
Abstract
Introduction
On a global scale, the need for sustainable work is increasingly felt for economic, political, demographic, and environmental reasons [1]. Stress related health problems due to psychosocial risk factors in the work environment, private situation, and personal characteristics are currently the leading cause of sickness absence and work disability in western countries, and as such, a threat to public health [2, 3]. Preventing future sick leave before sickness absence actually occurs can be more effective than counseling employees on sick leave, because of the limited effectiveness of treatment and rehabilitation [4, 5]. Nevertheless, investment in interventions to prevent sickness absence is low, especially for those with mild to moderate psychosocial health problems [3].
Dans et al. [6] refer to health screening as the cornerstone of preventive medicine. Screening for early disease or risk factors followed by appropriate early intervention is limited in Occupational Medicine. Recently, new and promising initiatives have been developed concerning prevention of long term sickness absence amongst office workers using a preventive approach [4, 8]. In a Randomized Controlled Trial [4], a preventive strategy comprising screening and early structured consultation with the occupational physician (OP) for preventing long term sickness absence (LTSA) due to a combination of factors related to work, private life, and (mental) health, was proven effective (see Fig. 2). Nevertheless, the delivery of early consultation appeared to be difficult because of unawareness of the high risk status amongst employees and unfamiliarity with the early moment of intervention amongst the OPs, as indicated during implementation. Because many interventions proven to be effective in health services research studies fail to translate into meaningful patient care outcomes across multiple contexts [9], we conducted a process evaluation among OPs in order to identify facilitating and hindering factors for future implementation activities. The design chosen for this process evaluation was a case study, focusing on experiences of OPs during the trial and afterwards, delivering the structured early consultation in occupational healthcare practice. A mixed method approach was followed using interviews and surveys.
Study context
In the Netherlands, the employer and employees within a company are primarily responsible for occupational health and safety policy. According to Dutch occupational safety and health legislation, the employer is obliged to contract an occupational safety and health service or an occupational physician. These contracts comprise the following four tasks for the employer [10]: Assist employees who are not able to work Review risk assessment and evaluation Conduct periodic occupational health examinations Conduct pre-employment medical examinations
Task number 1 is especially important, because in the Netherlands the social security system obliges the employer to pay at least 70% of the salary of the employee who has fallen ill for a maximum period of 2 years. About 90% of the occupational health service’s (OHS) time is spent with task number 1. In the last decades, lifestyle became an issue of concern. The occupational health services or the OPs in the Netherlands are external organizations/specialists working for one or more companies. The role of OPs and employers in primary prevention (referring to task 2) is regulated through the Labor Conditions Law (Dutch: Arbeidsomstandighedenwet). An assessment of all risk factors a company faces in safety and health has to be performed, including the psychosocial risk factors related to the work environment. However, this law does not provide explicit instructions on how to deal with the latter, and it is left to the interpretation of the employers and employees to identify and evaluate working conditions and stress at work [3].
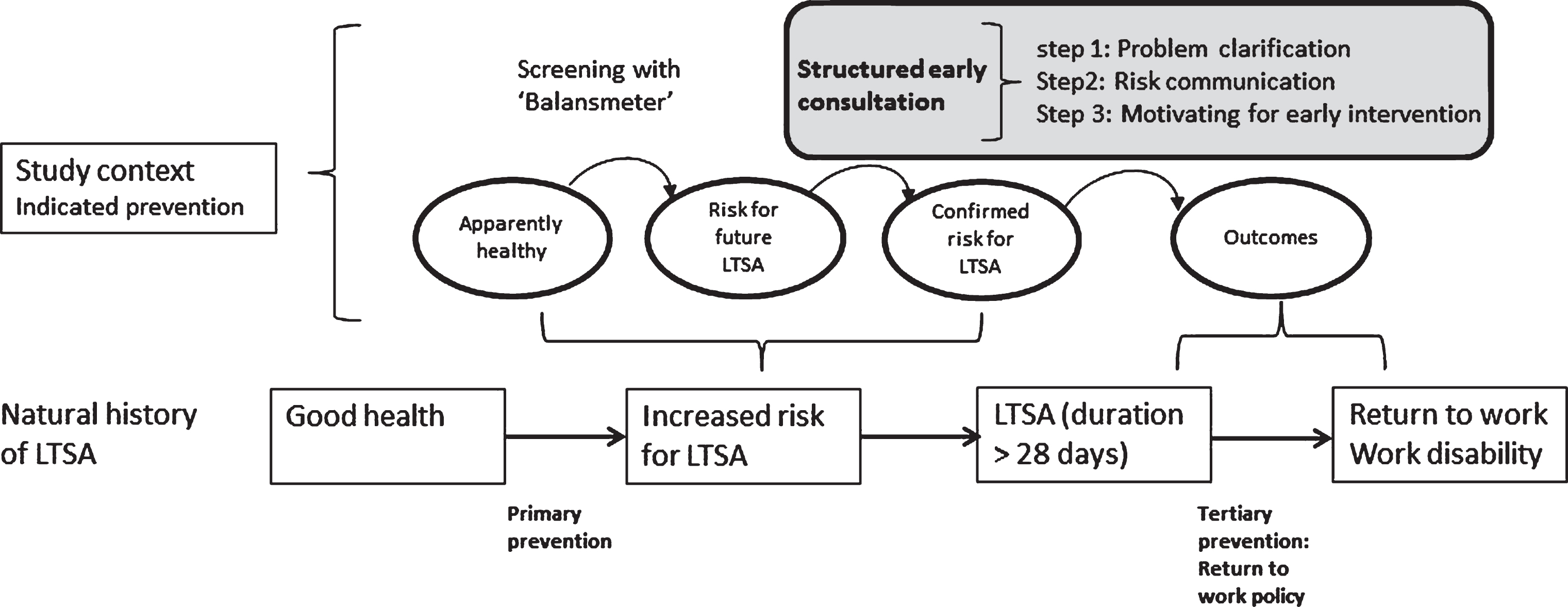
The preventive strategy comprises screening with a questionnaire (‘Balansmeter’) to identify employees at risk for future long term sickness absence and subsequent early structured consultation [4]. The screening questionnaire ‘Balansmeter’ is an algorithm-based prediction model built on data of the Maastricht Cohort Study (see Box 1) [7]. Employees with a high score on the screenings questionnaire and who are not listed as sick, are identified as being at high risk for LTSA in the near future, and are offered an early structured consultation with an OP. This consultation consists of three steps: 1. Problem clarification, 2. Risk communication, and 3. Motivation of the employee for engaging in an early intervention targeting the problem(s) identified in step 1. The early intervention, where necessary offered in the third step of the structured early consultation, can be delivered by different healthcare professionals (e.g. counseling by OPs, company councelors, psychologists, physical therapists or other allied health professionals) tailored to the specific needs of the employee. The characteristics of this preventive approach are visualized in Fig. 1.
