
Abstract
BACKGROUND:
The relationship between metabolically healthy obesity (MHO) and cardiovascular disease (CVD) risk remains debated. The critical point may be the lack of consensus on MHO’s definition and diagnostic criteria.
OBJECTIVE:
This study aimed to investigate the association of MHO status with arteriosclerosis-CVD (ASCVD) risk in Chinese under new diagnostic criteria.
METHODS:
Participants aged 35–79 in the 2009 China Health and Nutrition Survey cohort were included. The 10-year ASCVD risk was predicted by the prediction for ASCVD risk in China, and participants with a predicted risk of
RESULTS:
The 10-year ASCVD risk score and the proportion of individuals at ASCVD high risk were significantly different between metabolically obesity phenotypes (
CONCLUSION:
These results showed that there was no significant increase in ASCVD risk of MHO phenotype based on the new diagnostic criteria, suggesting that MHO is in a relatively healthy state.
Introduction
In recent years, overweight and obesity have become a worldwide epidemic. According to The Lancet, from 1975 to 2014, the rate of adult obesity in men increased from 3.2% to 10.8% and from 6.4% to 14.9% in women [1]. Obesity is a significant risk factor for many chronic diseases, such as cardiovascular disease (CVD), and contributes to the increasing morbidity, mortality, disability, and medical costs of these CVDs [2, 3]. Finding a specific subset of the obesity phenotype resilient to obesity-related cardiovascular outcomes allows us to focus interventions on those who may benefit most and develop personalized treatments.
Recently, related studies have found significant heterogeneity in the body fat distribution and metabolic indicators of obese people [4]. Some obese people do not show abnormal cardiometabolic characteristics but have higher insulin sensitivity, healthier blood pressure, blood glucose, blood lipids, and other metabolic conditions, known as “metabolically healthy obesity (MHO)”. There is an ongoing debate about the association between MHO with CVD and other poor clinical prognoses. The previous systematic reviews and meta-analyses have concluded that MHO is associated with an increased risk of developing CVD. However, recently studies have shown that MHO has a significantly lower risk of metabolic diseases, CVD, and other adverse clinical outcome events compared with metabolically unhealthy obesity (MUO) [5, 6]. The high heterogeneity and conflicting results observed in those studies are largely due to the absence of a uniform definition and diagnostic criteria for MHO and the use of different outcome definitions [7, 8].
In previous studies, the definitions related to metabolic health were frequently based on the absence of metabolic syndrome (MetS). Theoretically, CVD and mortality risk of individuals with MHO should be similar to those in metabolically healthy normal-weight (MHNW). However, studies in large-scale cohorts and meta-analyses found significantly increased CVD risk and overall mortality in individuals with MHO despite meeting the most stringent criteria of MetS [9]. Then, some researchers question whether the previous definition and diagnostic criteria of metabolically healthy may not be sufficient to identify risk-free MHO individuals. In 2021, Zembic et al. established a new definition for metabolically healthy based on the mortality follow-up of the third National Health and Nutrition Examination Survey (NHANES-III) and validated it in an independent cohort (UK Biobank) [10]. There is no report on the relationship between the MHO population and CVD risk in Chinese based on their diagnostic criterion.
Therefore, this study aimed to explore the association between the MHO population and the risk of arteriosclerosis-CVD (ASCVD) under the new diagnostic criteria based on the Chinese cohort.
Materials and methods
Study population
Participants came from the China Health and Nutrition Survey Cohort study (CHNS). The CHNS cohort study began in 1989 and is an ongoing, long-term follow-up survey that selected populations from 9 provinces through multi-level sampling [11]. A detailed description of the study design, eligibility criteria and sampling has been published previously [12]. The study was approved by the University of North Carolina Review Board and the Ethical Review Committee of the Institute of Nutrition and Health of the Chinese Centers for Disease Control and Prevention. All participants offered informed consent. Participants and data were from the 2009 CHNS database (
Data collection
The general information of the subjects was obtained by face-to-face questionnaire. Information on demographic data (age, sex, marital status, and education level), behavioral lifestyle (smoking, alcohol consumption, physical activity), personal health status and medical history, family medical history, and medication use were collected.
The physical examinations of subjects were measured by medical professionals following standardized procedures. Body Mass Index (BMI, kg/m2) was calculated as weight (kg)/height (m)2, and WHpR was calculated as waist/hip. Blood pressure measurements were repeated 3 times after a 10-minute sedentary rest, and an average of 3 times was taken.
