
Abstract
BACKGROUND:
Musculoskeletal disorders (MSDs) are highly prevalent among dental professionals. Studies examining the prevention of dental work-related MSDs have been completed globally.
OBJECTIVE:
To identify and evaluate the available evidence regarding MSD prevention in dental practice, and to identify knowledge gaps.
METHODS:
An electronic search was conducted across multiple scientific databases. Identified articles were assessed according to inclusion/exclusion criteria. Systematic reviews, interventions and published expert opinion were included.
RESULTS:
Five systematic reviews, 27 intervention studies and 21 expert opinion articles were included. There was overall consensus that use of ergonomic equipment is beneficial in MSD prevention. Knowledge gaps identified included: a lack of systematic reviews on the role of exercise and therapy in MSD prevention; a lack of high-quality intervention studies; a lack of research in general outside of ergonomic equipment use. Expert opinion articles have been published despite a lack of dental-specific research.
CONCLUSIONS:
Whilst more robust research is required, current evidence supports the use of optical enhancement, saddle chairs, and wide-diameter silicone-handled instruments in MSD prevention. Knowledge gaps were identified relating to the use of exercise, therapy, and education in the prevention of dental work-related MSDs. Further research is required, specifically high-quality intervention studies.
Introduction
Clinical dental practice encompasses the work of oral health professionals in the treatment of patients. Oral health professionals include dentists, dental specialists, dental students, dental hygienists, and dental therapists. This work is often physically demanding, requiring both strength and endurance to undertake [1, 2].
High prevalence of dental work-related musculoskeletal disorders (MSDs) has been reported in the literature. Hayes et al. reported that 64–93% of dental professionals experience MSDs during their career [3]. A similar incidence level of MSDs has been reported in Australia [4, 5] and internationally in both developed and developing nations [6–8]. Risk factors that are associated with the development of dental work-related MSDs include awkward working posture, high number of treated patients, administrative work, vibration and repetition, physically demanding work tasks and repeated twisting and bending [1, 9].
Dental clinicians suffer both physically and mentally due to dental work-related MSDs. This includes acute and chronic pain, increased need to seek treatment, decreased productivity, increased absenteeism, increased use of analgesics, increased stress levels and decreased overall quality of life [7, 11]. At its worst, dental work-related MSDs may cause affected clinicians to leave the profession entirely. Brown et al. found that 90% of all ill-health related retirement among dentists was due to MSDs [12].
Due to the established prevalence of dental work-related MSDs, as well as its negative impact on clinician wellbeing, it is important to systematically review the current literature pertaining to the prevention of work-related MSDs. Methods of prevention include workplace related measures such as the use of ergonomically designed equipment, optimising surgery lay-out and improving work habits, for example taking breaks or appropriate appointment bookings. Prevention of work-related MSDs can also occur outside of the workplace. This includes seeking physical therapies, exercise, complementary and alternative medicine, and further education such as attending continuing education programs.
Aims
This scoping review was undertaken with the following aims:
Method
An electronic search was carried out on the OVID, EMBASE and CINAHL databases during December 2019 and February 2020 with a cut off publishing date of 27th Feb 2020. The search terms and the search strategy were determined with the help of a research librarian at the University of Melbourne (Table 1).
Search strategy
Search strategy
The search terms included in the search strategy were:
Dentist*, dental*, musculoskeletal disorder*, musculoskeletal disease*, MSD, ergonomic*, postur*, Pain*, spine*, spinal*
Two researchers participated in data collection and analysis (JW and MM) and independently identified articles that met the inclusion/exclusion criteria (Table 2), reaching a consensus if there was any disagreement. All included articles were further analysed for content and quality. Data regarding year of publication, study design, quality of publication, sample size, methodology, outcomes, and conclusions were extracted.
Inclusion and exclusion criteria
Systematic review quality was assessed using the Critical Appraisal Skills Programme (CASP) checklist [15]. The CASP systematic review tool was developed to help identify high-quality research and assess whether the content of the publication has relevance to practice. Therefore, the CASP checklist was selected as a valid and appropriate measure of quality for the included systematic reviews. The CASP assessment does not use a scoring system, rather it uses a two-step quality control checklist. The first two sections assess study design validity and methodological rigour. If a paper is deemed of high enough quality, it will then be assessed using the final two sections to give an overall impression of quality.
