
Abstract
BACKGROUND:
Individuals seem to be differently susceptible to motion-related sickness (motion sickness, visually induced sickness etc.). Investigations of the reasons for these different susceptibilities have revealed many potential factors that could predict individual susceptibility to motion-related sickness.
OBJECTIVE:
This paper attempts to conduct a comprehensive literature review on inter-individual predictors of susceptibility to motion-related sickness using systematic approaches.
METHODS:
After a systematic literature research, titles and abstracts of 1778 publications were screened for relevance. Reference lists of selected publications were searched for additional studies. This procedure yielded 184 relevant publications.
RESULTS:
The identified predictors were clustered into demographic, physiological and psychological aspects. Among these predictors, the factors gender, length of velocity storage and anxiety showed the greatest predictive power. In addition, individual susceptibility to motion-related sickness is also to a large extent dependent on the degree of habituation to the aversive stimulus.
CONCLUSIONS:
Some of the identified influencing factors seem to have different effects on physically and visually induced motion sickness. More research is needed to close gaps, especially on predictive factors of visually induced motion sickness.
Keywords
Introduction
Motion sickness is a well-known syndrome many people experience while traveling by car, train, airplane or being at sea. The condition is experienced as very unpleasant for affected persons who often quickly abandon the situation and seek to avoid it in the future. Among the symptoms that occur in affected persons are nausea, vomiting, dizziness, vertigo, headache, loss of concentration and increased fatigue up to, in extreme cases, complete incapacitation [101, 160].
In recent history, since the emergence of motorized transportation like cars and airplanes, motion sickness in those kinds of vehicles has been acknowledged to be a serious issue [160, 167]. In an early study with data from the 1940 s with a huge sample size of about one million participants, approximately 75 % of all passengers reported symptoms similar to motion sickness when flying in an airplane [121]. This number seems to have decreased since then, probably due to technological development and the habituation of passengers to regular flights with airplanes. However the issue is far from solved. In a study conducted in 2000, 48 % of respondents said they experienced motion sickness symptoms during flights [194]. Given the still high incidence rates in common modes of transportation, motion sickness is a threat to passenger comfort and, if pilots are affected, can pose a significant safety risk.
Pilots are not only at risk within the aircraft, but often complain about motion sickness in full-flight simulators, i.e. flight simulators which, in addition to a visual scenery, try to reproduce the motions of a real aircraft [93, 111]. Interestingly, this simulator sickness occurs more frequently among experienced flight personnel such as instructors who have greater experience of how the real aircraft would move, than among less experienced student pilots [93].
In addition to full-flight simulators, simulator sickness also occurs in fixed-base simulators, i.e. simulators without any motion feedback. This is a first indication that motion-related sickness can also occur in the absence of any physical movement without stimulating the vestibular senses. And indeed, although the vestibular sense of motion sickness is of great importance, especially because it is the primary human sense of motion detection, motion sickness can also be triggered when there is no vestibular stimulation at all, when motion is visually presented but not actually experienced [159]. Numerous experiments on visually induced motion sickness (VIMS), in which participants are usually exposed to an alternating pattern, for example black and white stripes in a so-called optokinetic drum, confirm the assumption that motion sickness can also be induced in the absence of any actual movement. Motion sickness therefore does not necessarily seem to be a consequence of physical movement but instead seems to be a consequence of inadequate integration of different movement stimuli in the central nervous system [108].
While the experiments on VIMS are rather artificial and only slightly reflect conditions of real environments, the development of new technologies in the field of virtual realities (VR) lends new practical relevance to the topic.
VRs are digitally rendered environments which are most often presented with a head mounted display (HMD). Many users of VR complain about problems with the use of VR systems, especially symptoms that are very similar to motion sickness. Cybersickness was suggested as the term for this kind of motion sickness experienced in virtual realities [132]. Due to the relative novelty of the technology and the pace with which new developments are presented, there is a lack of research on the subject in many areas.
In order to subsume all these different types of sickness, in the following the term motion-related sickness is used as a generic term for all types of sickness triggered by any type of motion or visually-presented motion.
Even within the same setting, the same motion vehicle, simulator, or VR system, studies of motion-related sickness typically yield vast differences between individual sickness experiences which cannot be attributed to the utilized stimulus. The causes of these inter-individual differences in susceptibility to motion-related sickness have been subject to many investigations since the 1950 s [e.g. 116]. Nevertheless, a definite explanation of these differences remains undetermined.
The goal of this review is to provide an overview about past research using some systematic approaches, to identify factors which reliably contribute to the explanation of inter-individual differences and to reveal possible factors associated with motion-related sickness that need further clarification.
As many of the included studies used widely different methods (from the type of motion exposure to the outcome measurement), the aggregated parameters reported in the following review will only provide a rough overview and no exact estimate.
Literature research
Searches of electronic databases PubMed and PsycINFO were conducted using the following search term:
begin quote[motion sickness OR cybersickness OR simulator sickness OR visually induced motion sickness OR vr sickness OR gaming sickness] and [personality OR ability OR individual differences OR age OR gender OR gene* OR susceptibility OR anxiety OR neuroticism].end quote
Auto-exploding of both databases was enabled, using thesaurus expressions for all terms included in the query. No date restrictions were set.
The query resulted in 1282 references in the PubMed database and 496 references in PsycINFO. Publication titles and abstracts were pre-screened regarding fit to the subject of this review. Irrelevant publications were excluded. The remaining references were subjected to a detailed full-text screening.
The goal was to identify (stable) individual characteristics that affect motion-related sickness or are empirically related to it. This does not necessarily imply trait-like characteristics (e.g. personality) but assumes reasonable stability across different situations (e.g. habituation or experience) and precludes any characteristic induced by a treatment (e.g. anti-motion sickness drug) or due to context of the situation (e.g. being the driver vs. passenger).
Studies were selected for inclusion in the present review based on multiple criteria. Only studies with original data in English language covering sickness induced by motion-related stimuli were included, i.e. extreme motion, motion vehicles and visually presented motion. This excluded all studies investigating post-operative sickness, chemotherapy-induced sickness and all kinds of sickness without reference to motion-related stimuli. Furthermore all studies using a treatment to alter motion sickness susceptibility were excluded, unless reporting separate results for a control group. This included pharmacological interventions using anti-motion sickness drugs.
Finally, only studies involving human participants were included in the review. This narrows down the available evidence, especially with regard to physiological factors influencing motion-related sickness. However, it prevents a discussion on the generalizability of findings in animal studies to human organisms.
The screening of title, abstract and full-text, applying the inclusion criteria, yielded 127 publications fitting the purpose of this review. All of the selected publications were peer-reviewed journal articles.
Subsequently, the reference lists of all selected publications were searched for relevant papers following the same procedure and inclusion criteria from the original search (“backward snowballing”). After the first iteration of searching the reference lists, this procedure was repeated for the newly selected publications until no novel relevant publication could be identified. This method yielded 57 additional publications. These publications included peer-reviewed journal articles, conference proceedings papers and technical reports, for example from the National Aeronautics and Space Administration (NASA).
The procedure for the selection of publications is outlined in Fig. 1.
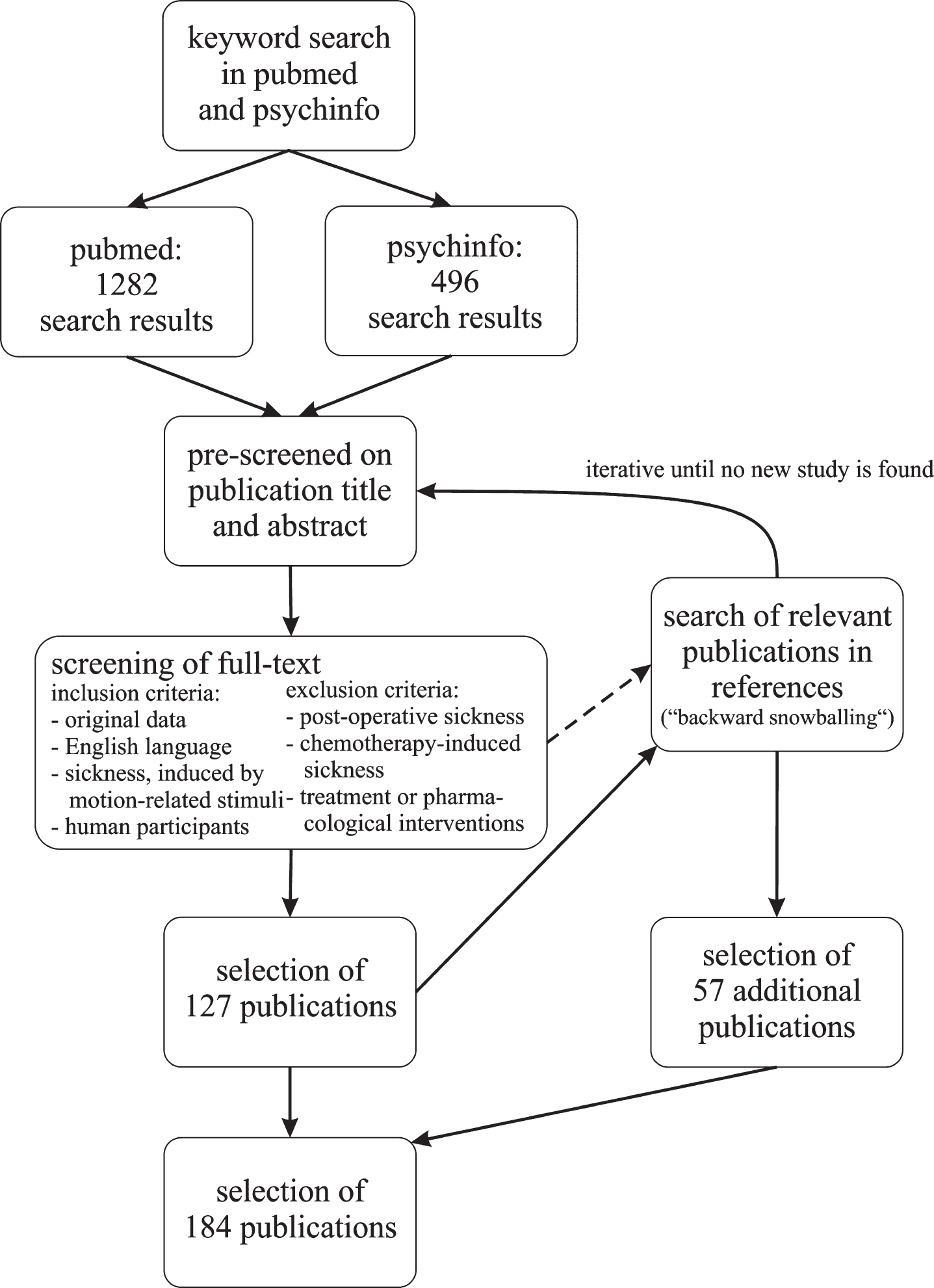
The procedure for the selection of publications.
A total of 184 publications were included in this review. Study characteristics and key findings that appeared relevant were extracted from the full-text and entered into a list. The list of relevant study information eventually included meta-information like title, authors, journal and year of publication as well as the following study characteristics: sample size, sample composition (male only/ female only/ both genders), type of sickness induced, sickness induction method, outcome/sickness measurement, and information on significant and non-significant predictors of sickness analyzed in the study. Table 1 summarizes the study characteristics of the 184 publications.
Characteristics of selected studies (N = 184)
Characteristics of selected studies (N = 184)
Sample sizes covered a large range from 8 to 80,494 participants. The largest sample size by far was used in a study [87] investigating genetic predictors. However, the median sample size was 50 participants. Most studies investigated mixed samples with male and female participants but 25 studies (14 %) only considered one gender. Studies investigating only male participants were mainly conducted with military personnel or seafarers while the female only studies often investigated the effect of the menstrual cycle.
