
Abstract
Keywords
Background
Paradigms influential in healthcare
Traditionally, Occupational Health and Healthcare are strongly rooted in the biomedical paradigm, which is characterized by a reductionist view, taking a symptomatic disease/disorder or injury as the primary point of departure for care. In the second half of the last century, when the predominant focus in Occupational Health was on chemical and physical exposures, this model proved valuable for determining causal relations and intervening on harmful determinants. In the last decades the focus of Occupational Health has shifted towards the impact of psychosocial factors on the health of employees, corresponding with a shift from a manufacturing based economy to one dominated by the service sector [1]. At the same time sustainable work participation and engagement of workers across the lifespan became of utmost importance, given the changing demographic and economic conditions, such as the aging of the workforce and increase in precarious employment due to the most recent economic crisis [2]. These developments augmented a call for professionals educated and trained to play a key role in implementing appropriate policies to foster health and the sustainable engagement of workers in organisations and companies.
Based on the work of Peterson [3] and Huber [4, 5] Fig. 1 represents the history of paradigms influential for the developments in thinking about health within the disciplines of medicine and healthcare, and important contemporary conceptualizations of health. The biomedical paradigm’s philosophical origin can be traced back three to four centuries [6].
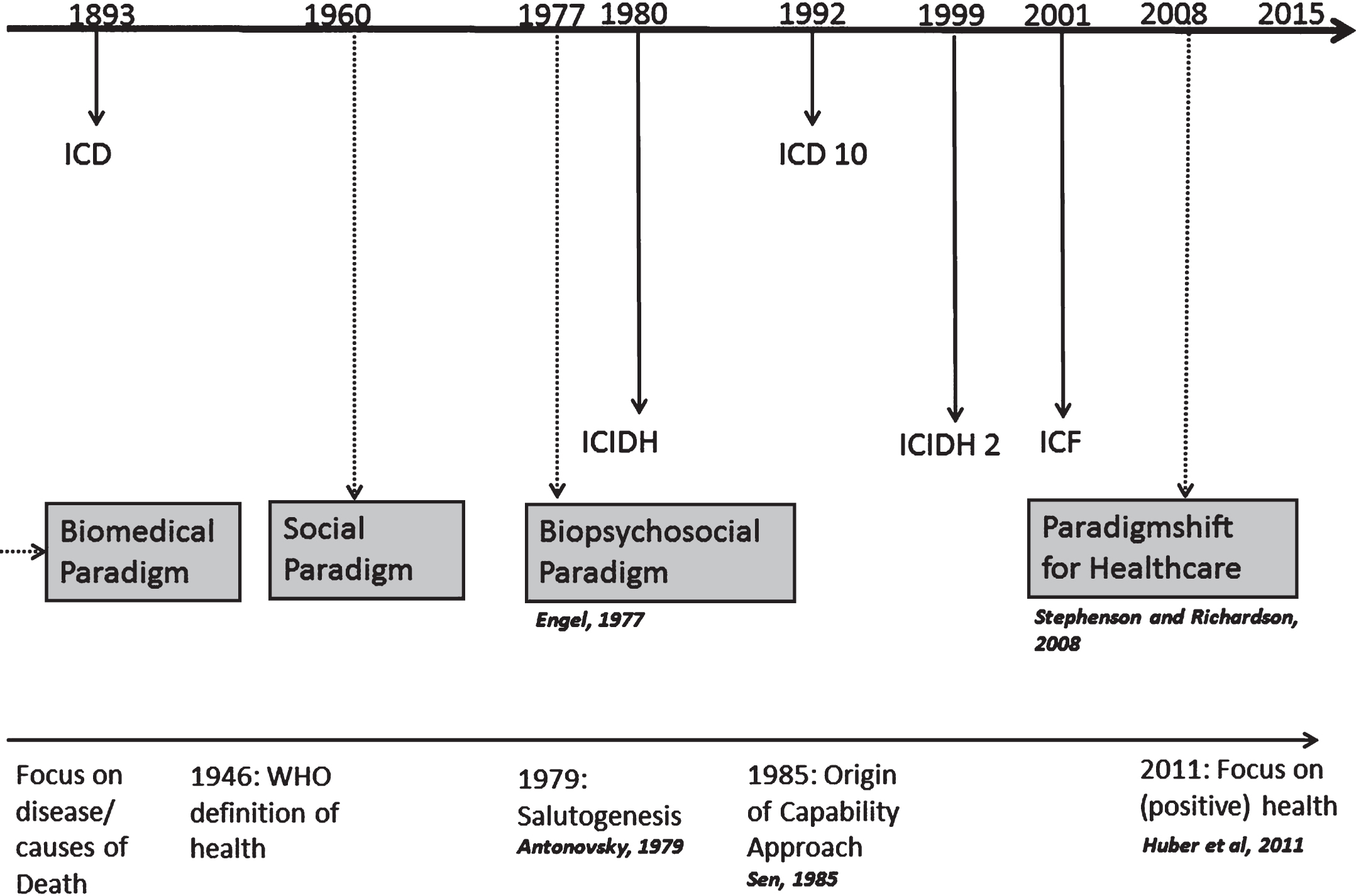
The history of paradigms influential for the developments in thinking about health and important contemporary conceptualizations of health.
The biomedical paradigm relates to an acute treatment process that first identifies a pathogen or cause of injury or other disease process, followed by selecting an appropriate treatment protocol for the condition identified [7]. It contributed to advances in science that helped researchers to better describe disease processes and related aetiology, allowing for rapid and effective response to the acute needs of people with a health condition. It relies heavily on measures and tests of the disease process and places a limited value on the experience of health and well-being [3]. Through operationalization in the International Classification of Diseases (ICD), from which the first version was released in 1893, and the 10th version is currently used [8], it still has a dominant position. The ICD provides an etiologic classification of health conditions (e.g. disease, disorders and injuries) related to mortality and morbidity. Ill health in the biomedical context is considered a personal characteristic that can be restored to normal by medical treatment focussed on the somatic domain. In this paradigm, health is merely the absence of injury and disease. The World Health Organisation (WHO) added a mental and social dimension to their definition of health in 1948 by describing health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. This definition appeared not very practical, but it did trigger thinking about health and how it could be operationalised.
