth-supported telescopic overdenture.
Materials and methods
Eligibility criteria
All documents were assessed for eligibility based on the following Population (including animal species), Exposure, Comparator, and Outcomes (PICO):
P) Participants consisted of patients that need of full arches rehabilitation. I) Intervention consisted of tooth-supported telescopic overdenture. C) The comparison was patients with a complete denture or implant supported protheses. O) evaluate the beneficial effects of a telescopic prosthesis, and to compare to other rehabilitation solutions.
Only papers providing data at the end of the intervention were included. The following exclusion criteria were used: 1) articles which did not answer the key questions; 2) duplicate articles; 3) systematic and narrative review article; 4) case series and case report; 5) books; 6) letters to editors; 7) experimental studies. The database search was also supplemented with a hand search of relevant articles in the reference lists.
Search strategy
PubMed, Web of Science and Scopus databases were systematically searched for articles published from the inception until Jul 30, 2022, according to each specific thesaurus, following the strategy. The search terms contained “overdenture” combined with “natural teeth” combined with “telescopic” OR “double crown prostheses”. The web search was assisted by the use of MESH (Medical Subjects Headings). The criteria for this review are described in the PRISMA flowchart (Fig. 1). Furthermore, a manual search of the references of previous systematic reviews on a similar topic was conducted as well.
This systematic review was conducted according to the guidance of Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. The systematic review protocol has been registered on the International Prospective Register of Systematic Reviews (PROSPERO) under number CRD42022326415.
Data extraction
Two reviewers (G.M. and R.F.) independently extracted data from the included studies using a customized data extraction on a Microsoft Excel sheet. In case of disagreement, a consensus was reached through a third reviewer (M.C.).
The following data were extracted: 1) First author; 2) Year of publication; 3) Nationality; 4) Age of study participants; 5) Type of rehabilitation; 6) Beneficial effects on chewing; 7) Population and the number of patients included; 8) Main findings.
Quality assessment
The risk of bias was assessed by two reviewers using Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2). Any disagreement was discussed until a consensus was reached with a third reviewer.
Results
Study characteristics
At the end of the research, 256 studies were identified. Only 13 were chosen to draw up the present systematic study, as illustrated by the PRISMA flowchart (Fig. 1); 72 articles were removed before screening. The remaining articles were selected for the title and abstract screening according to the PICO model.