Blood routine and other blood biochemical indexes were measured by the standardized process in the local laboratory at the scene of the investigation. Data on fasting plasma glucose (FPG), lipids, total cholesterol (TC), low-density lipoprotein (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and uric acid (UA) were collected.
Diagnostic criteria of metabolically healthy phenotype
Diagnostic criteria for metabolically healthy refer to the latest diagnostic criteria proposed by Zembic et al.: a) SBP
According to the definition of BMI level and metabolic status, the subjects were divided into six following metabolic obesity phenotypes: MHNW, metabolically healthy overweight weight (MHOW), MHO, metabolically unhealthy normal weight (MUNW), metabolically unhealthy overweight weight (MUOW), andMUO.
ASCVD risk assessment and grouping
ASCVD risk assessment was performed using a Chinese population-based prediction for ASCVD risk in China (China-PAR) model on an online website:
Statistical analysis
Bayesian network (BN) models were used to construct the network structure of the associations between metabolic obesity phenotype and the risk of ASCVD. The BN is a statistical method for inference and data analysis of uncertain information based on the principle of probability propagation [17]. The construction of the BN model mainly includes two parts: structure learning and parameter learning. In the first stage of manual construction, the prior knowledge of clinical experts was effectively embedded into the network structure through Whitelist and Blacklist. In the second stage of data-driven, the Tabu search algorithm and Bayesian information criterion score were used to learn the network structure and parameters [18, 19]. The stabilities of the arcs in the network were examined from 300 bootstrapped networks based on the original database, and the arc strengths were estimated by averaging the probability of the arcs presenting in these bootstrap-resampled network structures. The specific strengths thresholds were selected to construct network structure models of 10-year ASCVD risk and metabolically obesity phenotype.
Statistical analysis was performed using R 4.1.2 software. Continuous variables were presented as mean
Results
Characteristics of the study population
Table 1 shows the characteristics of the study population. Among the 6,108 participants, 2,817 (46%) were men. Except for drinking history, there were significant differences in demography, biochemical indexes, hyperuricemia, hypertension and diabetes status among the six groups (
ASCVD risk among different metabolic obesity phenotypes
In this study, the 10-year ASCVD risk of this population was 5.09
Construction of BN model
In this study, the nodes in the BN model include age, sex, metabolic status, BMI level, smoking history, drinking history, hyperuricemia, diabetes, hypertension, dyslipidemia, eGFR, hs-CRP and ASCVD risk classification. As shown in Fig. 1, age and gender are directly connected with ASCVD risk; dyslipidemia indirectly affects the ASCVD risk by affecting metabolic status, gender and other intermediate nodes. In addition, dyslipidemia is indirectly linked to sex through node hyperuricemia. Diabetes and eGFR are indirectly associated with ASCVD through metabolic status and sex, respectively.
Reasoning of BN model
Figure 2 shows the conditional probability distribution of metabolically obesity phenotype and 10-year
General characteristics among the study populationa
General characteristics among the study populationa
The 10-year ASCVD risk scores and grades of different metabolic obesity phenotypesa
a. The 10-year ASCVD risk scores and grades of different metabolic obesity phenotypes were evaluated based on China-PAR.