Evidence Based preventive strategy (PS) comprising screening for high risk for long term sickness absence (LTSA) in the coming year, followed by a structured early consultation in occupational healthcare;
Evidence Based preventive strategy (PS) comprising screening for high risk for long term sickness absence (LTSA) in the coming year, followed by a structured early consultation in occupational healthcare;
Screening questionnaire ‘Balansmeter’:
The screening questionnaire ‘Balansmeter’ can be considered a statistics based prediction model developed on the data of the Maastricht Cohort Study [7, 27]. In this cohort study a well-balanced mixture of concepts and self-formulated items, related to the etiology of prolonged fatigue were investigated. The concepts related to prolonged fatigue, either as a potential determinant or confounder, were measured by using scales and subscales of validated measurement instruments [27]. The items comprising these scales and subscales and the self-formulated items were used for analysis and construction of the prediction instrument ‘Balansmeter’. This instrument captures 34 questions on demographics, work environment, private situation, (mental) health, and sickness absence history. The ‘Balansmeter’ shows good predictive values for future sickness absence (>28 days) amongst office workers. The threshold for the maximum amount of items to enter the prediction model was set around thirty. As a consequence individual items originating from whole scales or subscales, best adding to the prediction of future long term sickness absence, were selected on a statistical basis [7]. This resulted in the screenings questionnaire ‘Balansmeter’ for office workers comprising 34 items.
Target population:
Office employees of a banking company in the Netherlands without a prevalent participation problem are screened for LTSA risk status with the ‘Balansmeter’. Inclusion criteria are not being absent from work, not being pregnant and not receiving treatment by the occupational physician at the time of completing the screening questionnaire.
Early structured consultation: Employees at risk for long term sickness absence (LTSA) are offered an early structured consultation with an occupational physician [4]. This early structured consultation comprises three steps;
1. Problem clarification guided by the scores on ‘Balansmeter’
2. Risk communication, explaining the high score to the client including the problem clarification
3. Motivating the client for engaging in an early intervention targeting the problem(s) identified in step 1 (and 2). Early intervention can be step 1 and 2 followed by an advice of the occupational physician, can comprise follow up consults with the occupational physician, or can be a referral to another healthcare professional e.g. company counsellor, psychologist, dietician, physiotherapist or another allied health professional.
The preventive strategy comprising screening with the ‘Balansmeter’ and a structured early consultation is a promising approach, since reintegration of employees with long term sick leave (>28 days) is difficult and the risk of people leaving the work force is considerable. This screening strategy was proven effective in an RCT [4]. A significant reduction of the total sickness absence duration (mean 18.98 days in intervention group and 31.13 days in care as usual group) and a reduction in the proportion of long term sickness absence spells over one-year follow-up, in favor of the experimental group (9.1% in the intervention group versus 18.3% in the control group).
Screening for increased risk of long term sickness absence (LTSA) to prevent LTSA in the near future. (Figure retrieved and adapted from Dans et al. [6]).
The aim of this study is to investigate the experiences of OPs who deliver structured early consultation to employees with an increased risk for LTSA, and to develop insight into factors hindering or facilitating the consultation process during the trials and afterwards in every day occupational healthcare practice. This study may further facilitate and enhance future implementation of the preventive strategy.
Methods
Design
The OHS involved in this study used to be the in-home OHS of a large banking company, but in line with European legislation, the OHS in 2003 changed to an external organization. Since the time of this change, they provide additional companies with occupational healthcare. The case study report refers to the experience of the OPs of the OHS delivering the preventive strategy (PS) to the employees of the banking company. The PS was developed and implemented jointly by the OHS and Maastricht University. The trial referred to in Box 1 was conducted in 2003 [4]. After the trial the PS became one of the instruments routinely used by the OHS for preventing LTSA, alongside more lifestyle oriented preventive approaches. Noticeable, within the setting, occupational healthcare already was easily accessible for the employees during open office hours. The main difference between the open office hours and the PS is that in the first case, employees take initiative for consultation, whereas in the second case the physician initiates a consultation. Before the start of the trial (see Box 1), the OPs were invited to attend an introduction meeting in which the rationale behind the PS was communicated through an oral presentation by one of the management staff members; this was followed by a group instruction on how to perform a structured early consultation with a high risk employee. Experiences of the OPs were discussed during meeting days organized for OPs of the OHS twice a year, to warrant the sustainability of the PS in the long term.
For this case study a mixed method approach was used [11] comprising surveys to gain a broad understanding of the implementation process, and semi-structured interviews for a more in-depth understanding of experiences and perceptions. The topics underlying the surveys and the semi-structured interviews are presented in Box 2. This topic list was based on observations during the trial when implementing the PS.
Topics used for formulating survey questions and for framing the semi-structured interviews
Topics used for formulating survey questions and for framing the semi-structured interviews
– Experience with preventive strategy (PS) during trial and routine use afterwards;
– Attitude towards pro-active work style (as opposed to reactive work style defined as offering help on client request)
– Necessity of training for adopting a pro-active work style
– Consequences of timing screening and early intervention for motivation of professional to engage in the PS
– Perceived facilitators or barriers practicing the PS
– Perceived positive or negative effects of the PS
– Importance of the nature and severity of complaints for motivation of professionals to engage in the PS
– Position of the PS in current practice
The study sample for the surveys consisted of all 25 OPs working for the OHS on a salaried basis. Surveys were sent in September 2011 by email and the OPs were asked to send the completed survey anonymously to the University by post. A reminder was sent the following month to all of the OPs to increase response rate. Surveys contained structured items as well as open ended questions. By means of purposive sampling, a subsample of OPs was selected for a semi-structured interview (N = 5) in the period from August to October 2011 (N = 5). This selection aiming for a diverse range of opinions and attitudes was based on OPs attitudes toward working with this PS, as expressed during the implementation process. Two had a management function within the OHS organization in addition to the tasks of occupational physician. All interviews were taped, after the interviewees gave informed consent to do so. To increase validity, interviewees were asked to illustrate their experiences with cases from practice they had come across during structured early consultation. All interviews were transcribed verbatim by an experienced administrative assistant. All interviewees gave written informed consent for using the results of the survey and interview for research purposes.