In the initial scan, articles were eliminated if they were clearly outside the aim of the review. All titles were checked, and 184 articles were selected for abstract reading. Then, the analysis of the abstracts excluded 125 articles that did not satisfy the eligibility criteria. Thus, 59 full-text references were identified, and 7 were not retrieved. Finally, 13 articles were present in the publication on the search engines used.
Main findings
Among the 13 studies, six were retrospective studies; four prospective studies, one was a Trial, 1 was a preliminary study, and 1 a Comparative study (Table 2).
Search strategy
Search strategy
PRISMA flowchart.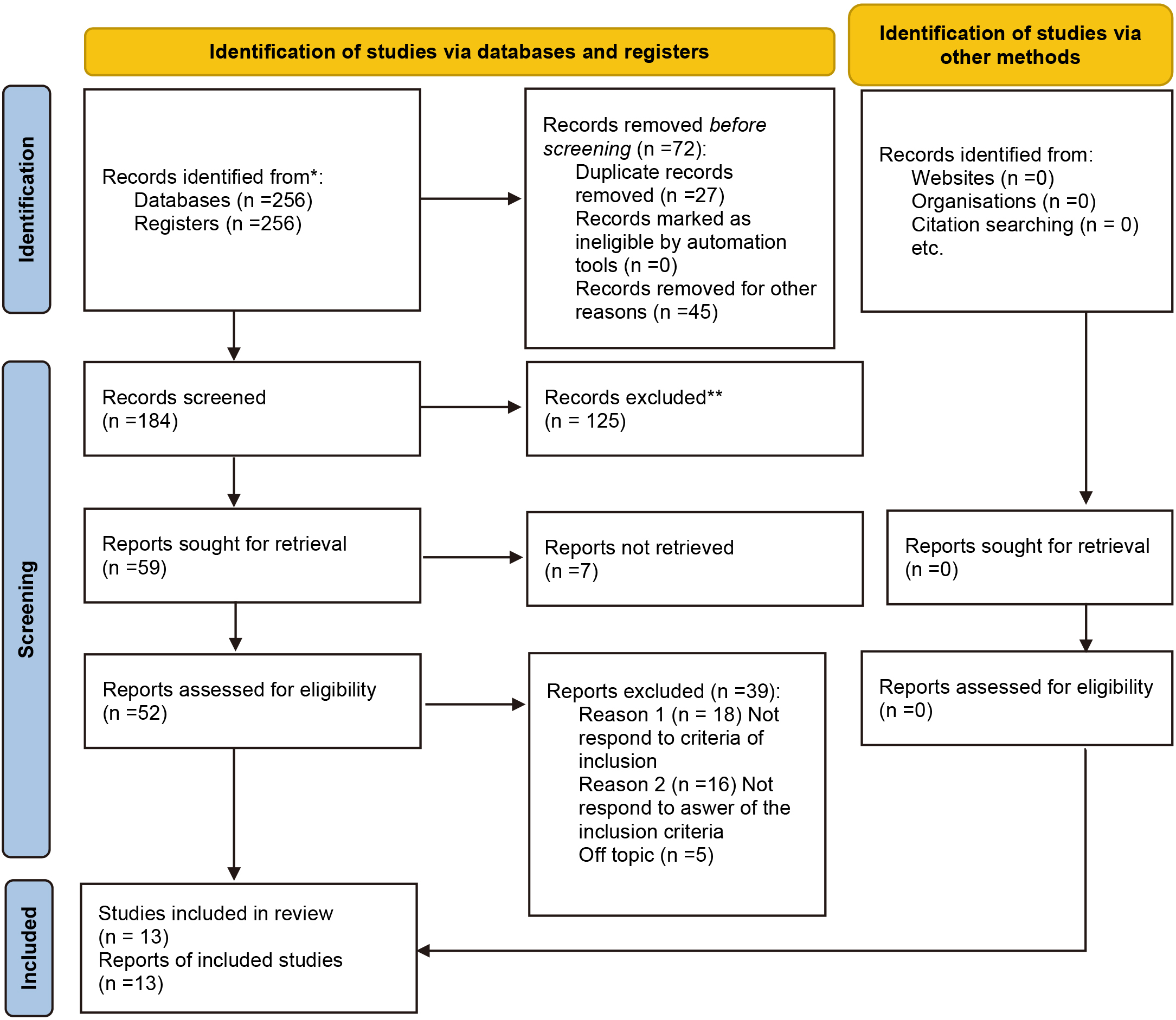
Features of included studies
Quality-assessment of included studies.
Using the RoB 2, the risk of bias among the studies analyzed was estimated and reported in Fig. 2. Regarding the randomization process, 95% of the studies ensured a high risk of bias. Only 25% of studies excluded a performance bias, but 100% reported all outcome data, and 100% of included trials adequately left out bias in the selection of the reported results. Overall, only 5 out of 13 studies were demonstrated to have a low risk of incurring bias (Fig. 2) (Table 1).
Discussion
Why chooses the overdenture?
Rehabilitation of a part edentulous patient can be established using a wide range of prosthetic treatment options [4, 17, 46, 47, 48, 49, 50].
The available prosthetic options depend on the strategic decision to maintain a particular number of teeth with a good prognosis, or to removing all remaining teeth in a jaw, or place implants at prosthetically favourable positions [2, 21, 22, 23, 51].
Financial limitations and other priorities may restrict the patient from choosing the most desirable treatment [27, 2].
Fixed prosthesis limitless
Only few patients are suitable for fixed implant-supported prostheses with crown design [30], in fact, many elderly patients show a highly reduced dentition with regard to the number of teeth lost due to periodontal disease or caries moreover often also due to moderate or advanced maxillary atrophy fabrication of fixed prostheses becomes impossible [1, 7, 42, 43, 52, 53, 54, 55, 56, 57].
The fixed prosthesis may also be contraindicated due to the need to reconstruct a large volume of lost hard and soft tissues [2, 30]. Today virtual planning aims to optimize function and esthetics prior to implant placement [30], so in the last decades there was a change in philosophy from “bone-driven” to “restoration-driven” implant dentistry was determined with regard to the prosthetic reconstruction [30].
Endosseous implants can be an alternative treatment [8], but it is not always possible to use them as presented by Avrampou et al., which showed that 36% of patients presented bone deficiencies that hindered prosthetically ideal placement of implants [30, 58, 59, 60].