The most frequently assessed type of sickness was motion sickness history (not counting studies in which motion sickness history was used as an independent variable) which is not actually experimentally induced but reported in a survey from past motion sickness occurrences. The different sickness inducing techniques illustrate the abundance of different methodology used in this field of research. Especially for motion sickness, motion stimuli differed quite substantially ranging from a space flight to a boxing fight. These methodological differences largely do not allow meta-analytical methods to be applied.
The variety of methods is also reflected in the list of different sickness measurement tools. Most studies use report questionnaires filled in by the participants or a trained observer. A large number of studies use self-made symptom checklists, self-made sickness history questionnaires, or provide insufficient reference to where they obtained their assessment method. These self-made tools are, however, often similar to the published questionnaires and usually involve an inquiry of nausea, dizziness and headache which are rated on a specified scale. Only few studies used self-determined termination or a clearly defined physiological response such as vomiting as measurement of motion-related sickness.
In the following, the results of the literature review will be presented in more detail.
Demographic aspects
Gender
Gender has been the most investigated predictor with regard to motion-related sickness. Furthermore, differential sickness scores for gender or gender comparisons are given in many publications despite not being the main research question. Thus, gender is probably the predictor least affected by publication bias.
In the set of selected publications, 37 provided gender comparisons. These studies differ considerably in their applied methods of motion-related treatment and outcome measurement. As can be seen in Table 2, about half of the given scores compared gender differences in motion sickness history, asking for past motion sickness incidences in various motion vehicles. The remaining studies reported sickness incidences or symptom scores following an experimental treatment. These treatments themselves differed tremendously in duration and stimulus quality, from motion sickness incidence during approximately 60 hours of initial flight training [128] to cybersickness during an immersion to a virtual reality for up to 15 minutes [143]. Most of these studies used symptom or general sickness severity ratings. Three studies simply used self-determined quitting of the exposure as outcome measurement.
Number of studies reporting significant and non-significant differences and sample size-weighted mean and SD of effect size between genders for motion sickness history, actual symptom ratings and quitting
Number of studies reporting significant and non-significant differences and sample size-weighted mean and SD of effect size between genders for motion sickness history, actual symptom ratings and quitting
Seven of the included publications provided comparisons for both motion sickness history and sickness ratings following an experimental exposure.
Table 2 shows that 17 of 18 comparisons found significantly higher motion sickness history scores for women when asked in a survey for motion sickness history. There is only one study indicating higher motion sickness history for women [201] which did not provide descriptive or test statistics on the comparison but solely reported a non-significant difference.
Besides motion sickness history, only six of 22 studies found significant differences in symptom severity scores following the exposure to an experimental sickness-inducing stimulus. Three (of three) studies reported significant gender differences in the rate of quitting a motion exposure due to sickness symptoms.
In order to more closely investigate the evidence, analyses of the effect sizes for the differences of male and female participants were performed. Twenty seven effect sizes could be extracted from the publication sample. Sixteen studies did not provide enough information to compute effect sizes. Figure 2 Fig. 4 present an overview about the effect sizes separated for motion sickness history (Fig. 2), (actual) sickness severity (Fig. 3) and quitting (Fig. 4). For studies reporting mean and standard deviations of scores, t-tests or F-tests, Cohen’s d was computed. However, for studies using a χ²-test, Hedges g was used.
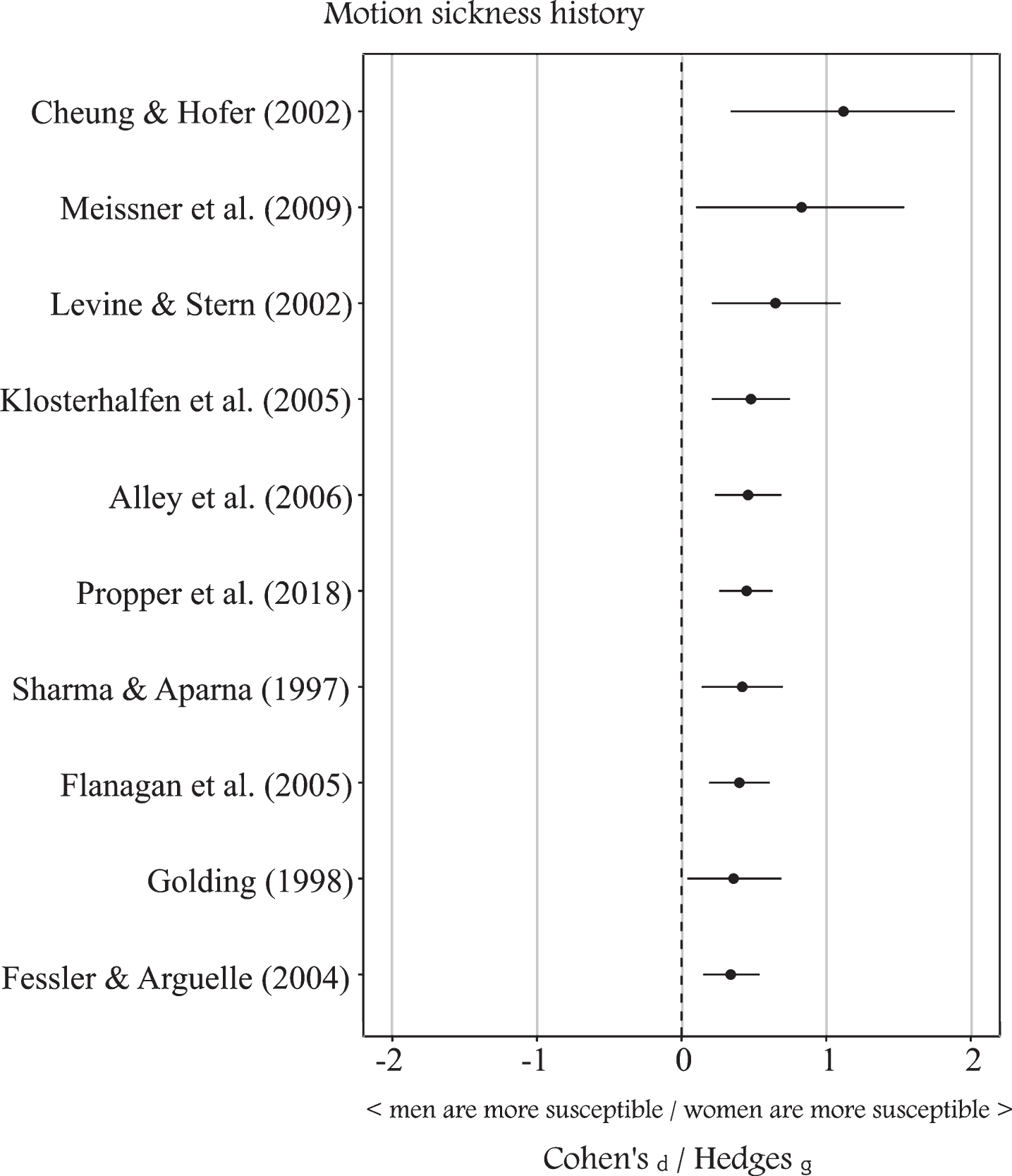
Gender effect on motion sickness history. Effect sizes with 95% confidence intervals.
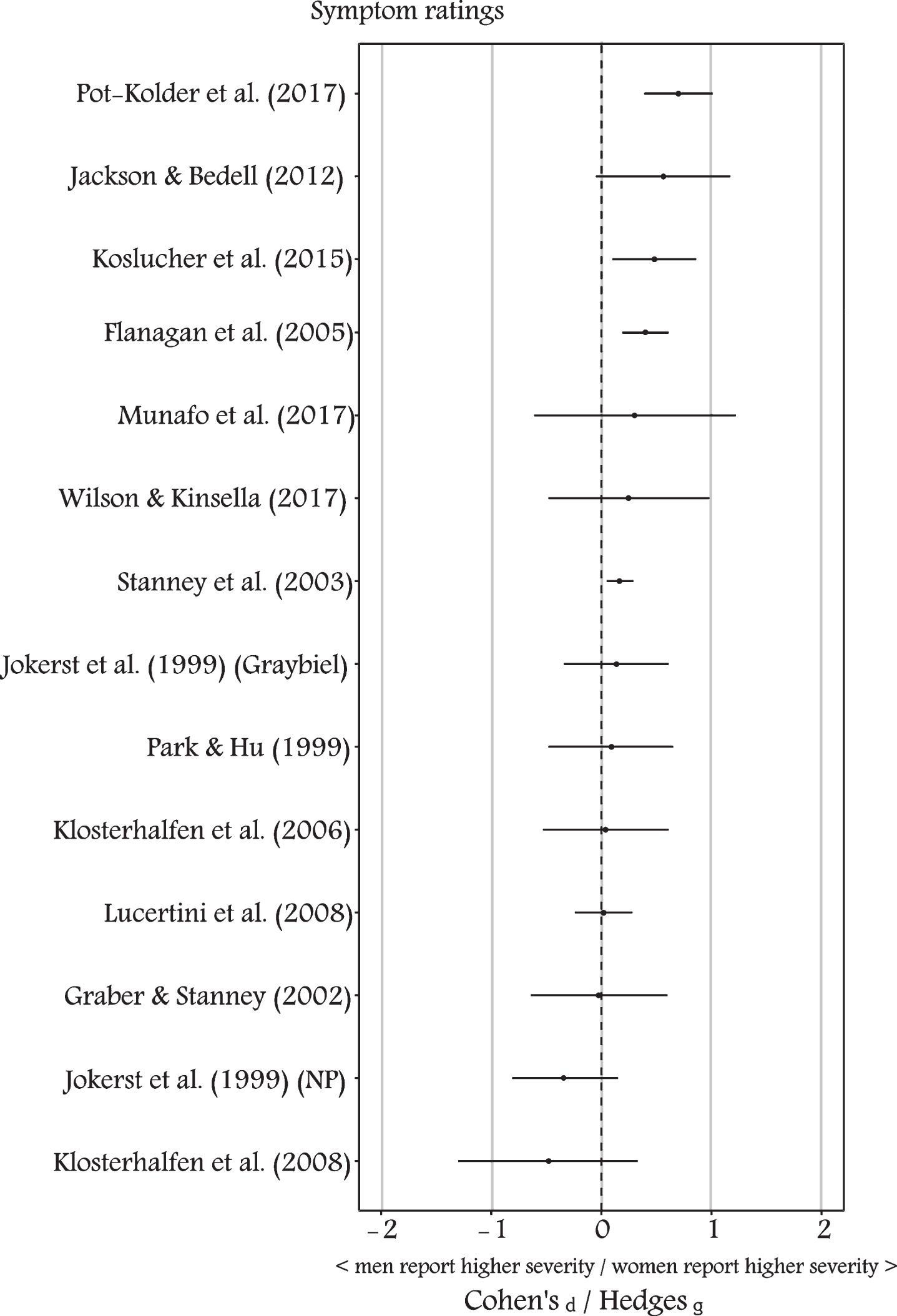
Gender effect on symptom severity ratings. Effect sizes with 95% confidence intervals.