Interventional study quality was assessed using the Downs and Black assessment checklist [16]. This assessment tool has been validated for use in evaluating the quality of both randomised and non-randomised health care interventional studies by assigning a score of between 0–32. A score of 0–6 is considered low quality, 7–13 low-moderate quality, 14–20 moderate quality, 21–26 moderate- high quality and 26–32 high quality.
Published expert opinion was also included in the scoping review to represent the breadth of the accessible information on the topic of dental work-related MSDs. This included narrative reviews, opinion pieces and letters to the editor. It is not possible to determine the quality of expert opinion, however, it is important to include this subsection to highlight the advice that is being disseminated regarding dental work-related musculoskeletal disorders and determine whether it is reflective of the available evidence.
Initial searches across the listed databases identified a total of 1313 articles. After duplicate removal and application of inclusion/exclusion criteria, 43 articles remained. Following hand searching of reference lists, a further 10 articles were identified for inclusion, leading to a final total of 53 included papers (Fig. 1). Five were systematic reviews, 27 were interventions (including case studies) and 21 were expert opinion articles (See Tables 3–5 for a summary of results).
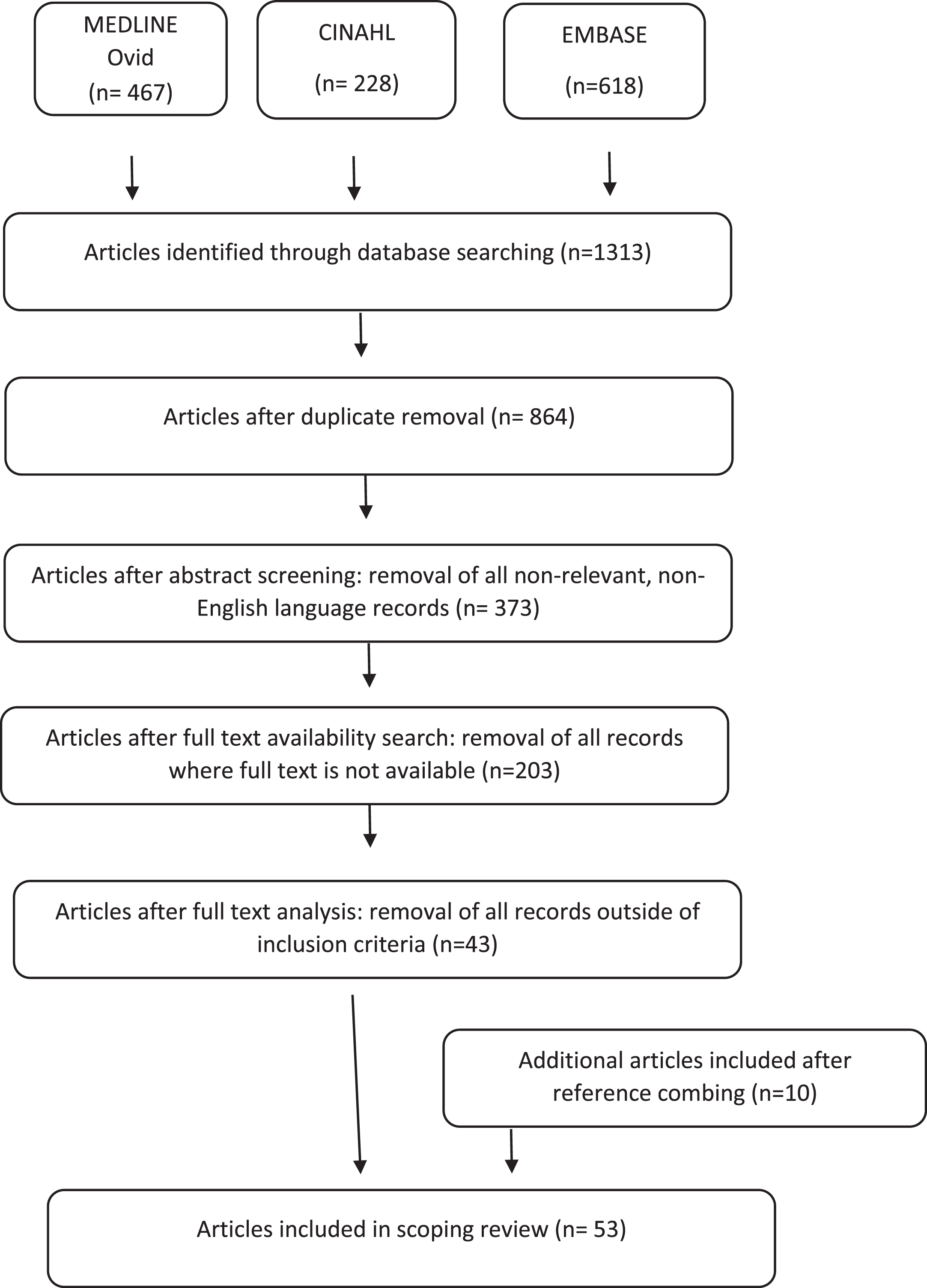
Flowchart for searching and selecting the literature.