Zitzmann and Marinello proposed a treatment concept that enables the practitioner to choose the appropriate type of restoration in consultation with the patient before the surgical procedure has been initiated. The systematical analysis and the classification presented by Zitzmann and Marinello give dentists the possibility to evaluate in detail the relationship of anatomical structures, implant position and teeth position and to explain specific aspects to the patient. Thus misunderstanding, possible difficulties, esthetic expectations, need for surgical procedures and absolute contraindications to fixed prothesis can be evaluated during the initial diagnostic phase [30, 61, 21, 22, 23, 51].
Esthetic advantages and facial support
In a situation where there may be significant soft tissue loss and restoring the soft tissue is necessary for esthetics [37], the use of a full acrylic flange extension is mentioned for esthetic advantages and for facial support [30, 43, 44, 53].
Facial support and natural lip mobility are crucial outcome parameters and important aspects that influence the decision between fixed and removable prostheses [30].
Acrylic materials, composites, and pink porcelain are described in the literature for the replacement of lost soft and hard tissues [30, 2].
Overdenture advantages
The overdenture treatment uses a removable total denture that overlies retained teeth, tooth roots, or dental implants [62, 1, 22, 23]. In the literature It was shown that patients with removable overdentures supported and retained either by tooth roots or implants have more predictable prosthodontic outcomes [63, 1].
Advantages of overdentures over fixed prosthesis are lower cost, high esthetics, improved access to oral hygiene [30, 21, 22, 23, 64], and better distribution of occlusal forces [40, 42, 47, 48, 53]. Moreover, provision of the tooth and implant-supported overdentures would beneficially aid the edentulous patient in maintaining their masticatory force, biting force and occlusal vertical dimension rather than rendering them completely edentulous [3, 44, 46, 52].
Implant overdenture vs natural teeth overdenture
Over the past years, titanium implants have been promoted as successful for tooth replacements [7] and to prevent the loss of alveolar bone in height [3]. However, the biological basis of implants provided in the bone is distinct from roots enveloped by a periodontal membrane, but the prosthetic concept is similar [65, 42, 46, 54, 57].
Several studies showed a high success rate for implant overdentures in the mandible, whereas treatment outcomes with maxillary overdentures appeared to be less predictable [7, 18, 20, 60]. Gargari et al. compared the Implant overdenture and the natural teeth overdenture showed that between the quality of mastication, phonetics and capacity of expression were not statistically significant [65].
Comparison between aesthetics for the two types of overdenture shows a good level of satisfaction, slightly higher in the group treated with tooth-supported overdenture [65, 35, 46, 50, 57]. They have not found differences even regarding the facility of cleaning the prosthesis [65]. Comparison between the facility of removal and insertion of the denture for the two types of overdentures shows a slightly higher easiness in the group of implant-support overdenture, but there isn’t statistically significant [65].
The result of this study also demonstrated a significant increase in maximum biting force one year after for implant and tooth-supported overdenture groups compared to the conventional immediate denture group. This result may be due to the good support and stability of the tooth and implant-supported overdentures compared to the mucosal-supported dentures [3, 20, 58, 59, 66].
In a comparison of maximum biting force [18, 19, 20, 21, 22, 67] for tooth and implant sustained overdentures, the implant-supported overdenture group experienced a larger increase in the maximum biting force than the tooth-supported group [3], in fact the masseter muscles’ electromyographic activity in the tooth-supported overdenture group is lower than in others [3, 68, 69], which suggests that the periodontal ligament plays an essential role in the efficiency of the muscular activity during chewing in patients wearing an overdenture prosthesis [3, 70].
Patients with tooth-supported prosthesis still had tactile proprioceptive reflex arising from the periodontal ligament that alarms them against overload [3, 65].
The periodontal ligament and osseointegrated interface distribute force otherwise to the supporting bone [40, 21, 22, 23, 51], in fact the periodontal ligament of a tooth distributes the forces to all the surrounding bone, whereas the osseointegrated interface concentrates the force at the crestal bone [40, 18, 20, 21, 22, 51, 59].