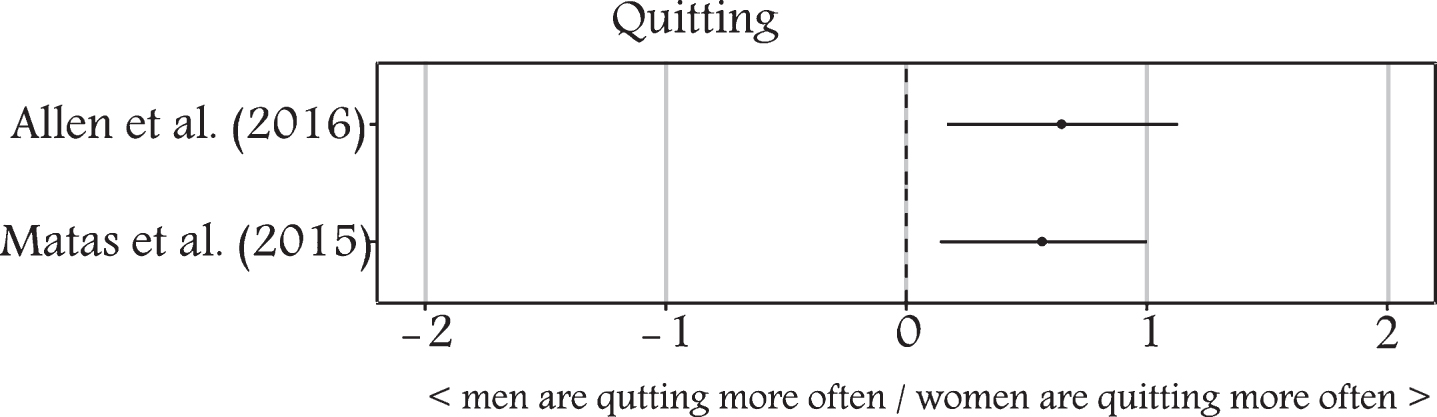
Gender effect on quitting a motion exposure.
Analyses of the mean of effect sizes, weighted by sample size, yielded an average effect size of 0.35 (CI: 0.26 – 0.43).
Due to the differences in the number of significant results indicated for motion sickness history and symptom severity, separate analyses for the different types of outcome measurements were performed. The results can be seen in Table 2. While the average weighted effect size for motion sickness history was at 0.46 (CI: 0.37 – 0.54), the average effect size for actual severity ratings was considerably lower (weighted mean: 0.22; CI: 0.07 – 0.36) and highest for quitting (weighted mean: 0.61; CI: 0.53 – 0.68). The analysis of quitting, however, was only based on two studies. It must be noted that the weighted effect size does neither include the quality of the study nor publication bias.
The analyses indicate a stronger gender difference in motion sickness history than in sickness severity ratings when exposed to an actual motion-related stimulus. These findings have already been reported in the literature, especially those publications reporting both differences for susceptibility and severity ratings [e.g. 106].
A greater susceptibility of women to motion-related sickness has often been explained with hormonal changes during the menstrual cycle. Six studies have investigated the role of the menstrual cycle in the genesis of sickness to motion-related stimuli. While two did not find a cyclical alteration of sickness susceptibility [32, 64] four of them found a significant effect.
Of these, three studies reported increased sickness symptoms during menstrual and peri-menstrual phases [67, 131] while one study found the opposite and observed stronger symptom severity during ovulation [37]. In addition, one study [131] failed to determine a fluctuation of sickness susceptibility during the menstrual cycle for women who took oral contraceptives at the time of the experiment and were thus regulating their hormone balance. The influence of the menstrual cycle on sickness susceptibility was suggested to be caused by fluctuating estrogen levels [37, 131]. Women near their ovulation tend to be more sensitive to auditory, olfactory and visual stimuli and may therefore be more sensitive to sensory mismatch. Moreover, high estrogen levels can increase the number of dopamine receptors which are usually inhibited by some effective anti-emetic drugs [13]. However, instead of the absolute estrogen level which is highest during ovulation, it was suggested that changes in estrogen concentration before and at the end of the menstruation sensitize chemoreceptive trigger zones [13].
Besides fluctuations during the menstrual cycle, another explanation has been presented in anthropometric differences between males and females, e.g. differences in height or center of body mass. Differences in certain anthropometric properties can yield differences in the ability to maintain postural stability when being exposed to motion-related stimuli which in turn might lead to increased sensations of motion sickness [178]. Few studies have been carried out investigating anthropometric differences with sickness symptoms. It was found that increased VIMS was associated with shorter foot length and smaller height (when controlling for gender, weight, and/or body mass index), both characteristics more prevalent in women [112]. Furthermore, one study [181] found a weak but significant correlation (r = 0.07) of the body mass index, but only with oculomotor symptoms of sickness and not with nausea or disorientation.
A hypothetical evolutionary adaption was suggested as a reason why women should be more susceptible to motion-related sickness [66]. According to that hypothesis, higher sensitivity to nausea-inducing stimuli gives an advantage in protecting a fetus from dangerous toxins. However, this has not yet been empirically investigated.
Despite all these explanations, the results indicate a stronger gender difference when asking for past occurrences of motion sickness than when assessing symptom severity after actual exposure to an adverse stimulus, suggesting at least a partial contribution of response bias when asking with a survey.
Some authors similarly expressed the hypothesis of a gender-dependent response bias. Perhaps females have the tendency to more readily admit the incidence of motion sickness or are generally more inclined to report physical discomfort [33, 61]. Admitting sickness might be part of a diverging socialization and might ultimately be more socially accepted for women than for men [61, 106].
However, a similar effect should be observable in reports of symptoms. It is questionable why men withhold reports of past motion sickness incidences but readily admit symptoms in an experimental setup. Furthermore, the experimenter’s gender was not found to influence the symptom ratings of the participants which would be expected if responses are biased by the social acceptance [95]. In another study, gender differences were also found in some but not in all kinds of vehicles in reports of motion sickness history [49]. If there is a general tendency towards less admitting sickness occurrences, males should have indicated less sickness across all vehicles.
Another explanation could be the different assessment approaches in motion sickness history and actual sickness severity. Surveys for sickness history usually ask for the incidence of motion sickness in a dichotomous “yes” or “no” format and the frequency of these occurrences. Assessments of sickness after actual exposure to motion-related stimuli typically ask for sickness severity on a continuous scale. Women might associate lower ratings on the sickness scale with the classification of severe sickness than men do. Moreover, women might have a lower threshold of symptom severity above which they indicate a motion sickness incident [61].
Finally, it was suggested that gender differences may be related to the nature of the given stimulus [112]. The authors proposed that women are more susceptible to sickness when exposed to linear oscillation in contrast with facing rotational motion. This is in line with the observation that gender differences in response to actual motion exposure are predominantly found in commercial transportation [33] which often involve more linear (e.g. heave of a ship) than angular movement.
In summary, the majority of studies found an effect, suggesting an influence of gender on motion-related sickness. However, future studies should determine the exact extent of response bias in gender-related differences and why this effect may be different between the report of past occurrences of motion sickness and the report of actual motion sickness severity.
Unlike gender, relationships between age and motion-related sickness were less often reported. Only sixteen studies in the current sample of publications provided correlations with age or comparisons of different age groups. Since many studies were carried out using student, flight school or military participants, studies often used samples homogenous in terms of age. In those cases, a comparison of different age groups is neither possible nor useful. In order to determine age-related effects, large ranges of age, preferably from childhood to seniors, needs to be used.
Table 3 shows a summary of the studies investigating age effects on motion-related sickness in terms of sickness increasing or decreasing with age or having no effect. A fourth option is a relationship of age and sickness, however, in a complex, non-linear manner. As previous studies suggested differences in the effect of age depending on the type of sickness, i.e. the type of motion stimulus [5], the descriptive statistics were further divided into physical motion induced sickness (motion sickness/ motion sickness history) and visually induced sickness (simulator sickness/ VIMS/ cybersickness).
Number of studies reporting an increase or decrease of sickness, a complex (e.g. non-linear) relationship or no relationship with age, separately for motion induced and visually induced sickness
Number of studies reporting an increase or decrease of sickness, a complex (e.g. non-linear) relationship or no relationship with age, separately for motion induced and visually induced sickness
Unfortunately, many studies did not provide sufficient information to perform a detailed analysis of effect sizes. However, the available data suggests for visually induced types of sickness, susceptibility tends to increase with age and in contrast to motion sickness [5, 22], no study found a decrease of sickness severity with age. Three studies did not find a relationship between age and sickness severity in visually induced sickness [97, 151].
For motion sickness, older participants tended to experience less sickness than younger participants in four of eight studies. It must be noted that all studies (with one exception) observing linear relationships between age and sickness were using adult samples. The two studies observing a complex pattern [18, 173] also included younger children. Children below the age of two were reported to be practically immune against any kind of motion sickness [173]. A different study did not observe any motion sickness below the age of five with the youngest participants being four years old [18]. In both studies, young children have been assisted by those responsible for them in filling in the survey. It remains questionable, whether surveys of children of that age are yielding reliable data.
After the age of five, a sharp increase of motion sickness severity with somewhat different progression for males and females was found [18]. While females were reported having higher amplitude of susceptibility and peaking earlier at the age of 11, men were not having their highest motion sickness susceptibility until the age of 21. After their peak, susceptibility gradually decreased for both men and women [18].
This is in line with all the studies finding a trend of decreasing motion sickness scores for older participants, given that these studies only had adult participants.
The studies on age were fairly consistent and some had large samples like the above mentioned study [18] who investigated 2840 individual surveys. However, the question remains why age should have an impact on sickness susceptibility and why motion induced sickness and visually induced sickness putatively differ in their relationship to age.
Aging is accompanied by loss in visual and vestibular functioning which could desensitize older individuals to sensory conflict responsible for inducing sickness. This hypothesis might explain the decrease of motion sickness with increasing age but does not explain and even stands in contrast to the elevated susceptibility of older participants to sickness induced by visually presented motion.
Older participants were less susceptible to in-flight motion sickness than younger participants in parabolic flight while also showing a significant correlation with the amount of experience with parabolic flights [68]. The authors concluded that relationships of age and motion sickness were most likely caused by the habituation of repeated exposures [68].
Similarly, many studies used commercial transportation like coach busses [193] or cruise ships [18] as motion inducing stimuli or were assessing motion sickness history with the frequency of motion sickness incidences in different common motion vehicles such as cars, ships and airplanes [49, 173]. This might suggest that the observed effect of age might be a mere effect of habituation due to more frequent exposure to these common motion vehicles.
Habituation is also a possible explanation for the inverted relationship of age and sickness with visually presented motion, at least for cybersickness. Computers, video games and virtual environments still enjoy greater popularity among younger people. Many young people are playing video games regularly or are using digital devices in their leisure time. Since many simulators or VR applications share many characteristics, playing video games or using a computer in general could provide a similar habituation for visually induced sickness as motion vehicles for motion sickness. This hypothesis can also be used to explain the gender differences discussed above as males usually play more video games than females.
Visually-induced motion sickness using an optokinetic drum is a stimulus, relatively uncommon in everyday life. In accordance with the previously presented rationale, the only study using VIMS to investigate a relationship with age yielded no significant association [88].
Although age seems to provide a good prediction of the susceptibility to both motion sickness and cybersickness, it remains questionable whether there is a causal connection or whether the connection is meditated by different degrees of habituation.
As has been mentioned in the previous section, habituation was proposed to occur after repeated exposures to an adverse motion stimulus and ameliorate motion-related sickness symptoms. Habituation is not a trait as it can be achieved by practically anyone. Only 1 % to 3 % of the population are assumed to never habituate to motion sickness [86]. However, habituation can be a relatively stable individual characteristic in the form of experience. Individuals who engage repeatedly with a certain motion-related stimulus, motion vehicle or virtual environment are familiar with the effects of these stimuli on the vestibular and visual systems and might habituate or adapt in order to reduce sickness symptoms.
