
Abstract
BACKGROUND:
Worldwide, approximately 350 million people are currently employed in the construction industry.
OBJECTIVE:
To determine the prevalence, pain characteristics, and associated risk factors for musculoskeletal disorders (MSDs) among construction workers in Pakistan.
METHODS:
This study was a cross-sectional survey conducted from February to August 2019 among 666 construction workers. The data were collected using a questionnaire consisting of 4 sections: demographic information, a numerical pain intensity rating scale, a Nordic questionnaire to report prevalence, and pain characteristics. SPSS was used for data entry and analysis.
RESULTS:
The mean age of the construction workers was 34.49 years. Participants who reported pain were 397 out of 666 and 269 were those who reported no pain. The 12-month prevalence of pain among construction workers in more than one body area was 89% (n = 591) and the 7-day prevalence was 52% (n = 343); lower back pain was the most common type of pain with a 12-month prevalence of 27% (n = 180) and a 7-day prevalence of 17% (n = 112). Regarding the characteristics of the pain, 26% (173) of the workers suffered pain occasionally, 27% (180) participants had pain for≤2 hours per day, and 32.9% (219) had dull pain. Moreover, a significant relationship was found (p < 0.05) between MSDs and age, lifestyle, work experience, smoking habits, and absence from work.
CONCLUSION:
Musculoskeletal pain is highly prevalent, with lower back pain being the most commonly reported type. Absence from work and disability in performing normal daily activities have been reported as consequences of musculoskeletal pain. Moreover, this study underscores the importance of targeted preventive healthcare measures for construction workers.
Introduction
Approximately 350 million people are currently employed in the construction industry worldwide [1]. Construction is one of the world’s steadily growing industries, both in developed and developing countries. Construction workers work under more physically demanding requirements than the general population and are constantly exposed to environmental and climate demands [2]. There is evidence that work-related musculoskeletal disorders (WMSDs) are major occupational health problems that lead to work-related disabilities, particularly among workers in the construction industry [3, 4]. WMSDs impose financial burdens on construction workers and their families, employers, and society, causing losses in income and productivity as well as medical expenses [5]. WMSDs have been reported worldwide among construction workers. One study found that construction workers specializing in wall plastering reported complaints of back, shoulder, wrist, and elbow problems as a result of high levels of repetitive work in uncomfortable postures [6]. Similarly, back pain has been reported as a serious work-related musculoskeletal problem and was responsible for sick leave and hospital visits in pipe workers [7]. In addition, another study by Wang et al. reported that the leading cause of WMSDs in construction was overexertion, and back injuries accounted for more than 40% of WMSDs in construction workers [8].
The identified risk factors for WMSDs include not only dangerous equipment, machinery, and situations, but also damaging factors that may be physical (e.g., noise, vibration, and thermal stress) [9], or ergonomic (e.g., awkward posture, inadequate rest breaks, monotonous work, standing for long periods of time, manual handling of tasks such as lifting, carrying, pushing, and pulling, improper body positioning, exerting excessive strength, and repetitive movements) [10, 11].
Safety in the construction industry is seen as an important issue. This is especially true in developing countries like Pakistan, where safety is a major concern due to the lack of implementation of workplace safety laws [12]. In developed countries, well-designed guidelines and policies are implemented to protect workers. However, workers in developing countries are more vulnerable to health damage, mainly due to the unsatisfactory quality of the work environment and health facilities. Moreover, construction workers in developing countries perform risky work for scant wages and face numerous physical and psychological problems. In addition, construction work is intrinsically physically demanding; consequently, workers are predisposed to the risk of injury [9, 13].