Analysis
The survey data were analyzed by using descriptive statistics for the closed questions. The open ended questions of the survey were compared to the qualitative data to check resemblance with the patterned responses within the qualitative data. Thematic analysis [12] was used for analyzing the interviews with the professionals about this new way of working. The first and second author performed the first phase of the data-analysis (structuring data and initial coding) for this purpose. The interpretations and patterns were discussed during the process of analysis by the first and last author. Themes were discussed and all authors connected the themes to the theory.
Results
The professional perspective was investigated directly in this case study. Thirteen of the twenty-five OPs responded to the survey resulting in a response rate of 52%. All five OPs invited for the interview agreed to participate. The perspectives of the employees of the banking company were addressed indirectly, through the OPs.
The characteristics of the OPs participating in the survey and the interviews are summarized in Table 1. The OPs are about fifty years old and most had been employed at the OHS for over five years at the time the surveys and the interviews were conducted. This implies that the participants can reflect on the full range of time from the trial period (2003) to afterwards with routine use in daily practice (2003–2011). Two of the interviewees had management tasks (OP4 and OP5) and the others (OP1-OP3) did not.
Characteristics of occupational physicians (OPs)
Characteristics of occupational physicians (OPs)
n.a.: Not available.
In Appendix 1 the scores and frequencies as observed in the survey are given. Most of the OPs indicated they had a reasonable amount of experience with the PS in daily practice, seeing employees for a structured early consultation on a monthly basis (item 1–3). Their initial opinion regarding the PS (item 4), was scored on average 7.8 (range 7 to 9, on a 10 point Likert scale). Arguments for this high initial score were “the need for a more preventive workstyle in the future” and the general positive attitude towards preventing LTSA instead of counseling when already manifest. Preventing more severe damage and the possibility to identify employees at risk on an individual level were other reasons for appreciating the PS. When asked about current opinion (item 5) a mean score of 7.1 (range 4–9, on a 10 point Likert scale) was given. Five of the 13 OPs showed a decline in enthusiasm and reasons mentioned were: “expectations not fulfilled” (n = 2), “delay between screening and early structured consultation, resulting in no referrals” (n = 1), “low response to screening questionnaire” (n = 1), and “made switch to lifestyle oriented strategies”. The other eight OPs gave the same rate for current opinion compared to initial opinion.
A positive attitude towards the proactive workstyle in relation to the PS was scored by all OPs (item 6). All OPs thought the PS was ethical in case of psychological problems, 92% in case of somatic problems, and 85% thought it was ethical in case of work related problems (item 7). “Voluntary participation” and “unethical not to treat somebody at risk” were arguments used. None of the OPs had ethical concerns with regard to the PS (item 9). The response category “Mildness of complaints” and “No question for help of employee” were scored by 3 respectively 2 of the OPs. Positive aspects of the PS (item 8) scored by the OPs most often is the category “Preventing LTSA” (77%), followed by “Monitoring health of employees” (54%), and “Preventing depression” (46%). The category “No positive aspects” was never scored.
When OPs were asked about possible concerns mentioned by the employees with regard to the PS during consultation (item 10), resistance of employees against raising awareness about problems not yet recognized by the employees themselves was frequently mentioned. Sixty-one percent of the OPs mentioned not being trained for performing the PS in practice (item 11) and 54% thought additional training was desirable (item 12). All OPs thought the PS was of value in addition to the open office hour consultation (item 13), but they thought the PS could not replace the open office hour because employees should be able to take the initiative for consultation as well (item 14). The perceived efficacy of the PS (item 15) was scored positive by more than half of the OPs and all but one would recommend the PS to colleague OPs outside the OHS (item 16).
Thematic analysis of interviews
Thematic analysis resulted in seven themes describing experiences and perceptions of the OPs with delivering the early structured consultation to employees at risk for LTSA.
Multifactorial prediction model is difficult to understand
Because of the awareness that participation problems are difficult to deal with when manifest, the OPs wanted to work more preventive in this area. They had positive experiences with screening and early intervention for other conditions like cardiovascular risk factors and RSI;
[OP2] “Then we said: we could use something like that for psychological complaints, because we saw a shift towards mainly psychological reasons for sickness absence. And if we could work in a preventive way – just like in the RSI program – it would generate a lot of profit for us.”
[OP4] “[ ... .] how can we shift from cure to early intervention, [ ... .] the occupational physicians, but also other professionals were confronted with all kinds of people in trouble. Strain, burnout or whatever and then you fantasize “it’s a pity we didn’t saw these people earlier, because then we could have made adjustments more easily. Then the need for interventions would have been fewer etcetera.” But the eternal question is “Who are those people”? How can we recognize them earlier or identify them or whatever? [ ... ] on the individual level we practically couldn’t do anything.”
Screening with ‘Balansmeter’ and structured early consultation (PS) offered a solution but proved to be more complex than expected in practice. The screening questionnaire puzzled the OPs, since it is not constructed on concepts, but on items predicting LTSA based on statistics. The initial amazement amongst the OPs was formulated by OP4;
[OP4] “It was a surprise to us [the OPs] that the way of thinking significantly changed. From the perspective of science, [ ... ] whole concepts were considered relevant. Is the concept of depression predictive ... or should we consider the concept of attention deficiency or whatever ... In the end, very practically, it appeared to be specific items, not whole concepts, [ ... ] You know? Purely from a statistical perspective.”
This combination of items without one clear conceptual basis made it hard for risks to be recognized by OPs and employees;
[OP1] “We [the OPs] tried to score the questionnaire [during an in service training] and we were asked if we knew which items would generate a high score or not, and we were all wrong.”