For motion sickness, experience with coach travel [193], parabolic flight [68] or seafaring [28, 189] was associated with decreased susceptibility to motion sickness in the respective motion vehicle. Not only has repeated experience in the past reduced the risk of future motion sickness at sea [28], prolonged duration at sea also reduced the symptom severity [74, 189].
In a laboratory setting, one study [48] observed an increased tolerance to a rotating chair and an optokinetic drum when previously adapted with the same device in comparison with a control group. Two different studies [84, 86]were similarly able to show a decrease in symptom severity after repeated exposure to a virtual environment across multiple days.
The majority of studies indicated an ameliorating effect of habituation or adaption on symptom severity in motion sickness and cybersickness. Two further questions in relation to habituation gained increased attention: the first one concerns the interval between repeated exposures and the second the generalizability of habituation to other devices or even different types of motion-related sickness.
It was suggested that adaption occurs with an inter-exposure interval of two days but does not occur when the time period between exposures is 4 days or longer [184]. In contrast, one study [86] investigated the rate of adaption for different inter-exposure intervals ranging from one day to seven days and found no difference between intervals concluding that the total number of exposures is more important than the inter-exposure interval. However, there is yet not sufficient research on inter-exposure intervals, especially to determine long-term adaption effects over the time course of months or years. For very short-term intervals, habituation does not seem to apply. Two studies did not find a reduction of sickness severity with an inter-exposure interval of 15 to 30 minutes, suggesting that it needs at least a couple of hours for the habituation to take an effect [50, 204].
Most studies investigated the effect of habituation with the same stimulus with which the habituation was performed. Repeated exposure to a rotating chair was found to decrease symptoms in the rotating chair and in an optokinetic drum as well [48]. However, participants who were adapted with the optokinetic drum only habituated to the drum and not to the rotating chair. The authors explained these differences with the higher relative motion sickness induction of the rotating chair. Two studies showed evidence that video gamers (operationalized with the amount of common video game play without HMD) might be less prone to experience cybersickness in virtual environments presented with an HMD [141, 165]. Video games possibly provide habituation to digitally presented virtual stimuli reducing cybersickness susceptibility in the more provocative environment of an HMD exposure.
An interesting finding indicated that experienced pilots reported more sickness in a flight simulator that fits the type of aircraft they are licensed on than more inexperienced pilots [21]. Experienced pilots may be more sensitive to subtle differences between the motion behaviors of the simulator to the real-world aircraft and thus experience more sensory conflict.
Although there is insufficient evidence of generalizability of adaption to motion-related stimuli across device and type of sickness, the rate of adaption, i.e. the time someone needs to be adapted to an adverse stimulus, seems to be fairly stable across multiple motion-related devices [76].
Handedness
Handedness has been investigated in relation to motion sickness in two studies in the publication set. Both studies used motion sickness history surveys as outcome measurement. Handedness was investigated because it was suggested to reflect possible individual differences in brain lateralization [140]. For example, non-right handers are thought to have an altered cortical lateralization of vestibular function [6] and decreased motion detection functioning [163].
A slightly higher relative proportion of non-right handers was found in the motion sickness resistant group [140]. However, they also found a similar increase of relative proportion in the extremely susceptible group. In a comparison between right-handers who are consistently using their right hand for various tasks and inconsistent-handers who preferred to use different hands for different kinds of tasks, neither group showed a significant difference in motion sickness susceptibility, neither in childhood nor in adulthood [154].
Based on the two studies, it seems unlikely that handedness is a reliable predictor of motion sickness susceptibility.
Other demographic factors
Other demographic variables investigated in relation to motion-related sickness include the body mass index (BMI) and alcohol abuse.
One study investigated the BMI in context of gender differences and did not observe a relationship of BMI but found a significant correlation of height with motion sickness history when controlling for BMI [112]. In a different study, a significant correlation of BMI and oculomotor disturbances with less symptoms for more overweight participants was reported [181]. However, the effect size was small (r = –0.07) and no associations with other symptoms of cybersickness were discovered. Thus, the effect of BMI and overall anthropometric constitution on sickness susceptibility seems limited.
There was only one study in the publication set investigating the relationship of alcohol consumption and motion sickness history [123]. The authors did not find a relationship between frequency of alcohol consumption and motion sickness but reported significant correlations of motion sickness history with relative frequency and overall severity of hangover after alcohol consumption.
Physiological aspects
Vestibular functioning
General functioning of the vestibular system and asymmetries in effectiveness of labyrinthine functioning in left and right ears are often considered to contribute to individual differences in motion sickness susceptibility.
Different tests are used in the motion sickness literature to determine the general functioning of the vestibular system and asymmetries of functioning between the left and right ear. These tests make use of different characteristics of the vestibular system: the vestibulo-ocular reflex (VOR), the caloric nystagmus and the vestibular evoked myogenic potentials (VEMP).
The first studies from the 1960 s compared the incidence of motion sickness in patients with vestibulopathy and healthy individuals during parabolic flight [99] and at sea [100]. In both studies, patients with vestibulopathy (with a loss of vestibular functioning) did not show any signs of motion sickness while the majority of healthy participants showed severe sickness symptoms. Therefore it was concluded that patients with vestibulopathy are practically immune to motion sickness and that vestibular functioning plays the key role in explaining differences in motion sickness susceptibility. In a different study, the resistance of patients with vestibulopathy to motion sickness was replicated in a laboratory setting with a rotating chair. However, patients with vestibulopathy were not completely immune but showed significantly decreased levels of sickness compared to healthy controls [144]. This could be attributed to residual vestibular functioning in the patients with vestibulopathy who participated in the study.
As patients with vestibulopathy did not experience any or at least very low motion sickness, differential functioning of the vestibular system was considered as source of individual susceptibility in non-pathological participants as well.
Eleven studies in the publication set investigated vestibular functioning with VOR. VOR was assessed prior to the sickness inducing stimulus and in some cases during the exposure to assess the effects of habituation.
The best predictor across all VOR parameters was the time constant. Six studies identified a significant relationship between the VOR time constant and measurements of motion sickness [36, 155]. The effects found were medium [η² = 0.20; 36] to large [r = 0.59; 155]. The time constant strongly depends on the integration of velocity information in the central vestibular system, the velocity storage. It seems as if more susceptible individuals have a more effective velocity storage and thus a prolonged time constant [155]. This assumption is supported by the fact that patients with vestibulopathy not experiencing any motion sickness symptoms also had a reduced time constant [43]. Furthermore, as described above, motion sickness symptoms usually decrease with habituation. The VOR time constant similarly decreases during extended exposure to a sickness inducing stimulus (e.g. at sea) and enhanced habituation [36, 176].
Another parameter considered for predicting individual differences in motion sickness susceptibility is VOR gain. Two studies found gain to be related to motion sickness with higher gain for more susceptible individuals [74, 176] while three studies reported insignificant relationships [36, 155]. The authors of those studies finding associations of VOR gains and motion sickness argued that the increased VOR gain indicates that motion sickness susceptible individuals have generally more intense vestibular responses [74]. An interaction of time constant and eye velocity (i.e. gain) on the susceptibility of motion sickness was proposed [195].
Besides VOR, which primarily assesses functioning of the semicircular canals, VEMP are used to determine functioning of the otolithic organs. Five studies have investigated VEMP in relationship to motion sickness. All five studies used cervical VEMP (cVEMP) while only one study additionally investigated the relationship with ocular VEMP (oVEMP). Three studies report a higher VEMP threshold [177, 190], two studies observed higher asymmetry ratios [62, 177] and one study reported higher cVEMP amplitudes for susceptible individuals [62]. One study did not find any relationship of cVEMP parameters or canal paresis from a caloric test with motion sickness history [23]. Only one study provided an investigation of both cVEMP and oVEMP and reported the same results for both, an increased threshold and asymmetry ratio in motion sickness susceptible participants [177].
Lower VEMP thresholds have been suggested to indicate a broader dynamic range of the vestibular system facilitating adaptive modifications to maintain postural stability and enhance habituation to unusual motion conditions [189].
The findings of higher asymmetry ratios being related to motion sickness [62, 177] match previous results of increased torsional asymmetries in astronauts more susceptible to space motion sickness [45, 46] and stronger asymmetries in ocular counterrolling to left and rightward tilts [119]. It is suggested that asymmetric otolithic functioning is well compensated during normal motion conditions. However, under extreme or unfamiliar motion conditions, this compensation fails, leading to a sensory conflict which in turn produces motion sickness [177]. Despite the evidence, the authors acknowledged that otolith asymmetry is only one and might not be the main causative factor in motion sickness susceptibility [119].
As mentioned earlier, only one study investigated the relationship of the previously described measurement methods with sickness induced solely by visual stimuli. In contrast to the findings for motion sickness, the authors of one study [94] were able to induce VIMS in patients with unilateral and bilateral vestibulopathy. Due to the low number of patients with bilateral vestibulopathy in this study, it is unclear whether these patients are as susceptible to VIMS as healthy individuals. The fact that severe VIMS could have been induced in these patients shows, however, that the vestibular system plays a different, probably much smaller role in the genesis of visually-induced motion sickness including cybersickness.
More research has to be conducted to determine the exact relationship of the functioning of the vestibular system and VIMS/cybersickness. For motion sickness, a relationship of general sensitivity of the vestibular system and/or the asymmetry of functioning is likely. However, the inconsistent results demonstrate that this relationship is only one of several factors of motion sickness.
Visual aspects
The first attempt to link ocular aspects to the sensation of motion sickness was conducted by James Reason using the spiral after-effect (SAE) [157, 158]. For this type of measurement participants are instructed to fixate a point in the middle of a constantly rotating spiral disc. After terminating the rotation of the disc, many participants experience a persisting movement, the SAE. The time until the participant indicates that the SAE has vanished is recorded with a stopwatch.
Reason found that the SAE was related to individual motion sickness history (r = 0.43 in [157] and r = 0.42 in [158]). Furthermore, he observed the SAE to be correlated with a labyrinthine after-sensation which was similarly assessed with a rotating chair and self-reported persistence of any after-sensations. Based on these findings, he proposed his ‘receptivity’ hypothesis in which he suggested that individual susceptibility would differ in association with general receptivity to sensory input. In this theory, he linked the sensitivity to visual or vestibular stimulation to personality constructs like extraversion-introversion [157, 158].
However, two subsequent studies on the SAE could not reproduce the high correlations with motion sickness history and reported non-significant correlations of r = 0.21 [41] and r = 0.09 [98].
In a sense, the SAE is very similar to the optokinetic after-nystagmus which will be introduced below. However, unlike the optokinetic after-nystagmus, the SAE relies on self-report and thus on the subjective experience of the participants. The persistence was measured with a stopwatch, another source of possible unrealiability, to the nearest 0.5 second which is a rather coarse temporal resolution.
As a more objective measurement and similar to the vestibulo-ocular nystagmus used for the prediction of motion sickness, the optokinetic nystagmus (OKN) was investigated in relation to motion-related sickness and especially with regards to VIMS and cybersickness. In contrast to the vestibulo-ocular nystagmus which is induced by vestibular stimulation utilizing the VOR, the OKN is the result of visual stimulation. Theoretically, OKN can be induced by any kind of constant angular visual stimulation such as a VR scenery. In practice, OKN are usually triggered by optokinetic drums similar to those used for inducing VIMS.
The OKN resembles the nystagmus induced by vestibular stimulation. It was shown that the slow phase velocity of the OKN is related to motion sickness history of seafarers suggesting a possible interplay of vestibular and visual systems in the mediation of motion sickness [98].