Pakistan, a developing country, is currently seeing strong growth in construction activity. Thus, the construction industry is a major contributor to Pakistan’s gross domestic product and employs around 9% of the total workforce [14]. Unfortunately, existing national safety regulations do not apply directly to the industry. The absence of such rules adversely affects safety enforcement, leading to more vulnerable conditions. Existing on-site inspection services are insufficient in identifying or assessing occupational hazards, and accident reporting and recording systems are not functional [15, 16]. According to the Occupational Safety and Health Administration (OSHA), contact force, repetition, awkward positioning, compression, high temperatures, and vibrations are factors that increase the chances of musculoskeletal injuries. Redesigning worksites and choosing appropriate tools can prevent serious injuries [17]. Moreover, early recognition and treatment of musculoskeletal pain (MSP) and its related problems may lead to faster recovery and prevention of disabilities [18]. Most studies on MSP and related disorders have been limited to computer-based office workers, bankers, students, teachers, and health workers in the Pakistani population [19–22]. To our knowledge, there is a lack of literature on the prevalence, characteristics, and consequences of MSP in Pakistani construction workers. The aim of the present study was therefore to measure the prevalence and determine the characteristics and consequences of MSDs in Pakistani construction workers.
Methods
Participant recruitment
Construction workers were selected from six randomly selected construction sites in Faisalabad city. The site managers were approached by researchers to involve the participants in the study. The site manager therefore asked the participants to take part in study. The participants were recruited if they were males between the ages of 18 and 60 years, had worked in the construction industry for at least a year, and volunteered willingly to participate in the study. Construction workers with any history of physical trauma due to an accident or chronic pain before joining the construction industry, or who suffered from radiculopathy, myelopathy, or any disability, were excluded from the study. Written consent was obtained from every participant before data collection. Approval to conduct the present study was obtained from an ethical review committee at Riphah International University (RCRAHS/REC/201).
Data collection
The data were collected from participants through face-to-face interviews using a previously validated questionnaire consisting of the following different sections: 1) demographic information, 2) a numerical rating scale for assessing pain intensity [23], 3) a Nordic Musculoskeletal Questionnaire (NMQ) [24], and 4) pain characteristics. The principal investigator (PI) and two additional investigators who were physical therapists took the survey forms to the selected construction sites, interviewed workers directly, and recorded their answers on the survey form during the workers’ break time.
Physical, personal, and occupational factors
Demographic variables such as age, height, and body weight were recorded as self-reported by the participants. Furthermore, the investigators asked the participants about their personal information. Participants were asked about their smoking habits to classify them into the “current smoker,” “ex-smoker,” or “non-smoker” categories. They were asked about their engagement activities to allow the investigators to classify them as “sedentary” or “active”. Workers who ran for more than 3 miles per day at the same pace or engaged in physical activity of equivalent intensity and quantity were considered to be active. To obtain more information on their occupations, the participants were asked about their number of years of experience, the hours worked per day, the duration of breaks, and their construction work specialties. Moreover, participants were asked to reply “Yes” or “No” regarding their use of protective equipment while on duty. Lastly, participants were asked to report the number of days they had taken off due to musculoskeletal problems.
Screening for musculoskeletal disorders
This study focused on determining the prevalence of work-related MSP. Therefore, screening for work-related MSP in construction workers was carried out by the PI and two investigators using the NMQ [24]. The NMQ is commonly used for evaluating musculoskeletal symptoms and the 7-day and 12-month prevalence of pain in nine main body regions, including the neck, shoulder, upper back, elbows, wrists/hands, lower back, hips/thighs, knees, and ankles/feet [25].
Pain Characteristics
The investigators documented the type of pain, intensity of pain during the working hours and at rest, duration of pain, and treatments received due to musculoskeletal conditions among the construction workers.
Data Analysis
Statistical analysis was performed using SPSS version 22 (IBM Corp, Armonk, NY, USA). Descriptive statistics, including frequency, mean, and standard deviation of demographic data, the presence of musculoskeletal symptoms, affected body parts, types of pain, and types of treatment were recorded. The Chi-squared test was used to assess the association between MSP and associated personal, physical, and occupational risk factors. Results were considered statistically significant if p < 0.05.
Results
A total of 1,000 construction workers present during the data collection period were interviewed at the selected construction sites; however, 334 participants were excluded based on the pre-defined inclusion criteria. Thus, the study participants were 666. Participants who reported pain were 397 out of 666 and 269 were those who reported no pain.