The social paradigm came about as a reaction to the biomedical paradigm. This paradigm takes the opposite stance when reflecting on the ways of dealing with ill health and disability. The role of the environment in terms of systematic barriers and negative attitudes was identified, and exclusion mechanisms by society leading to inequality in the social and vocational areas were addressed. The influence of the social paradigm, being part of an emancipation movement rather than a scientific discipline, was more pronounced in terms of legislation [3]. Its relevance for science became visible when Engel published his article about ‘The need for a new medical model’ in Science (1977), postulating the biopsychosocial paradigm [6]. The biopsychosocial model is a synthesis of the biomedical and the social model and stresses the need to consider psychological, social and cultural factors when; considering variations in the expression of a disease, establishing the relationship with biochemical data, studying the onset, severity, and course of disease, studying the sick role and entrance into healthcare system, clarifying the discrepancies between biological abnormalities and treatment outcome, and when reflecting on the interaction between professional and client as part of the treatment outcome. In 1980 the International Classification of Impairments, Disabilities and Handicaps (ICIDH) was released, the first classification based on the biopsychosocial paradigm and the origin of a more holistic reflection on disability. It describes the consequences of disease on the level of the organs (impairment), the level of the person (disability) and the societal level (handicap) and it was meant for complementary use to the ICD. The absence of an operationalization of categories describing the influence of the environment and the negative connotation of the terms used in this classification (impairment, disability or handicap) kept the focus on disease, leaving a reflection on health subordinate. These and other critiques triggered the revision of ICIDH into ICIDH2 and finally the International Classification of Functioning, Disability and Health (ICF) in 2001 [9]. The ICF encompasses functioning as a universal human experience that can be conceptualized and classified from different perspectives (see Fig. 2 grey blocks): the perspective of the body (body functions and structures, including mental functions), the perspective of the individual (activities) and the perspective of society (participation). As visualised with the ICF diagram in Fig. 2, disability from this perspective involves problems in functioning at one or more of these levels respectively called impairments, activity limitations, and participation restrictions. Functioning can be influenced by a disease/disorder, but also by environmental factors (e.g. work environment, family life, organizational features) and personal factors (e.g. coping, self-efficacy, ability to use resources) [10]. Through adding a list of Environmental Factors and acknowledging the influence of Personal Factors (classification not defined yet by WHO) on functioning, the ICF shifts away from the medical model and facilitates the description of problems in functioning (disability), health, and health related states. Functioning is the core of the broad concept of health embraced by the ICF, and as such functioning is the lived experience of health [11]. As a consequence of the etiologic neutral language of the ICF to describe functioning, the mind body dualism diminishes, which might contribute to reduction of disparity in dealing with physical and mental disorders [3].
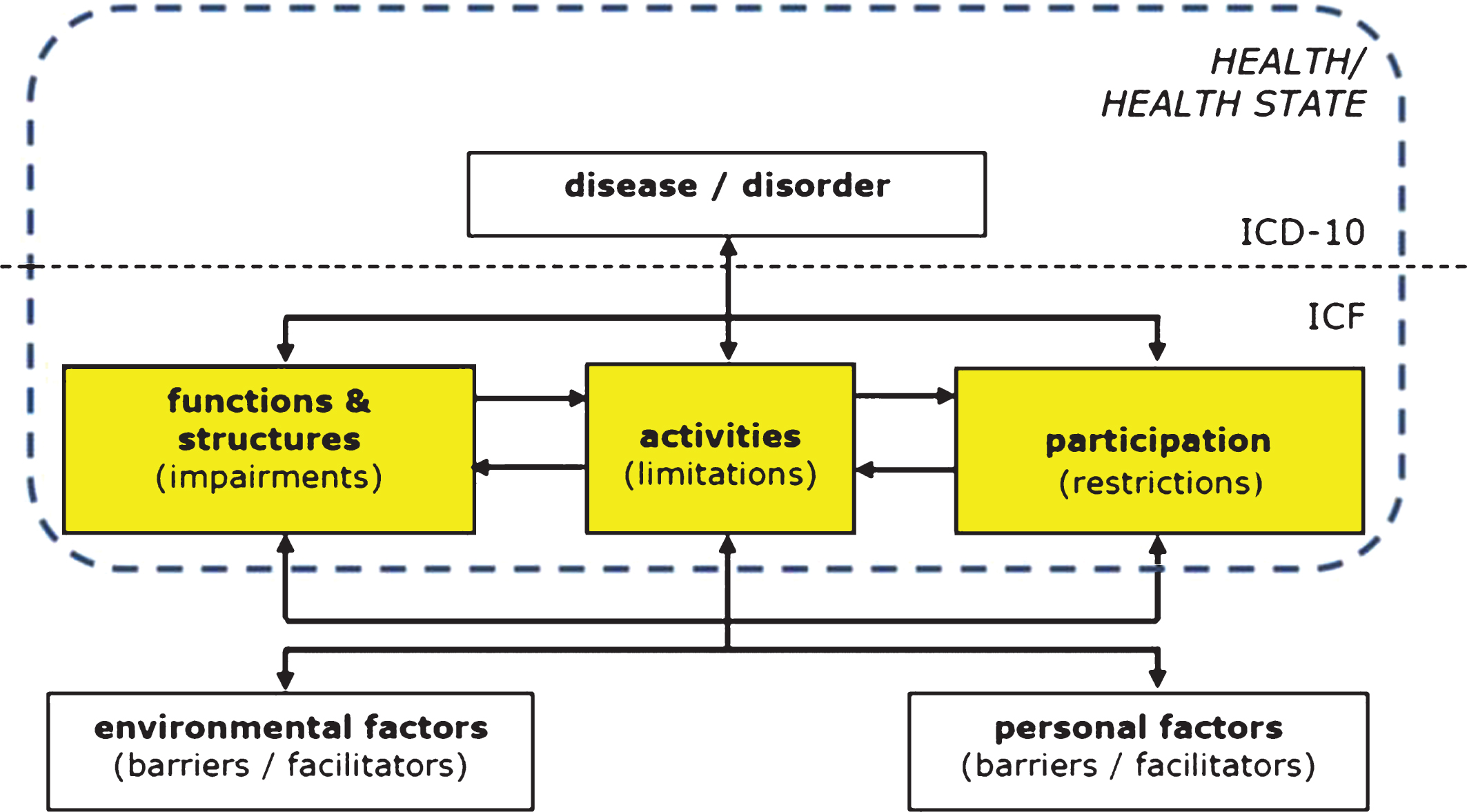
The ICF diagram visualizing a broad concept of health comprising functioning at three different levels (marked in grey).