Combined tooth-implant support in removable prosthetics
In removable prosthodontics a symmetric bilateral distribution is suggested to enhance the stability of the prosthesis, in fact when a very limited number of teeth can be maintained [7], the placement of a strategic implant on the opposite side of the arch to equalize the balance and create suitable support and retention is a suggested option [63, 17]. Presently, the question of different loading schemes on teeth with periodontal ligaments versus osseointegrated implants in the eld of removable prostheses, as well as the possible risk for an intrusion phenomenon of the natural telescopic abutment, as described on fixed tooth-implant reconstructions, is still unclear [17, 44, 49, 53].
In a combined overdenture, where there is a flexible connection between the overdenture and primary structures, the force applied to the tooth side will not be transmitted to the implant side in a deleterious manner as there is a stress breakage at the attachment level. For this, overdentures should be designed in such a way that prosthesis should be able to rotate at the attachment level without torquing on the primary bar [22, 23, 51, 59]. Parallel milling with a close fit in such cases can transmit these deleterious forces to the implants, hence should be avoided. In addition to this, the stress equalization between the natural tooth and implant can be done by the placement of nylon caps with different degrees of resiliencies. As there is stress breaking between the final prosthesis and both implant and tooth and the implants being splinted together, there will be even stress distribution among them [40, 43, 46, 52].
Finally, the concept of combined tooth-implant-retained telescopic prostheses improves the loading protocol for stable quadrangular support and appears to ensure successful function over a midterm observation period [17].
Natural teeth abutment advantages
The success factor of an overdenture is the selection of strategic roots or teeth for retention, in fact an elective endodontics, and periodontal therapy make them excellent abutments for an overdenture [71], furthermore the shortened crown improves the crown-to-root ratio therapy decreasing the motility of the abutment teeth under an overdenture (25% of roots that were initially mobile became less mobile) [71, 36, 44].
Not to be forgotten that the presence of a healthy periodontal ligament maintains alveolar ridge morphology and dimensions [62, 25, 57, 72].
Reassuming the goals of maintenance of roots and using them as abutments are to prevent alveolar bone resorption, provide better load transmission of the prosthesis to the underlying structures, maintain sensory feedback [7, 3], and achieve better stability of the dentures [7, 8, 70, 65, 3], further the psychologic aspects [73] of not being completely edentulous must be emphasized [8, 70, 74, 7].
Natural teeth abutment risk
Recent studies with long term results exhibited a high survival rate (80%) of abutment tooth [8], Toolson and Taylor showed that the major biological complications affecting the tooth abutments were gingival inflammation, loss of pulp vitality, periodontal disease, caries and tooth fractures [2, 7, 75] but it is essential to remember that no caries lesions may be the result of the regular recalls and short observation period [7]. Moreover, it was also shown that caries development under overdentures could be inhibited completely with daily application of clorhexidine-fluoride gel [7, 26, 33, 34].
Regular maintenance care, topical fluoride [7] use and oral hygiene have been identified as important factors in abutment longevity [72, 76, 77]. When these factors are controlled, even teeth with a relatively poor prognosis can be successfully utilized as overdenture abutments [8, 66, 78]. Anyhow in case of a failing abutment tooth, the reconstruction can more easily be modified compared to a fixed dental prosthesis (FDP) [2, 43, 44, 45].
Prothesis connections
The overdenture has many benefits and many options are applicable for retention of the prosthesis, including magnets, clips, bars and balls [65, 1]. But no single attachment is perfect for every case, so it is critical that the appropriate attachment should be chose for each individual situation [62, 46, 47, 48].
Telescopic crowns
Telescopic crowns (also known as a double crown) were originally used as retainers for RPDs at the beginning of the 20th century [1, 74], and continues to serve as a valuable therapeutic restorative option today [37, 18, 19, 21, 22, 23, 51, 59, 60]. They consist of an inner primary telescopic coping cemented to the abutment and a harmonious secondary coping embedded into a removable prosthesis [74, 1, 75].
The secondary coping forms a telescopic unit over the primary copings and aids in the anchorage of the remaining dentition. Telescopic crowns have been used mainly in such situations to connect dentures to the remaining dentition, and these can be used really to retain complete dentures which obtain their support in part from the abutments and partly from the underlying residual tissues [4]. Moreover, telescopic retainers to being cost-effective, increased the range of treatment alternatives in patients with lower dentition, by blending the advantages of both fixed and removable prosthesis [27, 26, 41, 44, 56], in more general terms of better distribution of stresses, rigid bilateral splinting, good retentive, and stabilizing properties [27, 74].