More recently, the OKN was investigated in relation to VIMS. The parameter of interest was the time constant in form of the optokinetic after-nystagmus (OKAN). OKAN can be assessed when abruptly ending the visual drum stimulation (e.g. by switching off the light). The nystagmus induced during visual stimulation usually upholds for some time after ending the stimulation. OKAN is analogous to the VOR time constant, the time until the slow phase velocity decays to 37 % (1/e) of the peak velocity during visual stimulation.
Two studies investigated the relationship of OKAN and VIMS [78, 79] and found significant relationships between OKAN and nausea [ρ= 0.48; 79] and OKAN and total sickness [r = 0.51; 78]. The authors argued that the velocity storage mechanism, which was also supposed to affect the VOR time constant, stores information during OKN and discharges them after termination of the visual stimulation. The duration of the OKAN would reflect the amount of stored information which in turn seems to be related to the individual susceptibility to VIMS [78].
OKAN is a promising approach to predict the susceptibility to visually induced sickness (including VIMS, cybersickness and to some extent simulator sickness) using the sensory afferents involved in the genesis of the syndrome. The findings are especially intriguing in light of evidence that VIMS can be induced in patients with bilateral vestibulopathy [94] and thereby limiting the importance of the vestibular system for VIMS.
Taking together the findings for the vestibular system (especially VOR) and OKAN, it is possible that the velocity storage is in fact the key mechanism in the genesis of motion-related sickness. The velocity storage is a process of multisensory integration of different motion cues from the vestibular and visual systems and gains significance only in those situations in which either vestibular or visual signals are missing (or are highly incongruent), hence those situations in which motion-related sickness generally occurs. The time constant of velocity storage seems to be lengthened to a practical relevance only in those situations [120]. It is possible that the time constant can be increased either by vestibular cues in absence of visual cues or vice versa and thus can be triggered by either one of these two systems. This could explain why patients with vestibulopathy are immune to motion sickness elicited by vestibular stimulation but can experience VIMS induced by visual stimulation.
Concerning other ocular aspects, two studies investigated the influence of vision acuity on cybersickness. Both studies were not able to show a relationship between cybersickness scores and stationary 3D vision acuity [2] or stereo vision acuity [80]. However, one study [2] found participants with greater sensitivity to moving visual cues reporting higher sickness scores and aborting the VR at a higher rate. The authors argued that greater sensory ability in the form of better 3D vision enables the participants to more easily recognize visual motion cues incongruent to the vestibular reality and experience more discomfort as a result. So far, this study is the only publication on this relationship. Further research should determine if this relationship can be replicated.
One study [88] investigated differences in vertical phoria in relation to VIMS. Heterophoria (= misalignment of both eyes) can usually only be observed when both eyes are dissociated and single vision is prohibited, for instance by covering one eye. In this study, the vertical deviation of both eyes resting positions correlated to VIMS ratings resulting from an optokinetic drum exposure. According to the authors, sickness could be caused either by fatigue resulting from constantly aligning both eyes to single vision or reduced postural stability of participants with greater vertical phoria. However, it is also possible that vertical heterophoria itself is not causing higher sickness susceptibility but is merely a symptom of otolith asymmetry which could, as described above, also be related to motion-related sickness.
Postural instability
One area that has often been studied in connection with motion-related sickness and is related to both vestibular and visual function is postural instability. Studies in this area were inspired by the postural instability theory of motion sickness, stating that motion sickness is triggered by a prolonged loss of postural stability. The theory also emphasizes that postural instability is not the result but the reason for motion sickness genesis [162].
In studies concerning postural instability, body movements were usually detected by optical or electromagnetic sensors attached to the abdomen or head or by means of a force platform. Parameters commonly used to study postural instability include postural variability (standard deviation), velocity of sway, range of sway and the alpha parameter of a detrended fluctuation analysis which determines the self-affinity of a signal.
Several studies [e.g. 115, 178] have shown that people who are exposed to an adverse movement stimulus sway more and exhibit greater variability in postural control before they report experiencing motion sickness. In the context of this review, the question arises whether postural stability without being exposed to a motion stimulus can also predict motion-related sickness in a motion environment. Or in other words: do people who later experience motion-related sickness have higher postural instability even before exposure? Twenty-one studies have investigated this question in the current publication set.
Seven studies found a significant difference in spontaneous sway between those who felt motion-related sickness and those who remained well, in the sense that sick participants showed greater postural instability [30, 203]. Six studies could not detect any difference [17, 188]. The studies mentioned above dealt with motion sickness, VIMS, cybersickness and simulator sickness and showed no specific effect for one of the mentioned sickness types.
Many studies found inconsistent results with interaction effects and more complex movement pattern differences between well and sick participants. These results could be the subject of a review of their own and shall only be presented here in brief.
Some studies found significant relationships between postural instability and motion-related sickness, but only for part of the sample or only under certain conditions and observed no or opposite results for the rest. Interaction effects were determined with the gender [113], stance width [31] and the axis in which sway was measured [197]. One study [29] reported that participants who got sick in a car simulation showed less postural variability than well participants if they were the driver and more if they were not the driver.
The inconsistent results indicate that a linear relationship of standard parameters (postural variability, speed), measured during spontaneous sway, with symptoms of motion-related sickness cannot be found reliably. Other studies followed the approach that it is not generally the postural instability during spontaneous sway that distinguishes people getting sick and those who do not, but the strategy with which postural balance is established.
In two studies, participants who became sick achieved a higher ratio of lateral to pivotal head movements, suggesting that well participants are better at stabilizing their head [169, 170].
An in-depth study [118] examined the power spectrum of sway in the anterioposterior axis and found a greater proportion of high-frequency components in people with a high motion sickness history, as well as a greater proportion of low-frequency components in sick participants who were exposed to visual motion stimuli. Because sway in a specific frequency range is associated with postural control by a particular sensory system, the authors concluded that people with a low motion sickness history tend to regulate posture by using visuovestibular signals. With the actually induced VIMS, the correlations were exactly the other way around. In contrast to the motion sickness history, it has been suggested that people who have become sick make more use of visual stimuli in the regulation of postural balance.
This obvious contradiction is explained by possible differences in the questionnaires used in the collection of motion sickness history and actual symptoms or differences in the types of motion stimuli needed to induce motion sickness (actual motion) and VIMS (visual motion).
Some of these results coincided with previous studies [203] but some did not [171]. People who did proprioceptive physical sports (e.g. gymnastics, skiing or archery) for a long time were found to be less susceptible to motion sickness which could be caused by a learned regulation of posture with proprioceptive and less reliance on visuovestibular signals [25].
Postural stability has a strong theoretical foundation for explaining motion sickness [162]. However, postural stability in spontaneous sway in the absence of motion stimuli, i.e. general postural stability, seems to be an unreliable predictor for individual differences in the experience of motion-related sickness. Strategy differences in the regulation of postural balance with the analysis of sway frequency bands offer a new possibility to elucidate individual susceptibility to motion-related sickness. Still, these results differ in some analyses without these differences being sufficiently theoretically explainable, yet.
Migraine
One common disorder mentioned in the context of vestibular disturbances and motion sickness is migraine. Migraine is usually associated with unilateral headache with or without additional neurological symptoms (aura). However, many migraine patients also suffer from vertigo, other vestibular disturbances and nausea. Fourteen publications in the publication set investigated the relationship between migraine (or associated disorders) and sickness symptom ratings or general motion sickness history.
Earlier studies comparing migraine patients and healthy controls found higher susceptibility to motion sickness assessed by self-report questionnaire for adults [65, 173] and children [9] with migraine.
One study [77] investigated motion sickness of participants of a yacht race over a period of nine months and found a higher incidence of motion sickness for those indicating experience with migraine prior to the race. Importantly, motion sickness and headache did not occur together. Thus, motion sickness was not a mere symptom of a migraine attack.
When investigating migraine patients within an optokinetic drum eliciting VIMS, migraine patients did show significantly elevated general sickness ratings but only higher scores on the nausea and dizziness sub-scores [52]. Similarly, migraine patients only indicated a higher incidence of motion sickness in some but not all motion vehicles (e.g. cars and buses but not trains) in comparison to controls [53].
Since the mid-2000 s, research on the topic made a distinction between regular forms of migraine and vestibular migraine (VM). In contrast to migraine, the main symptoms of VM are dizziness and nausea which are not necessarily accompanied by headache. The distinction between VM and regular migraine (or other migraine variants) yielded promising results: most of the studies investigating VM patients observed significantly higher sickness history scores for VM patients in comparison with healthy controls and regular migraine patients [16, 198]. Only one study did not find significant differences between VM and regular migraine patients, neither in motion sickness history nor in actual symptom ratings following rotating chair exposure [144].
Two studies additionally investigated the relationship of motion sickness history and Menière’s disease (MD). MD is very similar to VM and difficult to distinguish. Both studies observed drastically elevated susceptibilities to motion sickness for MD patients [69, 175]. The increase in motion sickness susceptibility from childhood (before the onset of the disease) to the time of assessment was in fact the best predictor for an MD diagnosis in adulthood [69].
Generally, most studies agreed on the following pattern for motion sickness susceptibility: general population <migraine <vestibular migraine/ Menière’s disease.
There have been several attempts to explain the relationship between migraine and motion-related sickness. Most of them argue that migraine is accompanied by visual (e.g. impaired motion perception) and vestibular (e.g. impeded balance and vertigo) dysfunctions which increases the sensory conflict during unusual movements and thus leads to increased motion sickness [53, 69]. Another tentative explanation states that both motion sickness and migraine are associated with serotonergic deficits. This hypothesis was supported by findings of migraine symptoms augmented by decreased serotonin synthesis and reduced VIMS for healthy and migraneous participants after consuming a drink with L-tryptophan which is a serotonin precursor [54].
Although the exact mechanisms underlying the association need further clarification, the relationship between migraine (especially VM) and motion-related sickness is well established.
Fitness and sympathetic activity
Aerobic fitness is related to the amount of physical exercise an individual is carrying out. More frequent physical exercises lead to an increase of VO2max, the maximum oxygen uptake which is often used as a measurement of aerobic fitness. High VO2max is important for endurance during prolonged exercise and is often considered as a sign of good health. Five studies investigated motion sickness and aerobic fitness and assessed or validated aerobic fitness with VO2max. All of these studies used an exposure and reports of actual motion sickness as indicator of susceptibility.
Three studies found a positive relationship of aerobic fitness and motion sickness scores [8, 156], in the sense that participants with greater aerobic fitness showed more motion sickness symptoms during exposure to a rotating chair. While two studies used cross-sectional analyses, the authors of the third study [34] administered an 8-week aerobic fitness program and longitudinal data with three rotating chair exposures prior and three exposures after the fitness program. Successful training was validated by increases in VO2max in all participants. Despite a certain degree of habituation to the rotating chair that is common with a longitudinal design, all participants had an increase of motion sickness ratings accompanying the elevated aerobic fitness.
It is yet undetermined why aerobic fitness correlates with motion sickness susceptibility. An increase in aerobic fitness is characterized by adaptive cardiovascular and metabolic adaptions of the body which could lead to an increase in susceptibility [34]. It was hypothesized that increased aerobic fitness leads to higher tonic levels of certain hormones such as vasopressin or adrenocorticotropic hormone which might reduce the efficacy of acute release of these hormones in a motion situation [156].
However, aerobic fitness was not predictive in all environments. One study [49] did not find a relationship between the amount of self-reported physical activity and motion sickness susceptibility, without assessing VO2max. Another study [89] did not observe a significant correlation of aerobic fitness and the level of space sickness in astronauts flying to the International Space Station. It is possible that the metabolic changes for aerobic fitness do not apply at weightlessness. It must, however, also be noted that astronauts typically show drastically reduced variance in aerobic fitness compared to the general population.