The last paradigm shift mentioned in Fig. 1 is that proposed by Stephenson and Richardson [12], concerning a shift in focus from post diagnosis tertiary care towards fostering the health of clients across the lifespan, indicated for healthcare as a whole. They reconsider the ideas of Engel [6, 13] and subsequently broaden these ideas and the scope of healthcare, by stressing the need for monitoring clients across the lifespan through using a broad biopsychosocial assessment, adding to a client specific database over time. Client behaviour is the central key for monitoring by healthcare professionals and as such prevention gets an important position within this paradigm. Furthermore, they add to practice in terms of how to assess and monitor cases using a client oriented approach and how to revise clinical thinking of healthcare professionals through advocating the use of a broad evidence base.
In their view this means that teaching the biopsychosocial paradigm in healthcare curricula also affects the way evidence based practice is learned and trained. By teaching students how to value, appraise and generate evidence using methods from a wide methodological base, a client centred approach in which human functioning and behaviour are central, emerges. This leads to developing, assessing and legitimising knowledge drawn from a wide variety of sources to underpin client focussed problems, ultimately changing clinical decision making of (future) healthcare professionals, facilitating inter-professional care [12].
By giving the ICF a prominent role in realising these goals, healthcare professionals are given a language to operationalise their re-conceptualisation(s) of health, are guided in positioning of questions from professionals using a different methodological base in the ICF framework, are facilitated in a holistic assessment of each case taking into account contextual factors (being environmental and personal factors) and reactions on past influences for future interventions, and are legitimised in using a wide range of valued knowledge as the foundation of the evidence base for underpinning of clinical reasoning [12]. For monitoring clients across the lifespan, advocated by Stephenson and Richardson, a more dynamic concept of health is needed, like the one by Huber et al. [5]. They propose a new concept of health, serving contemporary healthcare to deal with the increasing burden of chronic diseases. Being a reaction to the definition of health formulated by the WHO in 1948, this new concept should “reflect the dynamic character of health, based on the resilience or capacity to cope and maintain and restore one’s integrity, equilibrium and sense of well-being” [5]. This resulted in the preferred view on health being delineated as “the ability to adapt and self-manage in the face of social, physical and emotional challenges” [5]. This view on health was operationalised by Huber and colleagues empirically, resulting in six dimensions of health: 1. Bodily functions, 2. Mental functions and perceptions, 3. Spiritual dimension, 4. Quality of life, 5. Social and societal participation, and 6. Daily functioning. These dimensions underscore the need for a broad concept of health, which is referred to as ‘Positive Health’ by Huber [14], to distinguish this approach from the definition of health as the absence of disease.
Reflection on health and how to monitor it is also needed within the field of occupational health given the challenges this field is facing, being the need of fostering health, productivity and sustainable engagement of workers throughout their careers. In the policy arena, this change is addressed frequently and extensively. Yet, in the professional domain, the developments are lagging behind.
In the Netherlands, legislation related to compensation for health related work participation problems shows a strong relationship with the evolution of the paradigms addressed in the former section. The biomedical model, with its long history and operationalization in the ICD, still has a dominant position. This paradigm was reflected in the first Social Security Act of the Netherlands, the Injuries Law of 1901, compensating workers for injuries incurred during work only (‘risque professionel’), according to the ‘Baremale principle’ (compensating wages for physical losses and death). While scientific disciplines enabling research like epidemiology evolved during the last century, occupational health shifted the focus from counting the dead and the injured, towards investigating the influence of chemical, biological and physical exposures as causes of morbidity and mortality. Under the influence of the Social Paradigm, the law in the Netherlands changed, adopting the ‘risque social’ in 1966. From then on also non work-related diseases or injuries were compensated for. At the same time, work disability benefits were related to wages through a system based on the loss of earning capacity (Invalidity Insurance Act) [WAO in Dutch]. The basic principle of the social insurance act continued to be ’risque social’ but more and more attention is paid to keep workers in the work force, making participation a key issue following the biopsychosocial paradigm and the classifications related to this paradigm (ICIDH, ICIDH2 and the ICF). This is reflected in the Work and Income Act [WIA in Dutch], effective as of 2006.
The latest development in legislation in the Netherlands is the ‘Participation Act’ (effective as of 2015), according to which persons with a disability and related restrictions in work participation will be reintegrated into the workforce, through the joined effort of local government and local employers, as directed by national policy. Occupational health professionals, operating on the intersection between the employer and the reintegrating employees, will be confronted with issues regarding functioning and work participation of this group.
Since the publication of the ICF in 2001, the environmental factors are addressed in reflecting on health in relation to activities and work participation. In 2004, Heerkens et al. used the ICF components to fill in the Van Dijk’s model of workload and work capacity, transforming the use of environmental and personal factors in relation to assessing workload and work capacity into a more operationalised conceptual model [10, 15]. In this special section Heerkens and colleagues elaborate on the article of 2004 by proposing a list of candidate ICF categories for describing relevant work related Environmental and Personal Factors in much more detail [16]. These candidate categories can be used together with the ICF manual [9] for a broad assessment of cases when evaluating health in relation to work.
Using a broad biopsychosocial assessment instead of an ICD based diagnosis as a starting point for evaluating a case seems to be desirable, especially in a field like occupational healthcare where functioning is the main outcome of interest and contextual factors situated in and outside the work environment are important for assessing the work demands and the work capacity [15]. However, healthcare professionals seem to be reluctant in taking up this approach as was one of the findings of the case study reported about in the article by de Brouwer et al. [17]. Therefore new directions in healthcare education are needed to change this. Stephenson and Richardson made a strong plea for starting the paradigm shift in healthcare from within the healthcare curricula by training of the skills relevant for a broad biopsychosocial assessment and training with the use of a broad evidence base to enrich clinical reasoning. The role for the ICF in this paradigm shift is fortified when a more precise description within a subfield is available, like the elaborations of Heerkens et al. [16] for work related environmental and personal factors. How these elements became the corner-stones of the new master program Work, Health and Career is outlined in the following sections. This new one year master program at the Maastricht University was started in 2013, and implemented the ICF as a frame of reference from the start. The ultimate goal of this curriculum is to deliver professionals capable of fostering sustainable work at all levels within organizations. The careers of these Work, Health and Career professionals can be within occupational healthcare organizations, human resource departments, or as policy makers. Being apprentices in the field of work and health, they can be the forerunners of the pursued paradigm shift.