[OP1] “I don’t think he [employee] had taken any action himself if he wasn’t eh [ ... ] he was not miserable enough to go visit his GP or OP by himself, because he was not experiencing a peak problem at one moment in time ... .For a lot of problems, you know, today isn’t much worse than yesterday you see. Not much better, not much worse. But in the course of half a year, these problems may grow. And most of the time people only realize this has happened when it is too late. When they are already absent of work or if the problems have grown over their heads.
The latter quote illustrated the perception of the OP that an imbalance in private life, psychosocial work environment, and (mental) health can make a person vulnerable in the long term. It is a possible manifestation of increased risk for LTSA. Because of this unawareness, problem clarification was a challenge for the OPs. Of course, this is also the case in other preventive strategies. Yet, the issues at stake there are easier to understand;
[OP4] “Why is lifestyle so much easier to discuss? Because everybody can understand it. Weight, smoking, and off they go. As a matter of fact they need a kind of frame. When we talk with customers or companies [other companies served by the OHS thinking about implementing the PS] we try to find a suitable mold, but we have not found the ideal mold yet.”
[OP1] “You just do your consultations and you advise people where they can change things, but I doubt whether this can be called an intervention.”
The diffuse nature of the increased risk for LTSA and the variety of possible early interventions make it difficult for the OPs to delineate a uniform picture of the PS. Compared to screening strategies for somatic risk factors like increased cholesterol level and blood pressure, which in case of abnormal values can be dealt with according to a standard treatment protocol, the diagnostic process and the intervention are much more intertwined in the PS.
The absence of a question for help is a difficult starting point for communication
In healthcare, a question for help or a perceived risk usually triggers clients to visit a healthcare professional. Given the unawareness of the imbalance of factors concerning private life, the psychosocial work environment, and (mental) health, a question for help is lacking as a starting point for the structured early consultation.
[OP4] “During the trial it became clear that the stage of the problems screened for was different from every day practice”[ ... ]”24 out of 25 employees are surprised to be invited for an intake”
[OP5] “It soon became obvious to us that the strange thing was that people are identified on a moment in time when they’ve not formulated questions themselves, when they’re not absent yet, but also they actually still wonder if there is something going on even if you discuss it with them. This is still a problem in current practice. Yes it is still difficult to motivate people.”
“[OP4] Because you operate earlier on the time axis, which was our original aim of course, towards early recognition of problems [ ... ] the role of all players involved becomes different.”
Furthermore, employees often feel overwhelmed by the high risk message;
[OP3] “Sometimes they are startled: “Gee, apparently something is wrong”. That is a frequently heard reaction: “I have to come and see the doctor, something is wrong”. ” ... . And then it’s not so bad. It’s also very much the way you communicate it, I think.”
Communication was often mentioned by the OPs in the interviews as crucial for all three steps of the early consultation (problem clarification, risk communication, and motivation for early intervention).
Trust and privacy
An important issue mentioned by the OPs was trust. The employees have to trust the occupational health professionals when sharing delicate information about their health, work and private situation, and how these domains influence functioning at work. Given the image of the OP in many companies as being the right hand of the employer, this can create an obstacle for participating in screening or attending the structured early consultation;
[OP3] “We have different roles and most of the time our role is to control for sickness absence, counseling those on sick leave, certifying sick leave, tasks related to sick leave. That’s how the people [employees] know you. The other roles [including preventing sick leave] are less well known. We used to be called physician for controlling sickness absence [on behalf of the employer]. We can’t get rid of that label” [ ... ] Yes that is a handicap.”
The quote shows that the OPs had difficulties with image. They thought that professionals outside the OHS, for example GPs, are more easily trusted;
[OP1] “If there are problems related to the work environment, and if they think I’m on the bosses’ chair [ ... .] Than it would not surprise me if they think “O, apparently I do have a problem. I better go and talk to my GP [instead of seeking help from their OP].” And those people, we never see them of course”
Although confidentiality was stressed explicitly in the information accompanying the screening procedure, and although the information shared with an OP is protected through privacy legislation, OPs noticed during consultations that employees were worried about improper use of the information. Also some of the OPs perceived the privacy of information collected during the PS as inadequate, because too many people within the organization had access to the information system e.g. assistants in the OHS.
Fear of being labeled
Employees are aware that the nature of the problems identified was often related to mental health or psychosocial in origin and they fear being labeled with such issues. This makes screening with the ‘Balansmeter’ different from screening for pure somatic risk factors;
[OP2] “ ... .You have to realize that physical is more easily accepted. Physical complaints are way easier to discuss than mental complaints ... “No, I don’t mention it to anyone that I eh ... Yes, if I had a stomach ulcer it would be different but now burnout and it is not something I’m going to say out loud”
[OP1] ... “that is the advantage of an occupational physician over a company councilor right, a lot especially the higher educated [employees] they visit a doctor more easily under the guise of measuring blood pressure or cholesterol, while in the meantime something else is going on, but they don’t want to admit right away that they feel distressed. It entails a disqualification, that you are not able to manage your affairs well.”
Being labeled through screening might result in stigmatization;
[OP2] “ ... Yes, resistance with regard to getting a label ... .They feel like getting a label on their forehead ... .Especially a mental label is very bothersome.”
[OP1] “Yes. Afraid for getting an exclamation mark behind their name; this is a weak person. Or a category similar to that.”
[OP1] “I think that ... resistance occurs especially when things are wrong in the work environment. For example, when reorganizations are planned, people think: “How does it serve me to score this questionnaire ... Let it all be. I will not participate.”
This fear for labeling amongst employees can hinder the communication between employees and OPs during all three steps from the structured early consultation.
No action in the absence of a clear problem
A more proactive attitude of the OP is necessary given the generally low awareness of the increased risk on the employee side. The OPs indicate difficulties with this, which seems related to daily routine, work style, and work pressure;
[OP1] “ ... targets are agreed with our clients [companies who hire OHS], ... yes, that means that our agenda is filled and that you really can’t reserve time for other things ... .So, yes that gives some friction. Yes, right now the priority is acting in cases of sickness absence and that is not what they say out loud but it is implicitly the message. So that is what we predominantly do, and if you can save time to do other things, you do these other things [spending part of the reserved hour for a structured early consultation on other things]. But, if you want to change this situation, than you should prioritize prevention instead of sickness absence, and then you should spend time on it purposely.”