Three studies furthermore investigated parameters of baseline salivary secretion of individuals who were susceptible and those who were tolerant to motion sickness. These studies found higher salivary amylase [82], higher amylase activity [73], higher total protein concentration [72] and higher secretion rate [72, 73] for susceptible participants. The exact parameters predicting motion sickness susceptibility in these three studies were rather inconsistent. However, all three studies concluded that their results reflect increased sympathetic tone for those susceptible to motion sickness. None of these publications presented a possible explanation for these relationships.
At first glance, the results from salivary secretion contradicted the previously mentioned studies on aerobic fitness to some extent as the latter is often associated with decreased resting sympathetic activity.
Further research with larger sample sizes is needed to clarify the role of aerobic fitness and the mechanism of differences in baseline hormone balance and put the findings into the context of a theoretical framework. Those studies could determine if the increased sympathetic tone is the result of acute or chronic stress which is triggered by increased physical activity and if stress is also affecting motion sickness susceptibility.
Hereditability and genetic factors
Environmental factors such as habituation have been discussed in a previous section. Despite the influence of the environment, a considerable genetic contribution to the occurrence of motion-related sickness has been considered in previous research. The studies in the publication set investigating genetic factors can be categorized into studies of ethnic differences (5 studies), hereditability (4 studies) and a genome-wide association study (1 study).
Research on ethnic differences has focused on an increased susceptibility within those of Chinese origin. More precisely, four of the five studies investigating the ‘Asian hypersusceptibility’ to motion sickness observed increased sickness reports of participants with Chinese ancestry. These studies include both self-reported motion sickness history [92, 104] and symptom ratings after exposure to an optokinetic drum [182, 183]. Furthermore, one study found a similar pattern for participants of Chinese ancestry who were American-born [183]. Participants of African ethnicity showed comparable levels of symptom ratings as participants who were Caucasians [182].
Conversely, a history of lower motion sickness and fewer motion symptom ratings after exposure to an optokinetic drum stimulus were observed among participants of Chinese ethnicity in a different study [106]. Interestingly, as a behavioral measurement, total tolerance time, i.e. the time until participants aborted each sequence on request, was significantly lower among those same participants of Chinese ethnicity, indicating an earlier or more severe onset of VIMS symptoms. The authors stated that these contradictory results may be caused by a lack of awareness of motion sickness symptoms or a socially-based and culturally-based response bias. Moreover, fewer symptom ratings could have been the result of shorter average exposure duration as participants of Chinese ethnicity aborted sequences sooner [106].
In summary, an increased susceptibility of persons of Chinese ethnicity to motion-related sickness seems likely. The reasons for these ethnic differences are as yet undetermined. It has been suggested that ‘Asian hypersusceptibility’ has a genetic reason [183]. Participants of Chinese ethnicity could either have a lower threshold for the detection of toxins in the body or differ in their physiological systems, e.g. in the release of stress hormones such as vasopressin, which they found to be elevated in participants of Chinese ethnicity during drum exposure.
Besides differences between ethnicities, hereditability was investigated by assessing consistency in motion sickness susceptibility between parents and their biological children and comparing concordance rates between monozygotic and dizygotic twins. Three studies reported a significant increase in susceptibility of children if at least one of their parents indicated severe experiences of motion sickness [172, 201], and even higher when both parents indicated severe sickness [1]. Concordance rates of monozygotic twins were significantly higher than concordance rates of dizygotic twins [161, 172]. The heritability of motion sickness was estimated to be at around 59 % [201] to 57 % [161], and all studies clearly indicated a genetic contribution to motion sickness susceptibility. The influence of genes is probably highest at a younger age as the concordance rates of monozygotic twins was highest at childhood (70 %) and decreased at a higher age when environmental factors probably have a greater impact [161].
As for the question which genes play a role in motion-related sickness, a very large study involving 80,494 individuals was conducted [87]. Unfortunately, motion-related sickness was assessed by a single item asking for experience of motion sickness in cars. This could have severely restricted the generalizability of the results. Due to the large sample size, gene sequences that were related with a p-value smaller than 5×10-8 were considered significant. By this procedure, 35 genes were identified to be related to motion sickness susceptibility. These genes were associated with a number of different phenotypes. The gene with by far the lowest p-value was PVLR3, which is involved in the development of the eye. Loss of PVLR3 expression leads to ocular defects in mice and humans. Many other genes were related to inner ear development, balance, glucose homeostasis, insulin homeostasis or migraine. These results support the emphasis on research for vestibular and ocular aspects in the prediction of motion-related sickness.
Other physiological factors
Some additional physiological factors for the genesis of motion-related sickness have received only little attention. Although some might gain valuable insights into the genesis of motion-related sickness or are able to explain why individual susceptibility varies to a great extent, most of the following factors are based on only three or fewer publications (some additionally with small sample sizes) and might need some further validation.
Three studies investigated baseline levels of stress hormones, namely cortisol [107, 133] or adrenocorticotrophic hormone [ACTH; 109] which is involved in the production of cortisol. It must be noted that baseline levels of these stress hormones are generally difficult to attain as these parameters highly depend on the time of day due to fluctuations with the circadian rhythm and could be influenced by the context of the (possibly stress-inducing) laboratory setting.
Higher baseline cortisol levels were associated with increased tolerance to an adverse rotation stimulus. However, this relationship was only found in female participants. Men, whose cortisol levels were not related to motion tolerance, might have been less willing to admit sickness symptoms, which masked the relationship [133]. Similarly increased ACTH baseline levels were also associated with fewer motion sickness symptoms during motion stimulation [109]. The direction of relationship surprises at first glance as this means that a higher level of baseline stress hormone activity is related to decreased sickness during stressful motion stimulation. Although the authors do not imply any causative relationship and speculate about the involvement of other related hormones (e.g. vasopressin or corticotrophin releasing factor) in the formation of the observed results, they hypothesized that participants with greater baseline levels of stress hormones more readily adapt to stressful motion stimuli, have greater responsivity of the endocrine system and are able to resolve environmental stress such as sensory conflict more easily [109]. However, contradictory results have been reported as well. In a different study higher baseline cortisol levels were observed for participants who later became sick in an optokinetic drum and attributed these differences to higher anticipatory stress and anxiety which in turn compromised well-being during drum exposure [107].
Due to the controversial findings, the predictive validity of baseline stress hormones for motion-related sickness remains unclear.
Another aspect is regular smoking or more precisely the influence of nicotine. Regular smokers were observed to be less susceptible to motion sickness when they are deprived of smoking overnight or for several hours [70]. The findings fitted observations of nicotine dosages increasing VIMS susceptibility [205]. Nicotine could affect the vomiting center or directly exacerbate sensory conflict by altering vestibular functioning. Furthermore, nicotine is known to increase acetylcholine release which activates muscarinic receptors. Thus, nicotine deprivation indirectly reduces muscarinic receptor activation which is similar to the effect of anti-emetic drugs such as scopolamine [70]. Unfortunately, no non-smoking control group was included to test whether nicotine deprivation protects against motion-related sickness or if regular smokers are generally more susceptible and only return to a “normal” level when deprived from smoking.
In two studies, the susceptibility to vasovagal syncope was linked to the susceptibility to motion sickness in children [20] and adults [19]. Vasovagal syncope is a brief loss of consciousness caused by a sudden drop of heart rate and blood pressure. As this relationship is also observable in family members of the participating children, the authors suggest a common genetic foundation for both motion sickness and vasovagal syncope, emphasizing the link of motion sickness and the autonomic system [20].
Elevated levels of motion sickness history were also found in patients with adolescent idiopathic scoliosis (AIS), a medical condition of curvilinear deformation of the spine during adolescent growth [26]. AIS is often accompanied by difficulties of postural control, attributed to either a deficit in sensory modalities or inadequate central integration of multiple sensory inputs.
According to the evolutionary hypothesis [192], motion sickness is a residual symptom of a toxin detector that identifies malicious substances and subsequently excretes substances that evoke similar symptoms as motion sickness. Thus, motion sickness was investigated in relation to other mechanisms of detecting possibly toxic constituents like unpleasant odors, (bitter) tasting or food aversions.
Super-tasters of phenylthiocarbamide which is essentially bitter tasting were reporting the highest motion sickness history, although the relationship was non-linear and normal tasters had the lowest susceptibility [174]. In a more recent study, somewhat contradicting results were found in non-tasters being the group with the highest motion sickness history [14]. But again, the relationship was not linear. The authors suggested that susceptibility to nausea may have co-evolved with bitter tasting in the sense that nausea as a response to ingested toxins is unnecessary if normal bitter tasting serves as protector against toxic substances. In a different study, individuals who preferred sweet over salty taste and who were more sensitive to unpleasant odors were more susceptible to motion sickness [173]. Motion sickness history has also been shown to correlate with the number of food aversions a person indicates [60]. No significant baseline differences in vitamin B12 blood concentration for susceptible and non-susceptible participants were found [110].
Phenotypical analysis in the large genome-wide study [87] discovered correlations of motion sickness susceptibility and poor sleep quality. Insomnia patients displayed more symptoms during a driving simulator, although it must be noted that the insomnia patients were not well matched to the controls in terms of age or psychological variables such as anxiety and depression and consisted of females only [4]. However, the results suit findings of increased motion sickness severity of sleep depraved participants in rotating devices [51, 96]. The results indicated that the VOR time constant is prolonged for those who are sleep deprived and that fatigue could compromise the ability to adapt to adverse motion environments. Thus, poor sleep quality could yield chronic fatigue and a chronically extended VOR time constant, exacerbating motion sickness susceptibility [96].
Lastly, there seem to be differences in white matter diffusion along a tract (inferior fronto-occipital fasciculus) connecting the right visual motion processing area (MT/V5) and the right anterior insula between susceptible and non-susceptible individuals [145]. However, the causation, whether increased white matter integrity led to increased motion sickness or the elevated integrity is a result of frequent nausea experience, is unclear.
Psychological aspects
Anxiety
Anxiety is the most often investigated personality trait in relationship to motion-related sickness. The object of investigation ranged from state anxiety to trait anxiety, a general tendency to be more anxious in various situations, and neuroticism, a similar concept with additional aspects of impulsivity and depression.
Studies assessing state anxiety either right before [102, 196], during [68, 153] or after an exposure [103, 196] to an actual or visual motion stimulus predominantly observed relationships between the level of state anxiety and expressed sickness severity. On the other hand, two studies did not provide significant correlations. However, one lacked in sample size [102] and the other [68] investigated the response to parabolic flight and thus might have had a very restricted sample as probably only those people would voluntarily participate who are generally not particularly anxious. Apart from that, state anxiety, although influenced by trait anxiety [180], is thought to be highly dependent on environmental factors and not very stable across multiple situations and therefore will not be discussed in more detail.
The other publications assessed anxiety as trait anxiety, neuroticism or as something in between state and trait anxiety referring to states of anxiety within a predefined time frame such as two, four or six weeks prior to the assessment. In the interest of simplicity, these will in the following be referred to as ‘anxiety’ despite the disparity in meaning. The questionnaires employed in this process of assessing anxiety are manifold: State-Trait Anxiety Inventory [STAI-T; 180; used in 6 studies], Eysenck Personality Inventory [EPI; 56; 4 studies], Taylor Manifest Anxiety Scale [TMAS; 191; 2 studies], 16PF Questionnaire [27; 1 study], Eysenck Personality Questionnaire [EPQ; 57; 1 study], Hamilton Anxiety Scale [HAS; 81; 1 study], Maudsley Personality Inventory [MPI; 90; 1 study], NEO Personality Inventory Revised [NEO-PI-R; 40; 1 study], Self-rating Anxiety Scale [SAS; 206; 1 study] and a self-made anxiety questionnaire.