Method
Preparations for the Master Work, Health and Career started in 2011. The target groups for this master are amongst others students with a university bachelor in health sciences, medicine, psychology, epidemiology or students who graduated from a university of applied sciences (e.g. human resource management, physiotherapy, occupational therapy). The fundamental elements for the general outline when creating this master program were: 1. the central theme was sustainable work, 2. the key outcomes were work participation in relation to work related activities and health and all determinants influencing these outcomes, 3. the core disciplines involved were Health Science, Behavioral Science, and Organizational Science, 4. the two important pillars to build on were the biopsychosocial paradigm and the evidence based practice tradition, 5. there should be a strong emphasis on skills training, and 6. the future professionals educated with this master program would be prepared for working in research and practice. Given these fundamental elements outlining the master program and inspired by the discussion paper of Stephenson and Richardson, the idea of incorporating the biopsychosocial paradigm into training evidence based practice skills emerged, which resulted in addressing and integrating these two important pillars extensively throughout the master program.
Teaching the biopsychosocial paradigm
The central role for the ICF to educate the biopsychosocial paradigm followed naturally, because participation and restrictions in participation belong to the core elements of human functioning, the central concept of the ICF. Although the biopsychosocial paradigm originates from 1977 [6, 13] its concepts are scarcely implemented in healthcare and healthcare curricula [18]. In this master program we deliberately chose to train students the biopsychosocial paradigm before they start work as an occupational health professional and adopt the biomedical paradigm as a frame of reference. The ICF is in two ways an operationalization of the biopsychosocial paradigm because it provides a language to describe human functioning taking into account the role of contextual factors (>1400 categories in the ICF manual [9]) and it provides a framework to visualize the broad concepts of health it captures (see Fig. 2).
Teaching evidence based practice
With regard to the other important pillar, the evidence based practice tradition, the aim is to train students to become a critical user of evidence as well as a skilled producer of evidence. For training evidence based practice skills, Maastricht University has adapted and further developed a teaching style based on an approach imported from New Zealand, the Critical Appraisal of a Topic (CAT). This format is used for teaching evidence based medicine to medical students. There is a lot of expertise in developing and teaching the CAT to medical students to develop their scientific skills [19]. In the medical curriculum students learn to make a CAT in the domain of diagnosis, prognosis and therapy following a patient contact observed during an office hour by going through the following steps: 1. describe the patient in a clinical scenario, 2. formulate a clinical question capturing an uncertainty with regard to clinical decision making, 3. search for an article in PubMed, 4. critically appraise the best article available at this moment, 5. present the relevant figures in the evidence table, 6. translate these findings to the patient by commenting on quality and applicability of the evidence, and 7. draw a conclusion about how to perform in clinical practice in the bottom line. This process can be characterized as deductive reasoning, where generalizations of scientific inquiry is applied on a few exact dimensions of a single client (reductionist approach), a way of thinking which fits within the biomedical and positivist methodological paradigm [12]. The choice of the methodological domains and the order in which they are offered (diagnosis, prognosis, and therapy) reflect the scope of the healthcare system, namely being focused on post diagnosis tertiary care. This scope, as well as the biomedical and positivist paradigm, is too narrow for the Work, Health and Career master program.
The two important pillars for the master program, the biopsychosocial model as the leading paradigm and the tradition of evidence based thinking about health and healthcare, are not easily combined. The tradition of evidence based practice strongly resides in the positivist way of thinking about science in which an objective researcher describes and analyzes phenomena in a merely quantitative manner. The CAT-tool used in the medicine curriculum [19], is a typical example of this way of reasoning. This can conflict with a more holistic and humanistic concept of health embraced in the biopsychosocial paradigm, in which the qualitative and experiential aspects of health phenomena are fostered [12]. The idea of valuing and using a broad evidence base proposed by Stephenson and Richardson enables the solution to bridge the gap between the two important pillars in the master program as visualized in Fig. 3. This augmented a creative process of reformulating the already very useful CAT tool.
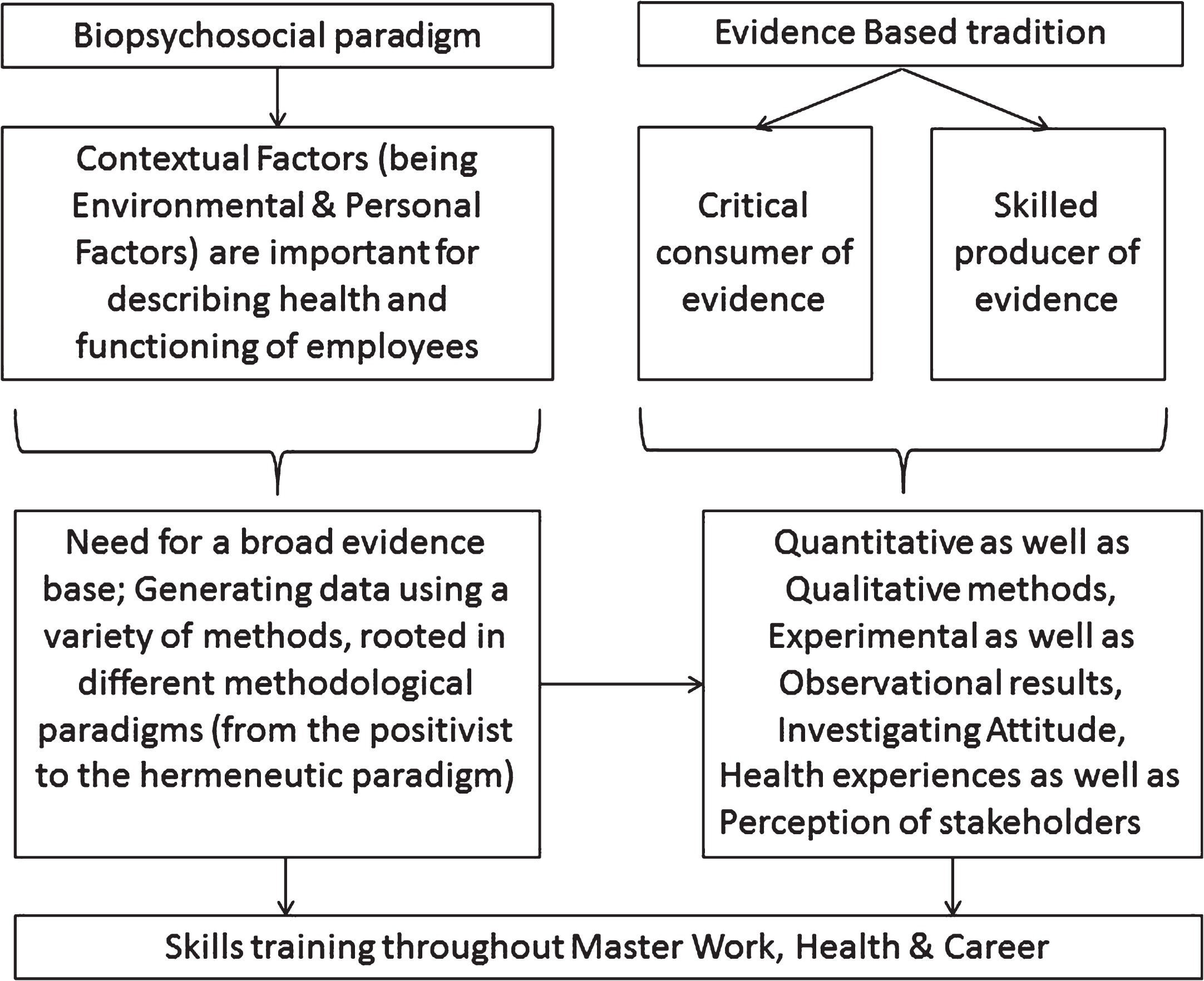
The broad evidence base connects the two important pillars in the master program Work, Health and Career.