Bayesian network model DAG plot of metabolic obesity phenotype and 10-year risk of ASCVD.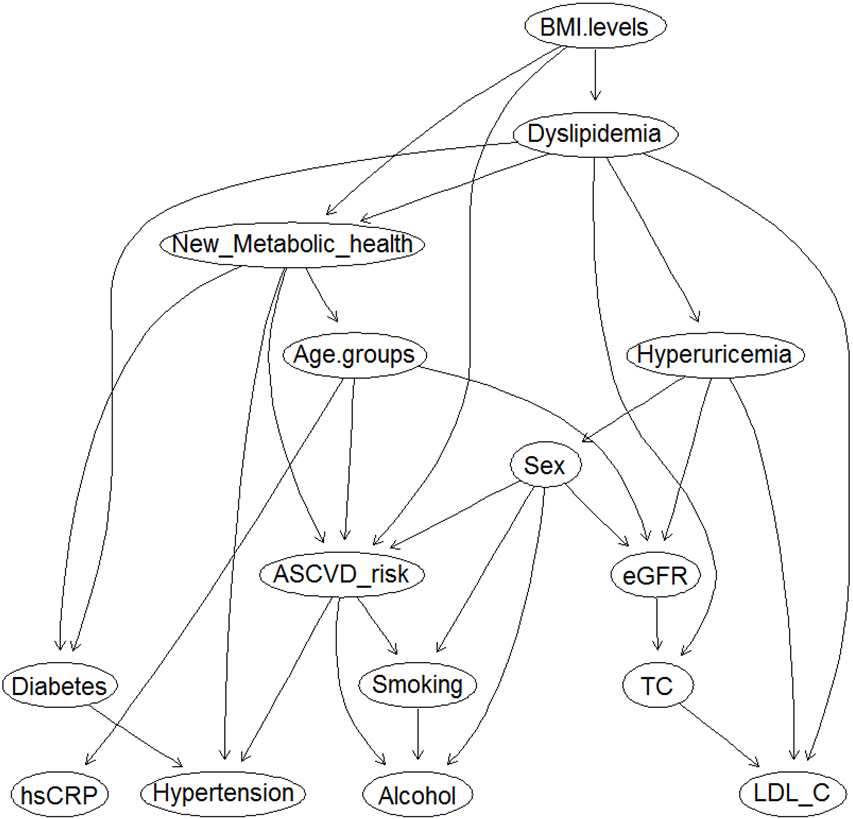
Inference and gender subgroup analysis of the 10-year risk of ASCVD in different metabolic obesity phenotypes.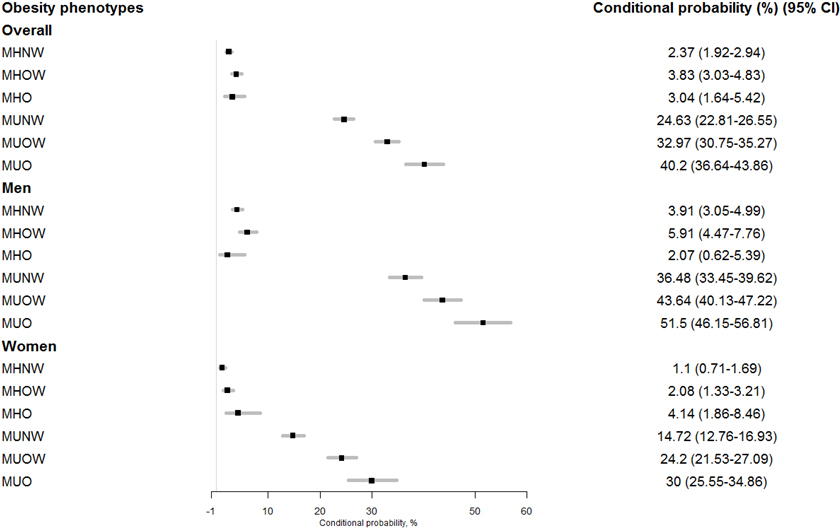
ASCVD risk. There was no significant increase in the risk of ASCVD in the MHO group compared with the MHNW group (3.04%, 95% CI: 1.64–5.42; vs. 2.37%, 95% CI: 1.92–2.94). However, in the metabolically unhealthy groups, the high-risk risk of ASCVD increased with elevated BMI levels; in the MUNW group (normal weight), the ASCVD high risk was 24.63% (95% CI: 22.81%–26.55%), while in the MUO group (obese) the ASCVD high risk was 40.2% (95% CI: 36.64%–43.86%).
After stratified by sex, there was no significant increase in the risk of ASCVD in the MHO group compared with the MHNW group in men. In women, the 10-year risk of ASCVD in the MHO group was 4.14%, which was significantly higher than that in the MHNW group (1.10%, Fig. 2).
In this study, we observed that the conditional probability of 10-year ASCVD risk in the Chinese MHO population was 3.04%. There was no significant increase in the risk of ASCVD in the MHO group compared with the MHNW group, while the 10-year ASCVD risk increased significantly among metabolically unhealthy groups. Besides, the significant associations between MHO phenotypes and 10-year ASCVD risk were only found in females. The new diagnostic criteria can accurately distinguish “healthy” obese people, but there may be some gender heterogeneity.