Nine studies provided information on 14 relationships between different measurements of (trait) anxiety and sickness severity or history. Four studies did not provide sufficient information for the computation of effect sizes of which two, however, stated to have found a significant relationship between anxiety and motion sickness history [39] or cybersickness [179] while two did not find a significant relationship [48, 116].
Figure 5 presents the effect sizes of the remaining publications with indications of the test employed. The effect sizes were remarkably concordant and most of them range in between r = 0.26 and r = 0.41. Ten of the fourteen tests resulted in a significant relationship between anxiety and motion-related sickness. Slightly lower and non-significant was the relationship with the 16PF (Sixteen Personality Factor Questionnaire), which assesses a broad range of sixteen different personality factors. In one study [63] three scales from the 16PF were used: C (affected by feelings – emotionally stable), O (self-assured – apprehensive) and Q4 (relaxed – tense). These three scales possibly do not reflect trait anxiety as good as other measures and are therefore only weakly related to sickness scores. Standing out on both extremes of the list are two correlations reported by the same study [15], obtained separately for men and women. For women, the author found the highest of all correlations reported (r = 0.62) while the effect was absent in men (r = 0.06). He concluded that motion sickness might be primarily related to neuroticism in women and to vestibular disturbances in men. In a way, the results refuted the hypothesis of gender differences being caused by social demand as there should have been a higher correlation for men due to equally high social demands on males presenting themselves as not anxious. It needs to be mentioned that the sample size in the aforementioned study [15] was fairly small and the effects for men and women comprise of only 12 participants each. The range of the confidence intervals shows that the gender differences could also be much smaller (Fig. 5).
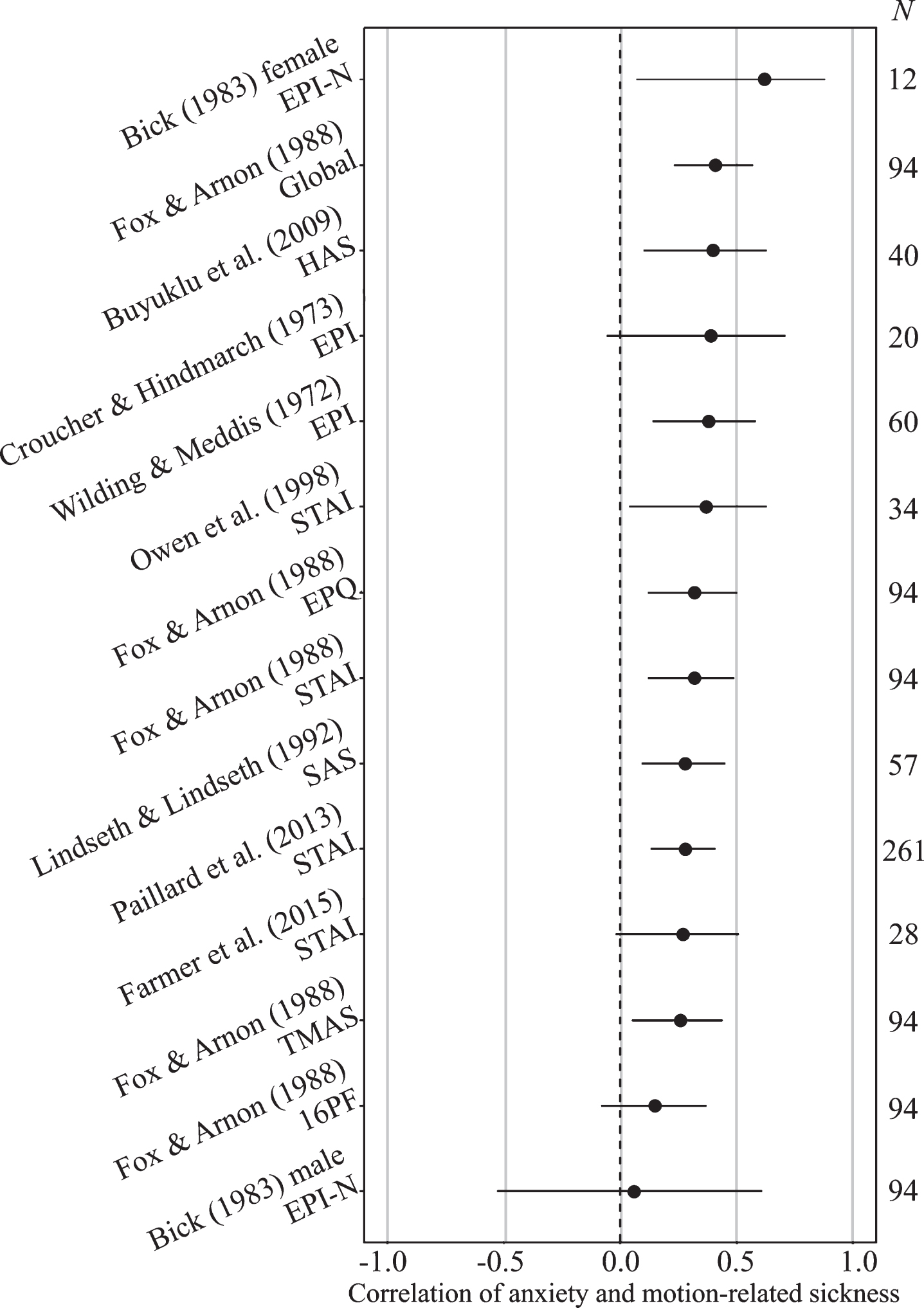
Effect sizes and 95% confidence intervals for all studies investigating (trait) anxiety and motion-related sickness.
Apart from that, the highest correlation was attained in a study [63] using four different measurements to assess anxiety. From the scores of all four measurements, the authors computed a composite global score of anxiety. This global score, probably due to its increased reliability, was best at predicting individual motion sickness scores of their participants (r = 0.41).
In a subsequent analysis, the correlation coefficients from all studies providing sufficient information were pooled with Hedges-Olkin fixed effects [83]. From the study using different measurements [63], only the correlation of the global score was included as the study would be overrepresented otherwise if all five correlations had been adopted. The pooled correlation resulted in rpooled = 0.33 (95% -CI: 0.26 – 0.40). However, it must be noted that the studies differ considerably in the assessment of motion-related sickness and anxiety and this was not taken into account in the calculation of the pooled correlation.
In summary, most studies supported the notion of a relationship between anxiety and motion-related sickness. However, only few were giving a proper rationale to explain why anxiety could be related to the genesis of motion sickness. Some symptoms of motion-related sickness may be intrinsic to anxiety as well, although nausea is usually not one of them [63]. It was suggested that anxiety directly affects postural balance and leads to deficiencies in postural control and hence to increased motion sickness susceptibility [148].
It is also possible that anxious individuals may tend to be more attentive or alert to internal states of the body and might also facilitate the appearance of symptoms of motion-related sickness [63]. This latter hypothesis is supported by the finding that motion sickness susceptibility and more severe symptoms of cybersickness are correlated with the tendency to catastrophize sensations of pain [142].
Virtual realities gained increased attention by phobia research due to its great potential for use in exposition therapy. As cybersickness is a common side-effect of virtual reality exposure, some studies investigated if cybersickness might be problematic when used in therapy or generally if phobic patients have an increased risk of getting sick when exposed to motion-related stimuli. Obviously, phobias are closely tied to anxiety.
Three studies investigated different specific phobias and their relation to motion-related sickness using visually presented stimuli. Two of them used a VR [164, 196] and one induced VIMS by means of a moving room [59]. Unfortunately, these three studies had some methodological issues. For this reason, the validity and generalizability of the results may be compromised.
Claustrophobia was found to be related to the level of VIMS when participants were restrained during exposure [59]. In contrast, there was no relationship when participants were unrestrained. However, claustrophobia was measured as a condition that comes very close to state anxiety in a restrained condition. This assumption is supported by the fact that more people without symptoms of sickness disclosed to have experienced claustrophobia in the past. Also, the authors suggested that claustrophobia (during the restrained condition) might cause an increased susceptibility to experience sickness. It seems equally likely that symptoms of sickness cause claustrophobia when restrained and impeded from withdrawing.
In another study, non-phobic controls were matched to patients with different specific phobias [164]. The participants were then exposed to a virtual reality display depicting the content of the respective phobia or the phobia of the matched patient. Phobic patients were showing higher cybersickness with a medium effect size. These results, however, could be explained by elevated state anxiety of phobic patients when exposed to the fear-inducing stimulus alone. Given the largely diverging levels of trait anxiety between phobic and control groups, a specific effect of phobia on cybersickness is unlikely.
The third study observed a relationship of agoraphobia and cybersickness during combined audio and visual stimulation but not when exposed to visual stimuli alone [196]. The increase in cybersickness among phobic patients was accompanied by higher state anxiety during audiovisual compared to just visual stimulation. An explanation for these results could be impaired multisensory integration ability among agoraphobic and anxious patients.
Finally, a significant correlation between acrophobia (fear of heights) and motion sickness history (r = 0.43) was found [173].
The interpretation of these studies with regard to the role of phobias is difficult as phobic groups were confounded with elevated trait and state anxiety. Future studies should balance anxiety levels between phobic and control groups in order to determine if there is a specific effect of phobia on sickness levels or if the relationship is caused by increased vulnerability of phobic patients for fear responses under certain conditions.
For other psychological disorders, the works of Charles Mirabile are pivotal. Mirabile was the only researcher to investigate psychological disorders and motion sickness history in more detail as he was trying to establish motion sickness as an objective predictor of various psychological disorders. In all of his studies, he used a motion sickness history questionnaire to attain a spectrum of differential motion sickness susceptibilities by disorder. Some psychological disorders were overrepresented at different points of the spectrum: passive-aggressive personality disorder as well as alcohol and heroin addicts have a low susceptibility; schizophrenia patients have medium-high susceptibility; emotionally unstable and antisocial personality disorders had the highest susceptibility [134, 137].
In a later study, patients with a seasonal affective disorder (SAD) were more likely to be susceptible to motion sickness, an effect which was not present in non-seasonal affective disorders [136]. Furthermore, patients with SAD who were also highly susceptible to motion sickness were more responsive to light therapy than motion sickness resistant patients. Thus, they suggested that common sensory (dys)function might play a role in SAD as well as in motion sickness.
One criticism against the studies by Mirabile and colleagues is that most studies, except the latest [136] did not incorporate healthy controls but only used a psychiatric sample with various different disorders. This complicated estimation whether patients of certain psychological disorders were having an increased susceptibility to motion sickness or lied in the normal range of susceptibility. Furthermore, despite assuming neurobiological causes, Mirabile and colleagues do not offer explanations as to why certain psychological disorders should be related to motion sickness and others not.
Overall, the practical benefit of motion sickness to predict or identify psychological disorders is very limited. Some disorders might be related to motion sickness history but the reasons are unknown.
Personality
Thirteen studies in the publication sample investigated personality in relation to motion-related sickness (excluding those only investigating anxiety/neuroticism or personality disorders). The idea of personality influencing the susceptibility to motion-related sickness was first raised by the receptivity hypothesis which claims that individuals who have a generally higher sensory receptivity are also more prone to become motion sick [157, 158]. This theory, referring to the cortical inhibition theory [55] stating that introverts are having greater neural response given the same sensory input than extroverts, suggested that introverts should also be experiencing stronger sensory conflict while exposed to motion-related stimuli. However, out of nine studies investigating extraversion, only three found significant relationships between extraversion and motion sickness, in the sense that introverts were more susceptible [39, 147]. Six studies were not able to replicate any relationship between extraversion and susceptibility to motion-related sickness [15, 199].