The emphasis on skills training, and preparing the future Work, Health and Career professionals for research and practice, led to the decision to offer three longitudinal training trajectories during the one year curriculum: 1. training in the International Classification of Functioning, Disability and Health (ICF trajectory), 2. training in Evidence Based Occupational Health (EBOH trajectory based on the CAT format), and 3. Training in Communication & Intervention skills. Since the ICF was intended to be the frame of reference throughout the master program, the ICF trajectory became interwoven with both other training trajectories. In this paper only the ICF trajectory and the synergistic relationship between the ICF and the EBOH trajectory will be illustrated.
ICF trajectory
The ICF training throughout the Master Work, Health and Career program comprises standalone training sessions and extensive use of ICF skills in the EBOH trajectory as described in the next section. The arguments of Stephenson and Richardson [12] for using the ICF in healthcare curricula (indicated between brackets by making use of italicized text) are important for designing the ICF trajectory. This trajectory starts with introducing the biopsychosocial paradigm to the students, and placing it in the traditions of paradigms influencing healthcare and addressing important conceptualizations of health (as outlined in the background of this paper and summarized in figure 1). Students are encouraged by means of a lecture and subsequent training sessions to start thinking about what health encompasses and how to value health. They learn how to use the ICF categories from the ICF manual [9] and the elaboration by Heerkens et al. [16], to describe cases cross sectional using a representation of the Problem Solving Form [20], to describe and visualize the elements of functioning, and to describe the (work related) contextual factors in detail (acknowledging each case as a unique open system influenced by its particular context). By means of describing themselves in ICF terms at three different moments during the master program, awareness regarding the principle of universality (“describing functioning and disability with ICF applies to all people irrespective of health condition”) embedded in ICF instills. When cross sectional case descriptions are mastered the step towards representing cases in time through a sequential presentation of ICF plots is made. Interventions, not covered by the classifications in the ICF, can be plotted outside the framework to pinpoint where they are expected to influence the case (facilitating a holistic assessment of each case taking into account reactions on past influences for future interventions). Through the ICF framework they adopt a broad definition of health, comprising health status and functioning. As outlined in Fig. 1 the concept of salutogenesis by Antonovsky [21, 22], the capability approach of Sen [23] as applied to work and health [24], and the preferred view on health as proposed by Huber [14] are addressed and worked with in the ICF trajectory, for shifting the focus towards more holistic conceptualizations of health (facilitating the re-conceptualisation of health). Furthermore, the linking rules defined by Cieza et al. [25, 26] are taught to students to facilitate the necessary skills to position measurement instruments and all kind of data which can be part of the broad evidence base (from laboratory test to client narrative), within the ICF framework (legitimising a wide range of valued knowledge as the foundation of the evidence base for underpinning of clinical reasoning). The ICF REHAB sheet as proposed by Finger et al. [27] is used in one of the ICF training sessions to facilitate inter-professional communication simulated by students during a role play centred around a cardiac (work) rehabilitation case. The students in the role play interdisciplinary team meeting and ask questions and formulate goals during this training from their own frame of reference, yet the common language ICF provides enables them to prioritise problem areas and tailor interventions to the patient’s needs (facilitating positioning of questions from professionals using a different methodological base in the ICF framework).
Furthermore, ICF based tools for enhancing an ICF based needs assessment and ICF Core Sets are introduced in training sessions where applicable.
EBOH trajectory
To boost the implementation process of the ICF within this curriculum, the training was grafted onto the other important pillar within health sciences and medicine of working evidence based. All scientific education healthcare programs teach and train professionals the skills for learning how to think and act in an evidence based way. The Critical Appraisal of a Topic (CAT) was used for training the skills needed to enhance an evidence based work style [19].
The choice for the CAT format when training evidence based practice skills is a deliberate one and motivated by the linkage of practice and scientific thinking. This makes the training program more attractive for students because how to use these skills in a future job is illustrated during schooling. The CAT format at Maastricht University [19] comprises of seven components as described in the method section. Elaboration of each of these components makes the CAT tool a better fit with the biopsychosocial paradigm through incorporating the biopsychosocial paradigm into the assessment and scientific reasoning skills of students. In Table 1 a comparison between the traditional biomedical oriented CAT and the CAT tool fitting the biopsychosocial paradigm is given, and how skills learned in the ICF trajectory mediate this transformation is indicated in the central column of this table.