At present, MHO is an important research direction in the field of obesity, and the focus is mainly on whether MHO can be defined as a benign category of obesity. Based on the previous theoretical definition, there is no significant difference in the risk of CVD or other adverse clinical outcome events between the MHO and normal populations [7, 8, 21, 22]. For example, Lin et al. found that stable MHO status did not increase ASCVD risk based on a Chinese cohort study with an average follow-up of 4.4 years [8]. Similarly, Mongraw-Chaffin et al. found no significant increase in the risk of CVD in MHO groups compared with MHNW groups based on the USA MESA prospective cohort study [7]. However, recently, some large prospective cohort studies have shown that the MHO group is significantly associated with poor prognosis of CVD and the risk of all-cause mortality [5, 23, 24]. Two prospective cohort studies from the US Nurses’ Health Study (5) and the UK Whitehall II [24] have confirmed that MHO individuals without CVD history at baseline were at increased risk for CVD after long-term follow-up. Similarly, in 2020, a national cohort study based on The China Kadoorie Biobank also showed that MHO individuals had an 8% higher risk of developing 10-year CVD than MHNW individuals [6]. The association of MHO phenotype with CVD risk varies from non-significant to statistically significantly positive.
Results on CVD and mortality risks of MHO remain inconsistent. Using varying definitions for metabolically healthy might be responsible for the observed heterogeneity. It is reported that there are more than 30 different diagnostic criteria for MHO, according to which the prevalence rate of MHO ranges from 1.4% to 40.2% [25]. Therefore, diagnosing MHO scientifically and reasonably is an essential prerequisite for studying the relationship between MHO and other metabolic obesity phenotypes and disease prognosis. Zembic et al. found that the phenotype of MHO based on conventional MetS or HOMA-IR diagnosis has different results on CVD risk in the NHANES-III and UK Biobank cohorts. Thus, they proposed new diagnostic criteria for MHO and confirmed that MHO was not associated with increased CVD and all-cause mortality, suggesting that the new diagnostic criteria are superior in distinguishing between at-risk and not-at-risk obese individuals [10]. To our knowledge, this study was the first to explore the association of metabolically obesity phenotypes with a 10-year risk of ASCVD in a Chinese population using a BN model. According to the new criteria, about 1/3 of obese individuals are classified as MHO phenotype; compared with MHNW individuals, there was no significant increase in ASCVD risk in the MHO population. On the contrary, the risk of ASCVD in metabolically unhealthy was significantly elevated and independent of BMI levels. The results of the latest Korean community population cohort with new diagnostic criteria were consistent with this study [26], which found no significant association between MHO and CVD risk (subclinical atherosclerosis). Furthermore, we further explored the relationship between MHO and 10-year ASCVD in different genders, and found no significant association of MHO and ASCVD risk in males. We speculate that the new diagnostic criteria may be gender-specific. However, since this study is only a cross-sectional study, it is necessary to carry out relevant cohort studies in the future to verify this conclusion.
The use of BN model in this study helps reveal the complex network risk mechanism between the pathogenesis and factors of ASCVD. In addition to the direct relationship between metabolic status and BMI level and ASCVD, dyslipidemia, diabetes, eGFR, and other variables can indirectly affect the risk of ASCVD by mediating the relationship between metabolic status and sex. In terms of data interaction, compared with conventional statistical models, the BN model can further describe the relationship between factors and the impact of interaction on the risk of ASCVD through the network diagram between variables, and does not affect the interpretability of the network. In addition, another important advantage of the BN model is that the complex model is decomposed into multiple sets of refined simple models through Markov blanket theory, making these simple models easier to calculate and analyze.
This study has some limitations. First, although CHNS is a long-term follow-up cohort study, it only uses its 2009 data set, which belongs to cross-sectional data, so the directed arc direction between nodes or variables only represents probability dependence, not causality. Further studies with follow-up cohort data are needed. Second, this study only covers the Chinese population, so the extrapolation and applicability of the conclusions in other ethnic populations must be treated cautiously.
Conclusions
In summary, this study performed a BN to construct a 10-year ASCVD risk model of metabolic obesity phenotype. Meanwhile, the inference results showed that people with MHO classified by the new diagnostic criteria are not at increased risk for ASCVD. In the future, follow-up cohort data will be used to verify the new definition. This study helps identify factors dynamically stabilizing MHO and implement targeted interventions for these factors as early as possible.
Funding
The research was supported by the National Natural Science Foundation of China.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
We thank all the participants in this study and all the collaborators of the research hospital.
Conflict of interest
The authors declare that they have no conflict of interest.