The participants had a mean age of 34.49±10.48 years, mean height 167.54±10.72 centimeters, and mean weight 63.12±12.41 kg. Additionally, 2.7% [18] of the participants had a sedentary lifestyle, and 97.3% (648) were active. (Table 1).
Demographic information of participants (n: 666)
Demographic information of participants (n: 666)
The 12-month prevalence of pain was 89% (n = 591) and the 7-day prevalence was 52% (n = 343) among construction workers who reported pain in more than one body area. The findings of current study revealed that overall 415 (62%) of the participants experienced difficulties in performing normal activities. 112 (17%) had complaints in the lower back area, and 46 (7%) had complaints in the wrists/hands in the past 7 days. (Table 2).
7-days and 12-months prevalence of musculoskeletal pain among construction workers who reported pain in more than one body area
With regard to the average level of pain during activities, 11% (74) of participants had mild pain, 37% (245) had moderate pain, and 11% (74) had severe pain. While at rest, 32% (210) of participants had mild pain, 14% (94) had moderate pain, and 2% (16) had severe pain (Fig. 1). With regard to the characteristics of the pain, 26% (173) of the workers had pain occasionally, 27% (180) had pain for less or equal to 2 hours per day and 141 (21.2%) had pain for > 2 hours. Similarly 44 (6.6) had pain for 1 to 7 days, and 4.8% [32] had pain more 1 week. 32.9% (219) had a dull ache, and 29. 4% (196) reported having taken sick leave due to WMSDs for≤15 days per year. (Table 3).
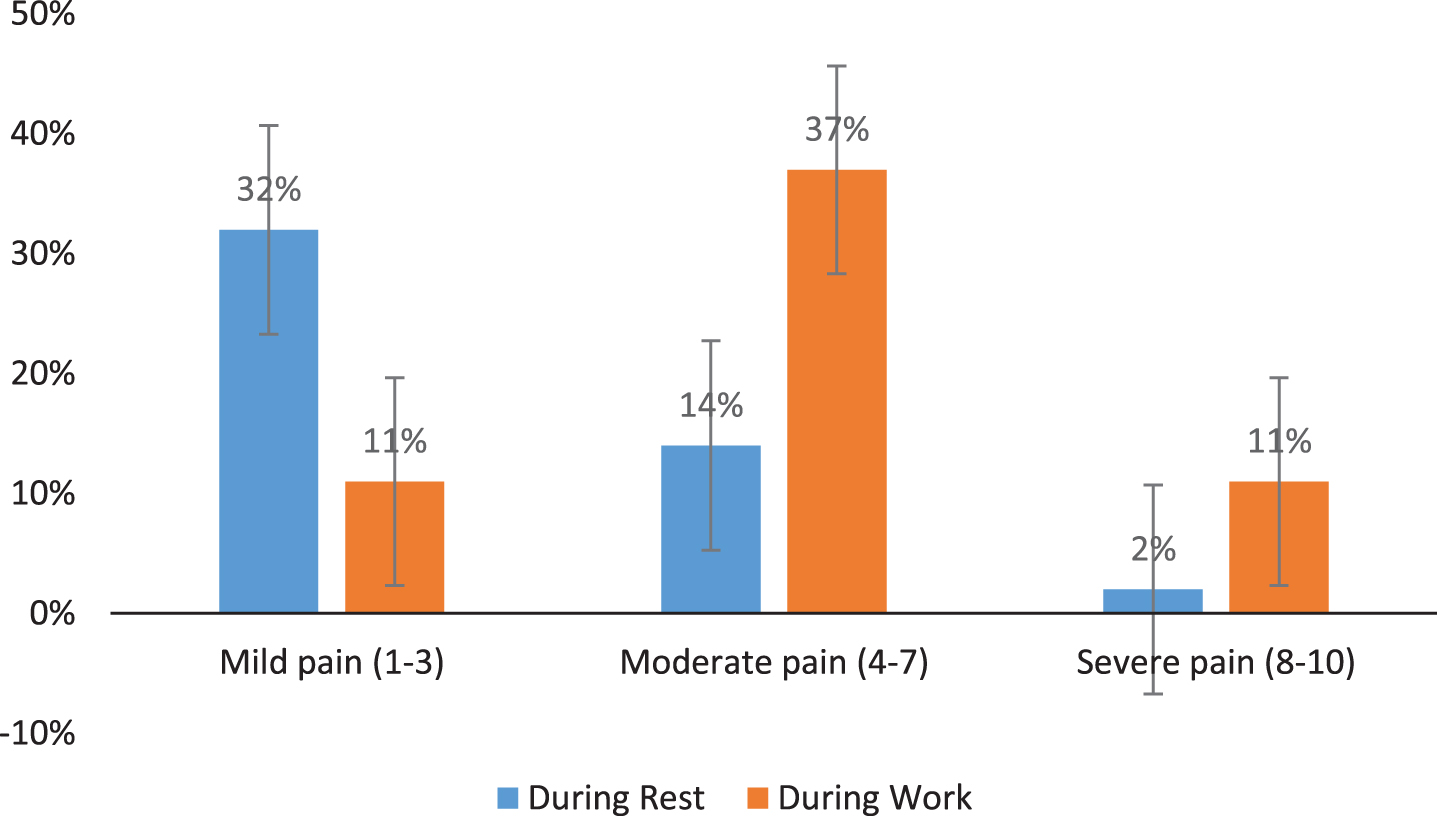
Pain intensity of construction workers during work and at rest.
Characteristics and consequences of musculoskeletal disorders among construction workers (n: 666)
There was a significant association between WMSDs and age (φ= 0.260, p < 0.001) which indicates that as age increased the chance of suffering from WMSDs increased. Similar associations were seen for work experience (φ= 0.220, p < 0.001), smoking habits (φ= 0.152, p = 0.002) and number of days off due to WRMDs (φ= 336, p < 0.001) (Table 4).
WMSD pain and association with risk factors in construction workers (n: 666)