A telescopic prosthesis can be constructed to be removed daily, enabling the patient to effectively remove plaque at the gingival crest [37, 79]. Moreover, the telescopic crowns are the least expensive and are very successful if properly maintained by the patient, in fact it requires a high polish of the denture surface, fluoride maintenance and attention to oral hygiene [1, 35, 36, 76].
Patient removability of the secondary structure facilitates abutment hygiene, making the telescopic crown system more acceptable from a periodontal perspective [74]. Major aspects for a long-time stable treatment success are the number and the strategic distribution of the telescopic double crown abutments [80, 2]. Many times, reported technical complications were the loss of retention of the primary double crowns and loss of facings of the outer frameworks [2, 50, 53, 54]. Moreover, a telescopic prosthesis is a more versatile alternative because the prosthesis can be repaired without reconstruction of the entire superstructure, despite a localized failure of weaker abutment [1, 37, 27, 74], so a lost abutment can be dealt with by simply filling the overcrown with acrylic resin to form a pontic [37].
Telescopic alternatives: Conical vs cylindrical
Usually, 2 different mechanisms of retention are used: parallel-sided primary and secondary crowns or cone-shaped primary and secondary [75, 80, 2], and double crowns with additional retention modifications [2], by using additional attachments (e.g., the TC-SNAP system [Marburg double crown]) [2]. The conical crown system was introduced by Körber, and the parallel-sided crown system firtly was described by Böttcher [75].
The fabrication of the parallel-sided crowns in particular is considered to be very difficult because this system requires a clear fit between both crowns for appropriate retention [80], that occurs through the force of friction [61, 2, 2, 61, 46, 47, 48]. The difference between the conus and the cylindrical crowns is the certain taper on the vertical surface of the conus crowns [81].
Yalisove and Dietz showed that in telescopic crown-sleeve-coping restorations, the effective crown-to-root ratio is reduced at the point that the telescopic overcrown rotates [37]. The reason for this, is the geometry of the crown. While in cylindrical telescopic crowns all the walls are parallel, in a conus crown, the parallelism only occurs in between the contact surfaces of the inner and outer crowns [81]. Another characteristic for the adaptation of the conus crown is the creation of a pressing effect [81].
In the cylindrical telescopic crowns, the surface is prepared parallel and a piston-cylinder effect occurs. Because of the continuous contact, it can act as a force arm. As a result of this perpetual friction, the abrasion ratio on the surface increases [81, 21, 22, 23]. The primary and the secondary crowns hold each other at the contact surfaces instantaneously [81, 45, 55].
During the removal of the denture, these contact surfaces depart from each other increasingly from the initiation [81]. In the cylindrical telescopic crowns, a frictional movement occurs on all surfaces starting from the first lodging of the prosthesis on the abutments [81].
The mechanism of retention of the cylindrical telescopic crown is based on the frictional force between external and internal surfaces, and this depends on the precision of component production [75, 19, 20, 60]. Therefore, the conus crowned prostheses can be removed without friction and contact with the first forcing movement [81].
The conus crown must have a certain degree, and this should be decreasing gradually as the retention is gained instantaneously [81, 36, 41, 53, 54]. Thus, a retentive force occurs and the already seated crown cannot be removed easily. In technically perfect and smooth- surfaced conus crowns, the retentive force is determined by the angle of the conus crown [81].
Telescopics prothesis difficulties
Manufacturing dentures supported by double crowns is difficult and expensive and requires special technical skills that only a well-trained and experienced dental technician can master [80, 35, 36]. The great disadvantages are the high demand on precision and special skills needed of both the dental mechanic and the clinician in the fabrication of double crown reconstructions, consequently growing the total cost of the prosthesis [2, 18, 20, 22].
Retentive force of the telescopic crowns
However, the retentive force required to make a denture adequately fixed, functional, and satisfactory for the patient has not been elucidated, the retentive force of each individual tooth for the cone crown telescopic system has been indicated to be 5 to 9 N [82].
Many factors influence the retentive force, including: height of conical crown, tapered angle, inner crown form, thickness of the outer crowns, alloy utilized for crowns, gap width in the occlusal region between inner and outer crowns, and surface roughness of cone crowns [82, 50, 52, 53]. In particular, the greater height of the cone crown telescopic system increases the retentive force. The retentive force increases also with thicker outer crown and as the gap width between inner and outer crowns builds up, regardless of the height of the cone crown [82]. Moreover, the retentive force increases when spittle or water is coated on the inner crown surface [82], while the retentive force fails as the tapered angle increases [82, 46, 47, 48].