The routine workstyle of the OPs, as for medicine in general, is strongly influenced by the principle of ’doing no harm’ as indicated explicitly by the OP4;
[OP4] “If not really necessary, we prefer to do nothing. That attitude still remains. This goes for the whole healthcare system, by the way.”
This workstyle originates in the former education of physicians;
[OP2] “Given our former education it is ... yes somebody comes to see you if feeling ill ... .You actually should try to prevent people from becoming ill before they come and see you.”
Employees foster the idea that the OP comes into action in case of actual sickness absence;
[OP2] ”It’s also strongly the belief of employees ... .the company doctor or the occupational health service comes into the picture when something is wrong.”
[OP1] “Yes, I think these proverbs are used for a reason, right. “It is no use locking the stable door after the horse has bolted”. I see it happen every day and I think well they solve it now, but the damage has been done and so yes, although I do think we should work on prevention, I sometimes question if it is realistic. Maybe it isn’t until people actually feel the negative impact of their actions that the right moment is there to work on it.”
According to OP1, problems with motivation for tackling early problems are inherent to the early moment in time of screening and intake. Employees do not feel the consequences of the problems in this early stage, do not formulate a question for help, and are not willing to deal with the efforts an early intervention might cost. Together with the principle of ‘doing no harm’ adhered to by the professionals this might hamper implementation of the preventive approach in practice.
Preference for prevention in the work environment
The PS is implemented in the existing OHS practice as a method for preventing LTSA at the individual level. The main focus of prevention by the OP is influencing the work environment through interaction with executives. The OPs without management related tasks mention this way of working as meaningful;
[OP1] “Advising, supporting. Yes. What I really try to do is to explain to them [executives] their role and added value. So I’m not saying “you do a bad job”, because I think it’s really difficult for a lot of executives to handle difficult situations well and yes, for a lot of the difficult absentees, some relevant issues are prevalent. And yes if you don’t have access to an extensive medical history, I can imagine it is difficult. And that’s where I try to provide some relevant background information to them, to create some awareness of the do’s and don’ts and how to perform well.”
[OP3] “ ... .than you become much more active on the organizational level ... ..interfering with the way the company deals with human resource management. How they design work conditions and other related issues ... .In my perception, my personal opinion, you are really effectively influencing health and as a consequence the kind of functional health of employees, I mean the kind of health they need to carry out their work. In this way you can add to creating a better work environment or work culture.”
The quotes above show a strong preference for prevention on the level of the work environment. In relation to the structured early consultation, the process of problem clarification can be hindered, when problems in the psychological domain are questioned less effectively. This might be related to or fortified by reticence of employees to share mental health problems or the employee’s unawareness of these problems.
From believing, to ownership, to practicing
The attitude of the OPs towards prevention in general can be characterized as positive and part of their professional ethics;
[OP3] “I think in the end...yes slowly we are drifting from the reactive side towards advising and helping to influence [employee] behavior.”
They all believe in guiding employees towards more healthy behavior and empowering them through enlarging their autonomy with regard to managing their own health;
[OP2] “I strongly believe in prevention and I strongly believe in good health education, so people can choose which way they go.”
Yet ownership of the newly introduced PS, in terms of fully adopting it in their routine, was not realized amongst all OPs. From the beginning, OP4 and OP5 were involved in research and development of the PS. This strengthened their sense of ownership enormously and played a role in mitigating the impact of the ‘no harm principle’;
“Yes when we were discussing how to use the screening tool ... ..we made defensive choices [by choosing high cutoff level for being indicated at risk for LTSA] to minimize doing harm to healthy people. So deliberately we miss high risk people to minimize that risk [of conflicting damage to healthy people]. Yet, it is not a medicine, [ ... ] there is no real chance for damage ... ..”
[OP5]: “Yes, the advantage is that the results from research were good. If that wouldn’t be the case I would immediately quit like “What am I doing”. And it is not me alone who decides what happens during a consultation. We involve the employee in the process so I’m not taking over. So I’m not causing damage or harm ... ”
The other OPs were informed about the new approach during meeting days, which are held twice a year. These meeting days became the platform for instructions about how to perform the PS, and for monitoring the problems and attitude of the OPs when performing long term. The OPs outside the management (OP1-OP3) were initially enthusiastic about this new opportunity for prevention, but the sense of ownership diminished when time passed. OP3 highly valued the fact that the PS is evidence based, which according to OP3 is not often the case within occupational healthcare. For the other two [OP1 and OP2], the scientific results did not really make a difference. They miss adequate information that gives direct feedback about their efforts with regard to using the PS in every day practice;
[OP1] “ ... he [the manager] presented it in Italy I believe, the story that the ‘Balansmeter’ generated 35% sickness absence reduction. And then I think – but I notice the same feeling amongst my colleagues – that everyone has something like “we don’t see that in practice”. And it might be perfectly true, but for us it would have been nice if we had had more feedback in ordinary figures like right: seen 2000 people, normally the absence figures are such and such, for the group participating in screening, it is: ... .And that you can see that kind of figures.”
The manager of the OPs is well aware of this difference in perception;
[OP4] “Their [OPs outside the management] whole picture depends on the cases they have seen themselves. Yes I think their picture depends much more on that, than on an article in a magazine. You have to imagine: they are not ... I’m of course the great believer, followed by my assistant, because we were involved from day one with the development, the thinking, all pro’s and con’s we’ve thought about them a hundred times. They are basically the ones who have to carry out.”
This quote illustrates the difference in involvement amongst OPs. In line with this, keeping the OPs motivated requires quite a lot of effort;
[OP4] “ ... and then [over the course of time] you notice a waning of their motivation and belief. And then we try, time and time again ... standing in front of the group [during meeting days], sending quarterly information [assistant of manager], we keep them on track. We succeed, but if you don’t make these efforts, it fades away [the belief of the OPs].”