CAT tool shifts paradigms from biomedical perspective to biopsychosocial perpective (ICF skills playing a mediating role are presented in the second column)
CAT tool shifts paradigms from biomedical perspective to biopsychosocial perpective (ICF skills playing a mediating role are presented in the second column)
By implementing the changes described in Table 1 in education and training, a new CAT tool emerges embracing the biopsychosocial perspective. The scope of a ‘classic biomedical CAT’ is (most of the time) a situation describing a consultation involving a healthcare professional, a client, and a health condition (micro-level). When training CAT from a biopsychosocial perspective a broader scope is warranted. The importance of Environmental and Personal Factors in an ICF based assessment requires more levels to be acknowledged, because Environmental Factors are often formulated on meso- and macro-level. For example, the meso- as well as the micro-level can be investigated or intervened on when an employer is struggling with an issue on a specific department such as frequent short term sick leave of employees as related to work culture. Or for another example, a certain group of professionals might show a high risk for a condition, such as a high rate of moral distress amongst intensive care nurses. Macro-level influences like legislation and economic depression have to be taken into account as well, if in a certain company or sector a lot of jobs are at stake impacting the health state of employees. Furthermore, future professionals of Work, Health and Career have to deal with many stakeholders, e.g. employers, employees, human resource professionals, occupational physicians, psychologists, and company counselors. For investigating the influence of contextual factors on work participation and for addressing the experiences and attitudes of stakeholders with regard to sustainable work issues, a broad evidence base is needed to generate a valid picture of all issues at stake. Moreover, the disciplines involved (e.g. health science, behavioral science, organizational science) engage themselves with different methodological paradigms. Therefore a broad evidence base addressing quantitative as well as qualitative methods, experimental as well as observational results, investigating attitude, and health experiences as well as perception of stakeholders have to be trained (also see Fig. 3).
A broad biopsychosocial assessment as the point of departure for analyzing each case and the use of a broad evidence base are the most important differences with the ‘classic biomedical CAT’, in which the dominant paradigm on which clinical reasoning is based is the positivist paradigm. Adding these skills to keep a holistic view on a case enriches all components of the CAT to the Bottom Line. The CAT format is visualized in Fig. 4.
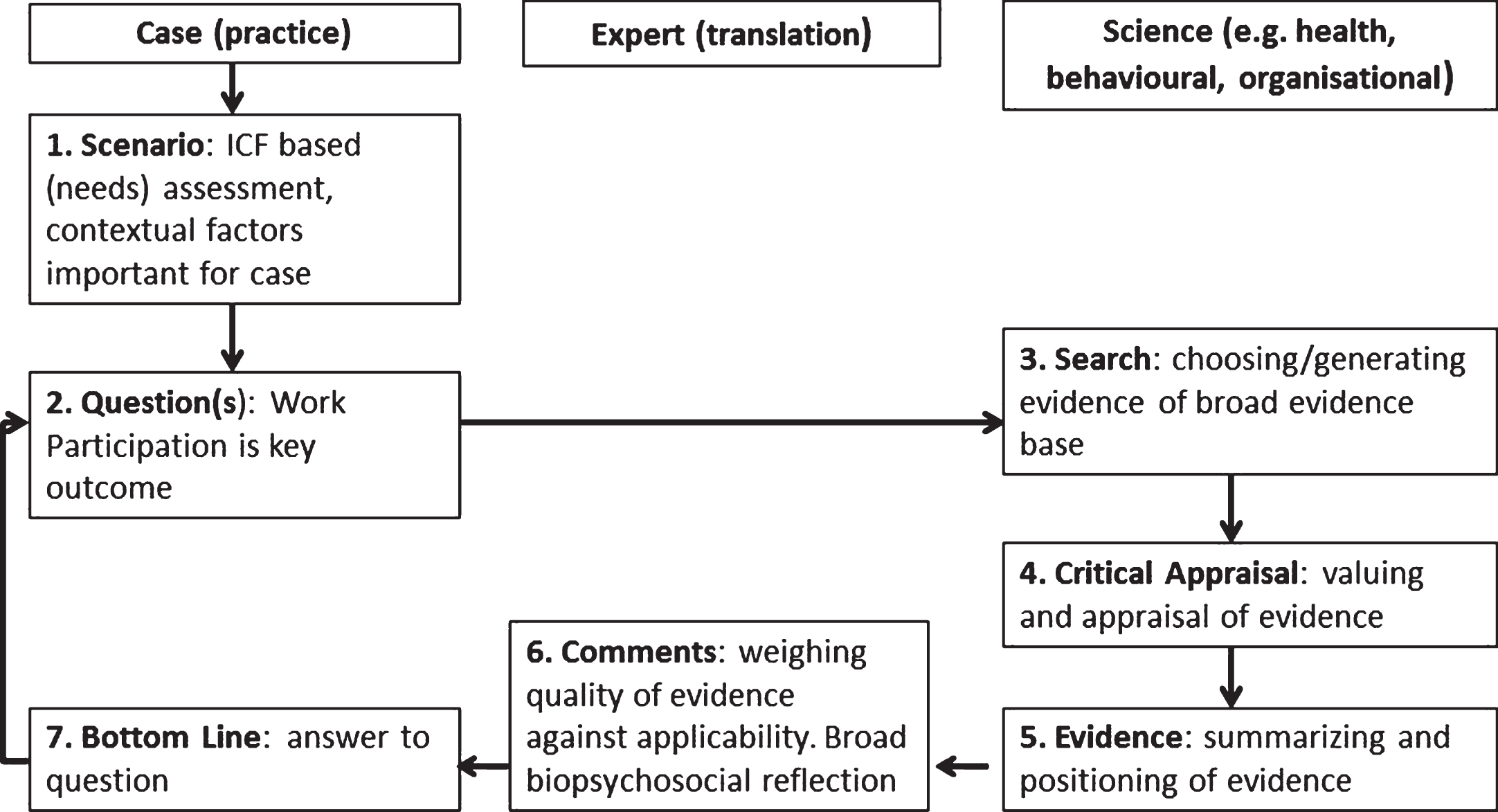
Flow chart visualizing the CAT format.
In the Work, Health and Career program, students come across a wide methodological base which they learn to use, value and generate, to substantiate a CAT. For example students not only learn to critically appraise articles in the domain of etiology, intervention, and implementation research, but they also learn to conduct an ICF based interview (interviewing fellow students to monitor work/study-life balance and interviewing a person with dyslexia about the influence of this condition on work related functioning), and they participate in a moral case deliberation session investigating values and norms of stakeholders with regard to a specific case. Use of sources of evidence gathered in the course of monitoring (dossiers or well-designed registration systems), should be included in the training for safeguarding a longitudinal reflection on cases in practice for future intervention planning if possible. Students train the latter by means of monitoring themselves in ICF terms at three consecutive moments in time throughout the curriculum. Formulating an advice with regard to one of these timeframes using a tool for accumulating an ICF based needs assessment for one of their fellow students simulates intervention planning in practice. Writing a narrative about their own lived experience of health and relating their experiences to contemporary conceptualizations of health as outlined in Fig. 1, is another example of training the use of methods from a wide methodological base. An impression of the operationalization of training the use of a broad evidence base in the master program Work, Health and Career is given in Fig. 5. Furthermore, training sessions outside the two trajectories described above, lectures and tutorial group meetings also add to educating students in the use, valuing and application of a broad evidence base.