In addition, the retentive force decreases more quickly when using an alloy of low hardness (it is the highest when gold alloy is used, followed by cobalt chromium alloy, CP Ti [Grade 2], and titanium alloy [Ti-6Al-7Nb]) [19, 20, 21, 58].
Surface roughness is believed to influence the retention, and so the surface roughness of the cone crown telescopic is likely to affect the retention of RPDs [82].
The mechanism of retention of the telescopic crown is based on the wedge effect, enabled by a small occlusal space between the primary and secondary crown [75, 42, 43, 44]. If the gap is too large, the structure will be loose and the retention of the denture will be inadequate [75]. If the gap is too small, it will be difficult for the patient to insert and remove the denture, which can have a destructive effect on abutment teeth and could result in deformation or decementation [75, 42, 43]. The retention of conical crown-retained dentures diminishes with time due to the insertion and removal of the dentures [75].
Ohkawa et al. reported a decrease in retentive forces after 10 000 insertion/separation cycles [81]. Previous studies report that the retention would decrease by the abrasion on the metal as a result of long-term removal [81, 33, 42, 43, 44]. As documented by Becker for the telescopic system and Körber for the conical double crowns, retention forces of 3.5 to 7 N should achieve adequate denture retention [83]. Becker reported that the change in the surface characteristics of the frictional surfaces of the telescopic crowns would cause differences in retentive forces and that saliva also affects the retention [81, 19, 22, 58, 59, 60]. In a study where two different casting methods were used, Wegmann and Maas indicated that the differences in the casting procedure would cause differences in retention [81]. As the crown height increased, the retention values increased, this increase too was more obvious in smaller angles [81, 47, 48, 49, 52, 53]. In fact, the majority of the authors report that the retention decreases as the conus angle increases [81]. Therefore, for a long-term use, the conus angle of telescopic crowns should not be tapered more than 2
In summary, the retentive force of the telescopic crowns is influenced by the convergence angle, height and width of the primary crown, fit of the secondary crown, gap amount at the occlusal portion, applied load, materials used, and age of the denture [75].
Telescopic prognosis
Long-term prognosis of conventional double crown-retained RPDs depends on the total number of the involved abutment teeth [17, 84]. When tested the clinical survival rates, the telescopic abutment selection is very important for the long-term success of the entire restoration [2]. On one side, the loss of one abutment will result in a loss of the complete restoration when the telescopic denture is sustained by only two double crown abutments [2].
On the other side, it is simple to balance for abutment loss when telescopic supports are made for all remaining teeth because this concept enables an easy modification while maintaining the function of the restoration [2, 36, 42, 46, 47]. Therefore, it can be anticipated that the long-term success of telescopic-retained dental prostheses is highly dependent upon the number [17, 2, 85] and topographic distribution of the remaining abutment teeth [17].
Significant differences in the long-term behavior have been reported between treatments with fewer than 3 abutment teeth and those with 4 or more [84]. Full-mouth reconstructions supported by fewer than 3 abutment teeth were less favorable in the distribution of loading forces and had a significantly limited survival probability [2, 17]. Moreover, the integration of one to three telescopic abutment teeth was less favorable with regard to the prosthetic loading forces, especially if the distribution of these abutments was arranged in a tangentially or cross- arch linear relation to the arch [17].
The probability 5-year survival valued for dentures with only one support was 70.9% compared to 90.4% with two, 95.0% with three, and 97.9% with four abutments [2]. With 3 abutment teeth for the prosthesis, the long-term prognosis after 5 years will decrease from 90% to 70%, while prognostic survival rates of more than 85% after 5 years have been reported by virtually all authors when using 4 or more abutments [84].
Although an often-overlooked technique, the use of telescopic retainers continues to allow treatment options for prostheses that improve access for cleaning by the patient and/or dentist and retain questionable teeth longer [37]. While assessment of hygienic parameters for implant abutments and natural tooth abutments demonstrated satisfactory soft tissue conditions for both abutments [84]. This prevents leakage between a natural teeth abutment and its over-prosthetic restoration that could contribute to cement failure or caries [37].