It might be concluded that the attitude of the OPs towards prevention in general is positive. They believe prevention is important for fostering employee health. Yet different efforts are necessary for switching the OPs from believers to owners of the PS. Knowledge transfer alone seems not enough for practicing the PS.
Discussion
Strengths and limitations of the study
We explored the experiences of OPs working in an OHS in The Netherlands who deliver a structured early consultation at a banking company with office workers identified at risk for future sickness absence by screening.
The results reported in this case study are restricted to the experiences of OPs in one OHS in The Netherlands. Occupational healthcare is strongly influenced by local policies and legislation, which might hamper extrapolation of these results to other OHS settings and other countries. However, increased risk for participation problems in office workers is applicable to a large part of the working population in western society given the magnitude of the service sector. Furthermore, we were able to address the perspective of employees only indirectly. The strength of this study is that our approach adds insight into understanding the barriers for screening strategies in the domain of work participation problems from the professional perspective. More than half of the OPs participated in the survey, providing a good representation of a stable team of OPs with regard to duration of contract (more than five years in the current OHS) and gender. We did not aim for saturation, interviewing only five OPs. The concordance of the comments from the open questions in the survey and the results from the interview strengthen our belief that the most important issues of the OPs were covered. In the literature to our knowledge, there are no other reports addressing a process evaluation about indicated prevention of LTSA.
Reflection on findings related to a theoretical perspective for process evaluation
For the evaluation of an implementation process, a variety of frameworks and models is available in the literature [9, 13–15]. We chose the model of Nielsen and Randall [15] to guide the interpretation of the results of this case study, because it focusses on occupational health, and interventions or strategies aiming to improve employee health and well-being. This three-level process evaluation model reflects on 1. “the intervention”, being the PS, 2. “the context”, being the interface of interests of stakeholders in which the OPs had to operate, and 3. “the mental models”, being the theories driving the behavior of the key stakeholders. Each level comprises several elements which are interactive (see Fig. 2), reflecting the complex and interlinked processes in the field of occupational health. The results will be discussed and interpreted following this format.
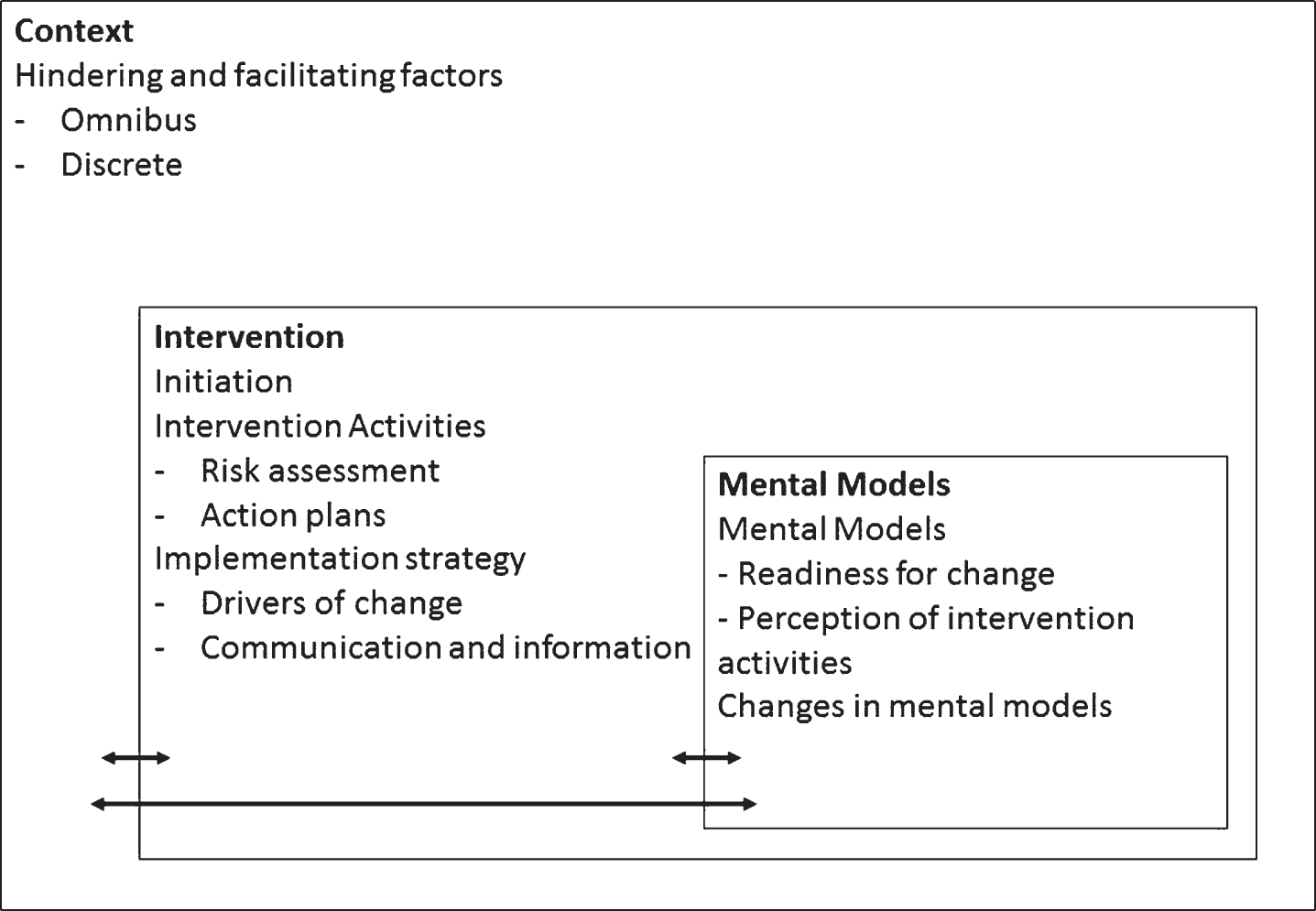
Model for process evaluation according to Nielsen and Randall [15].
The PS addresses a perceived need from the professional perspective, namely the increased prevalence of psychosocial and (mental) health problems amongst employees of the banking company, which caused sickness absence and reintegration problems.