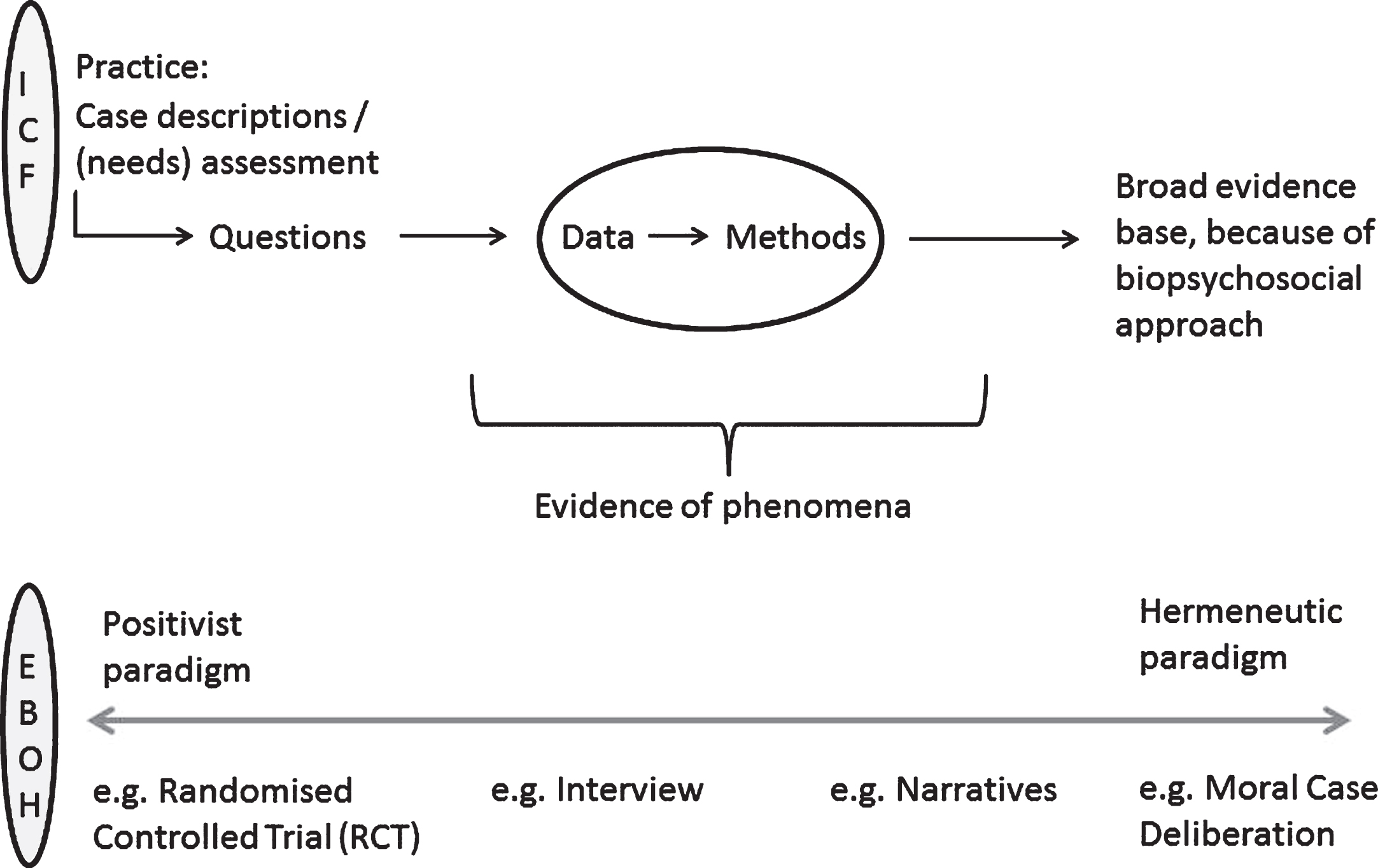
Use of a broad evidence base is indicated when the biopsychosocial paradigm is educated (inspired by Stephenson et al., 2008 [12]).
A contribution to realizing the paradigm shift described by Stephenson and Richardson is pursued by integrating ICF skills in the CAT and through teaching and training the essence of a broad evidence base. Students get familiar with deductive as well as inductive scientific reasoning with regard to cases and learn the value of monitoring cases over time. The expected results from this approach are a shift from the biomedical towards the biopsychosocial paradigm, a reductionist approach towards a more holistic view on cases, a reactive way of working towards a more proactive work style, and using a merely quantifiable evidence base towards using a broad evidence base.
The master program Work, Health and Career is a one year international master program of six half-time modules of eight weeks (six European Credit Time System points, ECTS points) and a full-time research period of 16 weeks (24 ECTS points). Both the ICF trainings trajectory and the EBOH trajectory are positioned in three consecutive modules: (i) Determinants of health and labor participation, (ii) Strategies for health protection, disease prevention and re-integration into work, and (iii) Occupational health management. About 30% of the time (six ECTS points) is directly spent during these modules to these trajectories. The trainings trajectories also account for 30% in the assessment of these modules. Moreover, students are encouraged to apply this knowledge in studying casuistry in these three modules as well as in their research during the thesis period.
The ultimate goals of the ICF/EBOH trajectory are to influence conceptual thinking about health, to learn how to use ICF as a language, to learn to work with ICF based tools, and to use ICF for occupational practice in an evidence based way.
The effects of the training with the trajectories will be evaluated and monitored with regard to knowledge, skills, and attitude of the students by particularizing the instrument of Reed [7] within the occupational health context. Results are not available yet, but will be published in the near future.
Discussion
This paper addresses the need for a paradigm shift from post-diagnosis tertiary care towards maintenance and promotion of health across the lifespan in health care in general, and in occupational health care specifically. Work and Health is a relevant topic for medical and other health care disciplines because working with a (health) condition becomes more prevalent given the societal development stressing the need for labor participation.
This paradigm shift may be facilitated through education of the ICF [12] to (future) occupational health professionals. Bornbaum et al. argue that ICF’s application in education can bring about a cultural change in healthcare, but also mention that, based on their review about ICF in health education, it is difficult to determine to what extend ICF has truly informed health education at this moment, and that teaching ICF is only just gaining momentum in healthcare curricula [18].