Major technical problem
The major technical problem for the telescopic dentures is a loss of retention observed in (25%) dentures [2]. Technical complications for tooth-supported reconstructions encompassed loss of retention, abutment tooth fractures [2], and the risk of vitality loss in the abutment teeth after the insertion of conical crown retained dentures (CCRDs), that was evaluated by Walther in 655 patients with 787 dentures (2478 abutments) for up to 8 years [2, 21, 22, 23, 51, 58]. During the observation time, 183 abutment teeth in 134 patients failed vitality and were treated endodontically. Furthermore, 916 (37%) abutments had an advanced periodontal breakdown, and 34 (1.3%) fractures occurred [2]. Often reported technical complications were the loss of retention of the primary double crowns and loss of facings of the outer frameworks [2, 34, 35, 36, 44, 45].
The principal reasons for the denture failures were the loss of support teeth and denture fractures [2, 21, 22, 23]. In conclusion, the telescopic dentures required a higher rate of maintenance service than conventional RPDs [2, 27, 20].
Materials
Major skill, complex laboratory procedures, and increased bulk are some of the disadvantages with double crown systems. These obstacles are unimportant in light of many advantages it offers above all with the introduction of cheaper and less dense casting alloys. Materials utilized for the inner and outer crowns are gold alloys, Cr-Co metal alloys, titanium, and zirconia [2, 46, 47, 53, 55], but the recommended alloy for fabrication of telescopic and conical crowns is the one that is high in gold content, and elastic modulus together with being very hard (ADA Type IV) [81]. Although the suggested alloy for fabrication of copings is type III gold alloy for technique sensitivity but for the high cost it can be replaced Co-Cr alloys which though not ideal It is a cheaper substitute [27, 18, 20, 60].
No significant difference or any changes in retentional values between the titanium and golden secondary crowns were observed [81]. While the use of base metal alloys is rare because of the practical and technical difficulties associated with these materials, both telescopic and conical double crowns can solely provide rigid support [81, 46, 48, 49].
Technical problems and difficulties in manufacturing prostheses
One of the most common problems associated with the tooth-supported telescopic prosthesis during clinical and laboratory procedures is the unseating of the denture.
This mainly occurs during the transfer of the secondary copings to the prosthesis using the direct or indirect technique [74, 20, 21, 22, 58].
The accuracy of the fit of the tooth-supported telescopic prosthesis is greatly affected by the transfer of the spatial relationship of the secondary copings intraorally to the master cast. Unseating of the tooth-supported telescopic overdenture is mainly attributed to the misfit of the secondary copings. It occurs as a result of dimensional changes of the impression material and denture base material and micromovement of the secondary copings within the denture base material used for fabrication of record bases.
To prevent the aforementioned problem, a reliable and accurate method will be achieved by a rigid connection between secondary copings to preserve the spatial relationship independent of denture base material used. Thus, a simple procedure involving the splinting of the secondary coping using self-cure acrylic resin was developed by Swapnil et al. in 2017 [74, 46, 47, 48]that suggested a simple technique to maintain the spatial relationship of the secondary copings to each other and in relation to the primary copings intraorally, in a tooth-supported telescopic denture.
Conclusion
Prostheses supported by Frictional telescopic crowns offer an effective treatment alternative for patients with Severely reduced dentitions who do not want implant treatment or complete dentures [85]. This protocol appears to be feasible when strict recalls and a rigorous maintenance program are followed. The technique’s documented favorable clinical outcomes of comfort and satisfaction combined with good (unlimited) repair capability are particularly encouraging. The risk of loss of telescopic crowns depends significantly on abutment tooth distribution, and the retention of weaker or nonvital teeth may be employed to improve and enhance abutment support [85].
Telescopic overdenture benefits:
Preservation of the residual alveolar ridges for a longer duration due to counteracting action of the remaining natural teeth, in comparison to conventional complete dentures. Direction of vertical forces along the long axes of the teeth, favorable for the abutment teeth. Maintenance of oral hygiene and periodontal health around the abutment teeth, due to the easily accessible and cleansable areas after removal of prosthesis from the mouth. The splinting effect of a telescopic overdenture has a favorable stabilizing effect on the remaining dentition. Can be removed and repaired in case of failure of the abutment teeth, without reconstructing the entire pros-thesis. Greater psychological benefit to the patient on assurance of retaining the natural teeth [74].
Footnotes
Conflict of interest
None to report.