The current study was conducted to determine the prevalence of MSDs, pain characteristics, and their associated risk factors among construction workers in Pakistan. Our study revealed that lower back pain (LBP) was the most prevalent type of pain among construction workers. Holmstrom et al. study supports our results, as they found that lower back symptoms were common among construction workers in the Swedish population [26]. Guo et al. concluded that there was a high proportion of workers experiencing lower back and waist symptoms [27]. Similarly, another study found that construction workers were most likely to have MSP involving the lower back, followed by neck, shoulder, and knee pain [28]. Rosecrance et al. revealed that 65% of experienced construction workers in Slovakia reported LBP [29]. Likewise, a study examining LBP in construction workers reported that 5,848 (29.3%) of 19,948 participants had reported LBP [30].
In our study, the highest incidence of WMSD in participants aged 36 to 45 years was 30.2%. Age was a risk factor for MSP in participants in this study, as reported in previous studies. However, some studies have shown that age is not a significant risk factor for MSPs [26]. In contrast to our study, Alghadir et al. reported that the highest incidence of WMSD was 38.7% among construction workers aged 30 and 39 years [31]. It is difficult to compare our results with those of other studies, probably due to differences in the population studied, data collection and analysis methods, and socio-economic status and safety rules, which varied from study to study. This study found that construction workers over the age of 45 reduced WRMSD compared to their younger counterparts. This could be because younger workers do more work compared to older workers.
In the present study, it was found that 29.4% (196) of participants reported being on sick leave for≤15 days per year due to WMSDs. Another study conducted in Hungary on construction workers showed that 42% of experienced workers reported absences due to LBP, along with 12% of trainee construction workers. These findings revealed that trainees experienced less MSP than experienced construction workers; there was a higher prevalence of WMSDs in experienced construction workers than in trainees due to their prolonged poor posture, vibrations, age, and physical and psychological stressors [32].