We developed an occupational health curriculum encompassing the ICF-framework, because this classification and the biopsychosocial paradigm it is based on facilitate the redefinition of health, while taking into account work related environmental and personal factors. As such, the elaboration on the contextual factors in the ICF as developed by Heerkens et al. [16] is vital to enable a thorough description, and subsequent needs assessment for cases in the field of work and health. Recent studies underscore the importance of elaboration on the contextual factors in the ICF. For example a recent study of Martins et al. showed the importance of personal factors like self-efficacy and personal attitudes for the work participation of people with a disability, alongside the importance of environmental factors like assistive technologies [28]. Recently, Finger et al. also indicated the need for more detailed categories in ICF with regard to work participation when going through the process of developing an ICF core set for vocational rehabilitation [29]. Moreover, the linking of ‘positive health’ defined by Huber and colleagues [30, 31] to the ICF, shows that the ICF categories enable the monitoring of a broad concept of health perceived as important by a broad range of stakeholders, especially so when personal factors are defined as well. Therefore the elaborations on the Environmental and Personal Factors by Heerkens and colleagues are an asset for the whole field of occupational health.
In the curriculum described in this paper two intertwined longitudinal trainings trajectories are offered: an ICF trajectory and an Evidence Based Occupational Health (EBOH) trajectory. The goals of the ICF trajectory are to influence conceptual thinking about different concepts of health, to learn how to use ICF as a language, to learn to work with ICF based tools, and finally to use ICF for occupational practice e.g. when monitoring participation of employees over time. The importance of the latter was also emphasized by Demou and colleagues who showed the proper reporting and recording of participation problems over time to be one of the success factors of their new sickness absence management service program [32]. The goal of the EBOH trajectory is to provide students with a life-long-learning tool (CAT) facilitating evidence based practice in the field of work and health, since the CAT tool sharpens scientific thinking of these future professionals with regard to practice based problems. The students, of whom most are not involved in a real work environment at that moment in time, can be motivated to learn the language captured within the ICF by using the CAT as a vehicle for applying the skills learned in the ICF training. Through intertwining of the CAT with the EBOH trajectory, the CAT becomes a more feasible tool for all disciplines in which the contextual factors strongly influence health and participation outcomes like in rehabilitation settings, psychiatry, and nutritional science.
The ultimate goal of this newly developed master program is to train professionals who can contribute to sustainable employment where individuals are productively employed in jobs that sustain psychological and economic well-being over time as well as balance the diverse interests of employers, workers and families. By using the ICF as the backbone of the master program and the intensive ICF/EBOH trainings trajectories, we hope and expect that the alumni of this master program are able to use the ICF in occupational practice to facilitate the paradigm shift towards to maintenance and promotion of health across the lifespan. The professional profile of the master students finishing this master program is, however, based on theoretical more than practice based assumptions. Although the profile is in line with the emerging need for more sustainable employment, it can only be assumed that the acquired knowledge and skills will match with the contemporary and future issues within organizations. Given the changing nature of participation problems in the last decades, the need for a psychosocial approach has become more and more urgent [1, 33]. Yet unlike for example in medicine [34], to date there is no competency profile for professionals raised in this master program, making our learning objectives and competency training more difficult to be benchmarked. Follow up of our alumni with regard to settings and professional profiles might reveal competency profiles that might be used as a benchmark and give leads for further tailoring of knowledge transfer and competency training trajectories to practice [34].
Through combining the ICF trajectory with a trainings trajectory in Evidence Based Occupational Health, we were able to incorporate the biopsychosocial paradigm into the assessment and scientific reasoning skills of students. In this way, we both conceptually and didactically combined the best of two worlds. A limitation of this approach is the need for trainers experienced in both, teaching evidence based practice skills (CAT-tool) and teaching the ICF. Also the amount of time necessary for training and practicing these skills by students is quite extensive, which might not be an option in all curricula. Our students learn to use the ICF language up to the fourth level. This level of precision might not be feasible for professionals already engaged in a busy professional practice nor for students and professionals from other disciplines involved in fostering sustainable working lives of employees (e.g. psychologists, occupational health physicians, general practitioners, policymakers, HR managers). Therefore, interdisciplinary communication based on the ICF language might be utopian for the time being. Using the biopsychosocial paradigm explicitly through propagating the ICF language might even cause resistance or might work out counterproductive amongst professionals not familiar with ICF. However, students from this master can be the facilitators in the implementation process of the biopsychosocial paradigm in current (occupational) healthcare. Tools based on the ICF can be an adequate starting point too, for disseminating the biopsychosocial paradigm in these healthcare practices.
In this master program we deliberately chose to train students before they start work as an occupational health professional. We think students are more open for this paradigm shift because they have not worked in the system in which biomedical reasoning is highly prevalent. Each cohort of students of this master program will be evaluated and monitored with regard to knowledge, skills, and attitude. These evaluations will reveal whether the students are capable of contributing to the proposed paradigm shift in occupational health care. The ICF training described in this paper will also be offered as a ‘stand-alone’ trainings trajectory for occupational health physicians and other occupational healthcare professionals. Evaluation of this ‘stand-alone’ trajectory with regard to knowledge, skills and attitude of the participants may indicate whether it is possible to change the attitude of experienced occupational healthcare professionals raised in the biomedical tradition, towards the biopsychosocial approach through ICF training. The evaluation of the program and the stand alone trainings trajectory will give indications of whether the trainings intensity is sufficient.
Given the clear conceptual model and the practical tools, adapted to present-day developments in society and healthcare, the curriculum described in this paper can be an exemplary case for other curricula in occupational healthcare including the curricula for occupational physicians, insurance physicians, (occupational) nurse practitioners, occupational therapists, company counselors and psychologists. Moreover, medical curricula and curricula for other healthcare professionals could benefit from an ICF based approach
A serious barrier for the proposed paradigm shift in Occupational Health care may be the extensive use of the ICD based classification codes rooted in the biomedical tradition. These codes are now used in communication between professionals and are also the basis for billing in occupational health care and health insurance. Furthermore the ICD codes still play a dominant role in the assessment for permanent work disability benefits. A condition for the proposed paradigm shift in occupational healthcare practice is that the ICF is used complementary to the ICD codes for communication between professionals and is implemented in the systems for monitoring clients.
Although there is still a long way to go, we are convinced that ICF based curricula in occupational health care can contribute to the paradigm shift from post-diagnosis tertiary care towards the maintenance and promotion of health across the lifespan in occupational health care. With this paper we hope to initiate an inter-professional dialogue on the use of the ICF in curricula, by sharing the experiences from the Work, Health, and Career program.
Conflict of interest
None to report.