Action plans for guiding the implementation process of the early structured consultation were not provided to the OPs. Information was provided during meeting days to all the OPs, by the manager and the assistant manager, both OPs themselves. Being involved from the very beginning in research and development of the PS, they can be considered the drivers of change in the implementation process. The other OPs, in their role as employees of the OHS, had to adopt the new way of working with their guidance. Given the initial enthusiasm about the PS when introduced, the intention to change seemed present. Yet ownership for the new way of working was not realized, which might be due to a perceived lack of adequate feedback on the efforts made by the individual OPs. The multifactorial model for predicting increased risk for LTSA is difficult to explain making risk communication challenging, since no clear starting point for risk can be communicated straight away to the employee (like in case of somatic risk factors, e.g. hypertension or cholesterol measurement).
Communication was mentioned as being the most crucial skill for performing well in the structured early consultation. Routine communication skills used for sickness absence counseling were perceived by the OPs as inadequate to overcome the unawareness on the employee side, causing attrition during the consultation. For health risk communication (the second step of the structured early consultation), appropriate training is necessary, since medical expertise and scientific knowledge alone are not enough to make health professionals equipped for communicating risk. Increasing early involvement of all OPs as key stakeholders and addressing risk communication skills through training, might improve implementation of the PS in future settings.
Context
Current OHS practice may have influenced the implementation of the PS e.g. through conflicting priorities (referred to as discrete context in Fig. 2). The PS is a new way of prevention targeting increased risk for LTSA on an individual level. Their routine job responsibilities mainly encompass socio-medical counseling of employees on sick leave (approximately 90% of time, 2/3 of actual sickness absence because of psychosocial problems). The PS is a relatively small part of their tasks and the targets agreed on with their clients are formulated in terms of tertiary prevention. Some OPs explicitly mentioned in the survey and during the interview that they were more occupied with lifestyle counseling. In the interviews, all OPs more distant from the management indicated preference for prevention on the level of the executives and the work environment.
According to Nielsen and Randall, the omnibus context can be explored by answering the question: “How did the intervention fit in with the culture and the conditions of the intervention group?” [15]. The structured early consultation does not match with their normal way of working. Working proactively triggered by the scores on the items of the screening questionnaire is unfamiliar because they are used to a reactive approach augmented by a help seeking question on the employee side. The unawareness on the employee side about factors concerning imbalance in private life, the psychosocial work environment, and (mental) health requires good communication on the professional side to enable problem confirmation and clarification. This is not in line with the current culture in medicine where a question for help on the employee side triggers a diagnostic process aiming for identification of a condition, disease or disorder through quantifiable measurements. All surveyed OPs are positive about a proactive workstyle. Training to perform the structured early consultation was indicated as desirable by over half of the OPs. Although they all want to prevent illness and intervene before sickness absence occurs, they are hindered by the culture of former education and current practice, in which the principle of ’doing no harm’ prevails.
The employees are also unfamiliar with the preventive role of the OPs. There is a lack of trust due to perceived lack of informational privacy, even when confidentiality is expressed during consultations. Heikkinen et al. state that because occupational health professionals have to work in close collaboration with employees and employers: this tripartite cooperation is susceptible to ethical problems of privacy [16]. In the interviews, only one OP expressed concerns about informational privacy. None of them mentioned problems with regard to dual loyalties when performing the PS in practice. This might be an indication for low ethical awareness, although ‘doing no harm’ is mentioned a couple of times during interviews as withholding them from action in the absence of a clearly delineated problem.
Mental models
Nielsen and Randall distinguish theories in use, which are the mental models that guide our behavior, from espoused theories, which are the attitudes and beliefs that we tell others to guide our behavior [15]. In general, the attitude and beliefs of the OPs about prevention are positive, as is their perception about the efficacy of the PS. Yet for actually delivering the PS in practice some hindering factors might be related to the mental model in use.
First, OPs indicated that working reactively guided by the presence of a clearly delineated problem was part of their former education. The switch to a proactive approach when delivering the structured early consultation (indicated prevention), in terms of guiding the awareness raising process in employees ignorant of their high risk status, was mentioned as being difficult and time consuming.
Second, the diffuse nature of the increased risk for LTSA appears to be a difficult starting point for the structured early consultation. Unlike for somatic risk factors, there is no biological substrate to communicate the high risk message to the employee straight away. Instead by means of a shared communication process with the employee, the high risk status has to be confirmed and further clarified. Only then can the risk for that specific employee be communicated, and thinking about what to target through early intervention can start, again on the basis of a shared communication process. This “lack of a suitable mold” makes the delivery of the structured early consultation difficult as mentioned in the interviews.
Third, knowledge and insight into psychosocial health problems is a prerequisite for adequately dealing with them. The unawareness of the high risk status on the employee side places high demands on the professional-employee interaction to accomplish the pursued outcome, prevention of LTSA. The attitude, knowledge and skills regarding psychosocial health literacy of both employee and professional determine the outcome of the communication process during the early structured consultation.
The dominant model in health care has been the biomedical model [17, 18] focusing on the diagnosis of a disease, disorder or injury. This paradigm is driven by pathogenesis and characterized by a mind-body dualism. It relies heavily on measures and tests of the disease process, and places a limited value on subjective reports of quality of life and wellbeing [18]. The administrative and declaration system used in the Dutch occupational health organizations implicitly supports, by its strong ICD-based coding, the use of biomedical consultation and handling. In the biopsychosocial paradigm as described by Engel [19, 20], the role of social and psychological factors in the onset, severity, and course of disease are stressed alongside attention for their influence on acceptance of the ‘sick role’ and entrance into the healthcare system. The patient-healthcare professional interaction is addressed as being important for the outcome of the treatment process and much more attention is given to interviewing skills and social and psychological knowledge in education of healthcare professionals. When relating these paradigms to our case study, the biopsychosocial paradigm seems a prerequisite for enabling the PS in occupational healthcare practice. Yet the aforementioned hindering factors for actually delivering the PS show the power of the biomedical paradigm, still dominantly present in education and healthcare practice.
Implications
OPs historically used to prevent work-related diseases and injuries related to physical and chemical exposures in the work environment. In the past, a reactive approach based on the biomedical model and intervening on the level of the work environment was an adequate workstyle for OPs. With the change from a manufacturing economy to a service economy in the last sixty years, nonspecific conditions related to stress have increased and have become the most important reason for sickness absence [2], requiring another mental model. In addition, on a societal level, the need for fostering health of employees over the lifespan emerged in the last decades, due to demographic and political reasons.