Since extraversion did neither show a relationship to the spiral after effect [41], the receptivity theory has been generally considered disconfirmed. Most studies were conducted prior to the 1990 s and investigated the relationship to motion sickness severity or history. However, two newer studies using visually presented motion likewise found no relationship [48, 58].
One study [98] assessed the tendency to cope with stress on the repression-sensitization scale [24]. Repressors tend to ignore and avoid facing stressors while sensitizers try to actively cope with the stressor at hand. In this study, repressors reported greater motion sickness while at sea.
Participants scoring higher on alexithymia, i.e. the inability to identify emotions in oneself and others, were experiencing more motion sickness, probably misinterpreting bodily signals and somatizing emotional distress [122]. This suggested that participants, who are ignoring bodily stressors during motion-related stimulation, either by personal tendency or by inability, are experiencing somewhat greater motion-related sickness.
Some other personality constructs were part of only one or two studies in the current publication sample. From those, higher motion sickness history was assessed for participants who had low psychoticism [71], low perfectionism [147], low sensation seeking [3] and low obsessiveness [122]. Other constructs did not yield significant relationships with motion-related sickness: locus of control [39, 98], validity scales [166] and most scales of the 16PF failed to show linear relationships, except social boldness, perfectionism and the primary factor extraversion [147].
Perception (Field dependency)
The majority of studies in the area of perception were conducted on field dependency. Field dependency is defined as a perceptual style in which the perception of an object is either strongly dependent on the object environment (field dependent) or independent of it (field independent) [200].
There are generally two different procedures for measuring field dependency. In the first method, participants must recognize geometric shapes embedded in more complex contextual shapes which ought to be ignored (embedded figures; EFT). In the second method, the participants sit in a tiltable chair within a darkened room and look at an illuminated frame with a rod in the middle (rod and frame test; RFT). Chair, frame and rod are vertically deflected and the participant cannot touch the ground. The task is to rotate the rod to a vertical position relative to the physical ground, ignoring the orientation of the frame and the own body. Task performance is determined by the deviation from the optimal vertical position (true vertical). Participants who can complete this task well are considered to be field independent.
In the present set of publications, seven studies were conducted, which examined the rod and frame test in connection with motion sickness, four used the embedded figures test and one study used a test that was similar to the rod and frame test.
Of the seven studies with the rod and frame test, six reported that there was a significant correlation between the result in the rod and frame test and the severity of motion sickness [10, 202]. One study [138] did not find a significant relationship, neither did the study that used a similar test to the rod and frame test [152]. Another study [35] found an interaction of field dependency with off-vertical axis rotation in light or in the dark. Field dependent individuals were generally not more susceptible to motion sickness but exhibited more sickness when the adverse rotation was administered in the dark without any visual cues.
Unfortunately, both studies not finding a linear relationship between the rod and frame test and motion sickness history did not report sufficient data of the linear relationship to compare them to the other studies. The pooled correlation of the remaining five studies with Hedges-Olkin fixed effects resulted in rpooled = 0.47 (95% -CI: 0.36 – 0.58).
For the embedded figures test none of the publications listed here could determine a significant connection with motion-related sickness [11, 127]. Although the rod and frame test and the embedded figures test should measure the same construct, the correlation between the two tests often does not seem to be higher than r = 0.50 [126]. A different study achieves a correlation of r = 0.61 [7], which is higher, but with a shared variance of 37 % there is low evidence for measuring the same construct.
Both tests are considered indicators of the ability to correctly perceive a stimulus in the presence of a conflicting context. With the embedded figures, both the stimulus to be perceived and the context are purely visual. In the rod and frame test, the conflicting context is generated both visually and vestibularly. Therefore, even theoretically it is much more likely that the rod and frame test is more closely related to sickness caused by a sensory conflict.
Another aspect that has only been investigated in one study so far is autokinesis, i.e. the phenomenon in which a small visual point of light that is actually stationary is perceived as moving. The study found a significant link to motion sickness history and concluded that both motion sickness and autokinesis were related to a vestibular system dysfunction [139]. Unfortunately, no attempts have yet been made to replicate the found connection.
Cognitive performance
The relationship between parameters of cognitive performance and motion sickness was investigated in two studies, in the sense that cognitive performance can predict future motion-related sickness or motion sickness history. In the first study, cognitive performance was measured in the form of a concentration test in Taiwanese boxers before and motion sickness after a boxing bout [31].
Boxers who did not report motion sickness after the bout also achieved a significantly better result in the concentration test before the bout. The result is doubtful in several respects. The authors speak of motion sickness, since the head and body were exposed to several passive movements (i.e. enemy blows) during the bout. However, it is much more likely that the sickness was not caused by movement alone, but by injuries to the head, such as a concussion. It is therefore questionable whether this can still be classified as motion sickness. In addition, the correlative relationship leaves questions about the causal relationship between the two variables. It is quite possible that boxers with a lower concentration performance also showed worse performance in the ring and had to take correspondingly more enemy blows, meaning the number and strength of punches was not standardized. The value of the results for predicting motion sickness is therefore rather low.
The second study investigated the predictive power of spatial performance on motion sickness history [124]. A significant correlation was found in men but not in women. The correlations were explained by a possible greater sensitivity for the vertical upright in those who had higher spatial abilities. This explanation is reminiscent of field independence. Since there are no further studies on the subject and the correlations could only be determined in men, it remains unclear to what extent spatial ability can predict motion sickness and go beyond field dependence.
Limitations
A limitation of this systematic analysis of predictors is that the selection of the included studies was performed by only one person. A selection of two or more persons might have increased the reliability of the selection.
In addition, the presumably high number of non-significant or other unpublished results that are missing in many reviews or meta-analyses is a possible reason why the (missing) influence of certain predictors has not yet been further clarified. This review has only used published data and may therefore be subject to a certain publication bias.
Conclusion
The compilation of the results has shown that many of the presented interrelationships were based on only a few or somewhat controversial results. Further studies are necessary to determine replicability and to eliminate contradictions in the relationships found. Unfortunately, more systematic (or meta-analytical) methods could often not be applied, as the conditions and measuring methods were too different or the necessary data were not available.
However, the review of the literature has also found some promising predictors for motion-related sickness. The possible predictors and their obtained relationship with motion-related sickness are summarized in Table 4. Although most results suggested that sickness caused by physical motion (i.e. motion sickness) shows the same correlations as visually induced sickness (i.e. VIMS, cybersickness and simulator sickness), there were some meaningful exceptions such as age or labyrinthine defectiveness. Therefore, the findings for these two categories are presented separately. This approach also illustrates that some aspects that were predictive of motion sickness have never been investigated in the context of visually induced sickness.
Summary of the results of the literature review
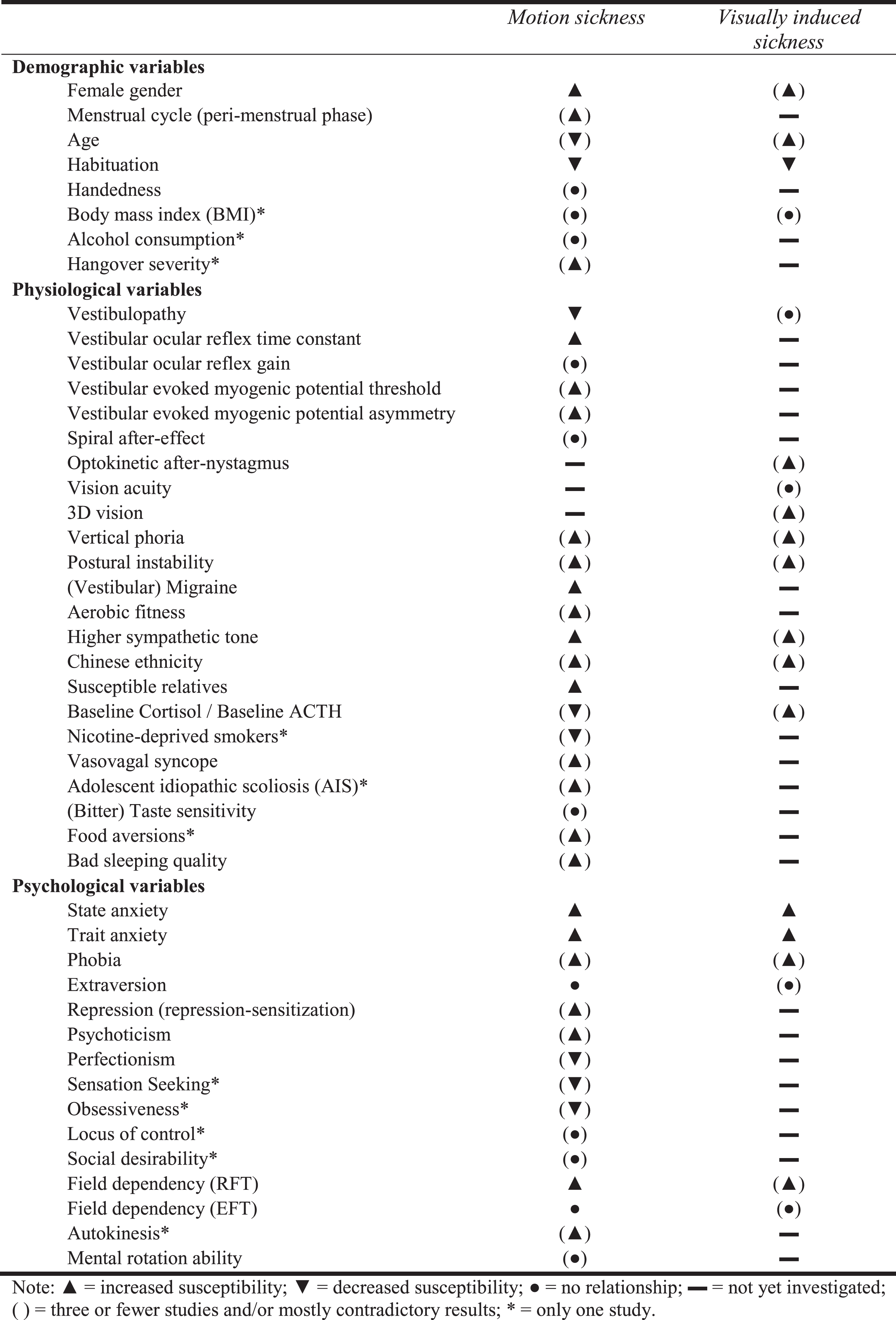
The most reliable findings for predicting motion sickness are gender, vestibular function, especially the length of the VOR time constant, the presence of migraine, the susceptibility of close relatives, great anxiety (both trait and state anxiety), field dependence, a high sympathetic tone. The presence of one of these predictors seems to increase susceptibility to motion-related sickness, while habituation to the adverse stimulus seems to reduce it.
There is less certainty about predictors for visually induced sickness (VIMS, cybersickness and simulator sickness). Gender, habituation, anxiety and possibly OKAN are currently the best available predictors of visually induced sickness.
As the genome-wide study [87] has shown, there seems to be a genetic link between the development of the vestibular and visual systems affecting susceptibility to motion sickness. In what way genes are affecting the susceptibility to motion-related sickness remains unclear.
Finally, there is probably a significant environmental impact on susceptibility, most likely represented by varying degrees of habituation. It is still unclear to what extent habituation for similar stimuli and different types of motion-related sickness can be achieved, even if results suggested certain generalizability. Anxiety as a general tendency to deal with aversive experiences may also influence susceptibility to motion-related sickness.
This review illustrates that despite being a long known phenomenon, individual susceptibility to motion-related sickness is still not fully elucidated. Although many indications pointed to physiological or biological differences, there is also reason to investigate psychological factors causing the large inter-individual differences.