We also examined pain intensity and found that 37% of workers had moderate pain during activity, and 32% had slight pain during rest. A similar study by Alghadir et al. examined the average pain intensity during activity and at rest; they found that 56.3% of participants experienced severe pain, 41.3% experienced moderate pain, and 2.5% had mild pain during activity. At rest, only 1.3% had mild pain, 51.3% had moderate pain, and 47.5% had severe pain [31]. In addition, another study reported that the majority (73.4%) had moderate pain, and 5.4% reported severe pain at work that required a break for relief [30].
We investigated the duration of pain and revealed that a high prevalence of participants reported work-related MSP for≤2 hours, and the lowest number of workers reported pain > 1 week. Contrary results were found in another study conducted by Alghadir et al., who stated that there was a higher prevalence of workers who reported work-related MSP lasting for 2 to 4 days, with the lowest prevalence of those who reported pain for < 2 hours [31]. The presence of MSP during working hours affects work productivity. It has been reported that construction workers who miss work due to health problems (assuming a qualitative loss of productivity added to a quantitative loss of productivity) would lose an additional 0.5 hours a day [33]. There have been some studies examining an association between working hours, break time, use of protective equipment during work, and active and sedentary lifestyles with MSDs in construction workers. Previous studies [35–37] showed that the prevalence of MSDs increased among workers who worked longer hours. Alghadir et al. stated that workers who took longer breaks (more than 20 minutes) and used protective equipment during work reported fewer MSDs. [31]. While the association between break time and use of protective equipment with MSP has been reported in the limited literature, these two factors could be important risk factors for preventing MSDs in construction workers.
The findings of current study revealed physical activity is reducing the chances of MSDs among construction worker. Previous research reported that healthy lifestyles, including physical activity and fruit and vegetable consumption, were associated with a lower risk of MSDs [34]. Physical inactivity leads to MSP, and increased physical activity throughout life has been linked “to a decrease in pain from musculoskeletal disorders”[35].
The findings of this study showed that the smoking increased the chances of MSPs in construction workers who are currently smokers. An association between smoking and musculoskeletal disorder is still debatable. Some studies suggest that smoking is a predictive factor for the occurrence of the MSDs [26, 37], and other studies have shown that smoking is not a significant risk factor for MSPs [38, 39]. A study conducted in Japan showed that smoking was associated with relatively severe lower back pain rather than total pain [39]. Similarly, Meo et al. assessed work-related musculoskeletal symptoms among construction workers in Saudi Arabia and found that smokers had a slightly higher percentage of musculoskeletal symptoms [40].
Our results for evaluating the type of pain showed that construction workers had a high prevalence of dull pain, followed by cramping and shooting pain, with burning pain having the lowest prevalence. Another study similarly showed that construction workers had the highest prevalence of dull pain, followed by cramps and stinging, with burning pain having the lowest prevalence [41]. The type of the pain aspect can give us an indication of which structures are affected.
Our study showed that there was a large proportion of workers 309 (77.83%) who had received medical treatments and only 3.6% received Physical therapy treatment for their musculoskeletal symptoms. The literature has shown that construction workers are often stressed due to work-related injuries and pain; Therefore, most of the time they need medical help [42, 43]. A recent study found that 25% construction workers received physical therapy services due to MSP [31], which is quite high compared to our study which is only 3.6%.
Conclusion
We found that construction workers often experienced MSP. The largest proportion of workers experienced lower back pain, followed by knee pain, with ankle/foot pain having the lowest prevalence. In addition, dull pain was the main type of pain suffered by construction workers. Moreover, a significant association was found (p < 0.05) between MSDs and age, lifestyle, work experience, smoking habits, and absence from work.
Limitations
This study was limited to male participants and was conducted in construction sites located in Faisalabad city of Pakistan. Only three categories of construction workers, laborers, masons, and painters, were assessed in this study, so the results may not be generalizable to other categories of construction workers.
Conflict of interest
The authors declare no conflict of interest.
Funding
None to report.