Stephenson and Richardson make a strong plea for fostering health of clients across the lifespan in healthcare in general, based on a client centered approach [21]. Client centered communication and health advocacy of professionals might be fostered by educating them in the International Classification of Functioning, Disability and Health (ICF) [22, 23], which is an operationalization of the biopsychosocial model. This can provide professionals with a language and with tools to acknowledge the context for understanding of individual’s functioning in their environment over time [21]. For the specific context of work and health, the elaboration on the ICF, described in the article of Heerkens et al. [24] is especially relevant. The value of using a biopsychosocial approach for early intervention from the start of a sickness absence period was confirmed by a study of Demou et al. [8], as was the use of ICF for enhancing a transdisciplinary approach [25].
Conclusions
Enhancing the implementation of indicated prevention in occupational healthcare practice needs to be addressed at different levels according to this case study. This can explain the intention behavior gap of the OPs for fully adopting the PS in practice. On the level of the context prioritization of prevention of LTSA next to the regular tasks of OPs must be facilitated further, by making prevention an explicit target, and addressing competencies involved like being a good communicator and health advocate in healthcare curricula and during in-service training. Furthermore, the biomedical model is still deeply rooted in the mental model OPs use, hindering the delivery of the structured early consultation. OPs need to be trained in problem clarification, risk communication, and client motivation from a biopsychosocial perspective. The unawareness of psychosocial risk factors on the employee side has to be investigated further. At the same time, problems in functioning or participation due to an imbalance of private life, the psychosocial work environment and (mental) health need to be normalized, to tackle the problem of stigmatization and labeling [26]. The use of ICF to describe (problems in) functioning complementary to ICD-10 (or other classification systems used for diagnostic labeling), might increase the awareness of occupational health professionals regarding the resources employees need to gain resilience and move towards health.
These developments are major challenges for OPs, raised in educational systems and healthcare practices embracing the biomedical model. ICF provides a neutral language to describe human functioning enabling monitoring of health over the lifespan. Reflecting on health using ICF might increase health agency at the client side and health advocacy on the professional side, enhancing the development of a trusting relationship. The potential role of the ICF as a common language to enable health professionals in making the biopsychosocial model the mental model in use instead of an espoused mental model must be further investigated.
Conflict of interest
None to report.
Footnotes
Appendix 1
Results Quantitative survey (N = 25, response rate 52% (n = 13))
| Item | N | Individual comments of OPs in open space to survey questions |
| 1. Performing PS in current OHS practice? | ||
| Yes | 11 | ‘Balansmeter’ office hour |
| No | 2 | |
| 2. A lot of experience with PS meanwhile? | ||
| Yes | 6 | |
| Reasonably | 4 | |
| No | 2 | |
| 3. How many employees with increased risk for LTSA monthly? | ||
| <1 | 3 | |
| 1 or 2 | 5 | |
| 3 or 4 | 3 | |
| >4 | 1 | |
| N.A. | 1 | |
| 4. What was your initial opinion about the PS when you first heard about it expressed as a school figure from 1 to 10? | 7.8 (7, 9) | Positive attitude towards prevention and PS and high expectations when PS was newly implemented |
| 5. What is your current opinion about the preventive strategy expressed as a school figure from 1 to 10? | 7.1 (4, 9) | Still positive but structured early consultation with employees is difficult/Early moment in time/ Expectations not met/Seen not enough cases/ Difficult to convince stakeholders |
| 6. Positive about proactive workstyle in relation to PS? | ||
| Yes | 12 | |
| Missing | 1 | |
| 7. PS valid from an ethical point of view? | ||
| Yes, in case of psychological complaints | 13 | Voluntary participation in PS, so ethical/Not ethical not treating employees at risk |
| Yes, in case of somatic problems | 12 | Voluntary participation in PS, so ethical/Not ethical when not treating employees who are at |
| Yes, in case of work related problems | 11 | |
| 8. Positive aspects of PS? | ||
| Monitoring of health by OPs | 7 | ‘Balansmeter’ indicates employees who do not attend the OPs office hour by themselves |
| Preventing depression through PS | 6 | ‘Balansmeter’ indicates employees who do not attend the OPs office hour by themselves |
| Preventing LTSA through PS | 10 | Own responsibility for individual choices is emphasized |
| No positive aspects | 0 | |
| Other | 1 | |
| 9. Concerns of OPs with regard to PS? | ||
| Mildness of the complaints | 3 | |
| Ethical concerns | 0 | |
| No question for help of employee | 2 | |
| Practical concerns | 1 | Motivating this group is difficult |
| None | 6 | |
| Missing | 1 | |
| 10. Concerns of employees, noticed by OPs, with regard to PS? | ||
| Yes | 4 | What happens with this information?/not in medical record?/Me a problem, why?/not wanting to acknowledge problem/Searching for problems when no complaints |
| No | 8 | |
| Missing | 1 | |
| 11. Training prior to implementation of PS? | ||
| Yes | 3 | |
| No | 8 | |
| Missing | 1 | |
| 12. Training desirable? | ||
| Yes | 7 | |
| No | 5 | |
| Missing | 1 | |
| 13. PS valuable addition to open office hour? | ||
| Yes | 12 | |
| No | 0 | |
| Missing | 1 | |
| 14. Can PS replace open office hour? | ||
| Yes | 0 | Open office hour is a different form of prevention/ employees must be enabled to take initiative as well/ dealing with other problems in open office |
| No | 12 | Open office hour is a different form of prevention/ employees must be enabled to take initiative as well/ dealing with other problems in open office |
| Missing | 1 | Open office hour is a different form of prevention/ employees must be enabled to take initiative as well/ dealing with other problems in open office |
| 15. Opinion OP about efficacy PS? | ||
| Positive | 8 | Evidence Based |
| Neutral | 3 | Doubts about the returns, sometimes it causes sickness absence |
| Negative | 1 | Low yields |
| 16. Recommending PS to other OPs? | ||
| Yes | 11 | |
| No | 1 | Low yields |
| Missing | 1 |