Systematic reviews results summary
Intervention studies and case studies results summary
Expert opinion results summary
Applying CASP assessment, the study by Roll et al. [17] was found to be the only systematic review included that was of high quality with a clear aim, methodology and applicable results. The study by Plessas and Delgardo [18] was considered to be of moderate to high quality, however the other three systematic reviews [3, 20] were all low to moderate quality due to poor guiding questions or not being applicable to a clinically practicing dental professional.
Among the 27 intervention studies identified, 18 assessed the effect of ergonomic equipment across three broad categories: seating design, visual magnification design and instrument handle design. Six studies looked at the effect of exercise or physical therapy on MSD and three studies explored the effect of ergonomic training on MSDs. Of these 27 studies, sample sizes were generally small. Only four studies had a sample size of over 100. Ten studies had sample sizes between 31–100 and nine studies had between 11–30 participants. Four case studies with one or two participants were also included.
Application of the Downs and Black assessment demonstrated that an overwhelming majority of the intervention studies were of very low, low, or moderate quality. Of the 27 studies, only two could be considered high or moderately high quality. Lindegard et al. conducted the largest intervention study, with over 500 participants, concluding that prismatic glasses significantly improved participants’ pain and work ability with an overall high compliance rate [21]. Nemes et al. conducted a prospective, randomised controlled study comparing modalities for MSD management. They concluded that dentists who used medications and rehabilitation compared with those using medications alone achieved significantly better outcomes in all categories measured [22]. The remaining studies were deemed of low to moderate quality mostly due to small or very small sample sizes, lack of blinding, non-randomisation or being conducted in a non-clinical setting.
Published expert opinion was well represented in our search, with 21 articles identified for inclusion. Of these, there were six narrative reviews, thirteen opinion pieces and two letters to the editor. Articles in this category tended to be quite broad in nature, covering both aetiology of MSDs as well as proposals of recommendations on preventative measures. Many articles included definitive recommendations using pictures or photos of recommended preventative exercises, however these were not supported by evidence.
There was consensus amongst the studies for several of the prevention strategies. However, overall, the quality of evidence is low. This serves to highlight the need for further, more robust, research in this area.
Regarding research on ergonomic equipment, systematic reviews identified examined the impact of ergonomically designed equipment on MSD experience. Two papers focused solely on the effect of ergonomically designed equipment on MSD prevention, such as stool design or the use of loupes in dental practice [18, 19]. The systematic review by Plessas and Delgardo included four studies on the use of loupes in dental practice and concluded that using loupes decreased clinician discomfort [18]. This was a moderate to high quality review as per CASP assessment.
All interventional studies on this topic, except two, concluded that there was an overall benefit to the clinician in using optical enhancements. Lindegard et al. produced the only high-quality study on this subject and found that the use of prismatic glasses produced a significant reduction in neck flexion [21]. Hayes et al. produced the two studies that concluded that loupes use among dental hygienists did not significantly improve neck pain or scapular positioning [23, 24] however, these studies were deemed to be of low to moderate quality due to several issues such as non-equivalent group selection and lack of randomisation and blinding.
Chair design was examined in two systematic reviews. Gouvea et al. [19] and Plessas and Delgardo [18] both included dental chairs in their systematic reviews. Gouvea et al. found that saddle seats presented a significantly lower ergonomic risk compared to conventional seating. Plessas and Delgardo found that the use of saddle chairs improved operator posture and that using both saddle chairs and loupes had a cumulative benefit. Dental chairs were tested in only four studies included in this scoping review. Two were deemed moderate quality [25, 26] and two were low or low-moderate in quality [27, 28]. There was consensus among all four studies that saddle chair use improved operator posture as compared to a conventional dental chair.
Instrument handle design was examined in one systematic review and four intervention studies. Mulimani et al. conducted a systematic review that concluded the use of lighter and wider diameter instruments had no clear effect on elbow and shoulder pain [20]. This systematic review was of low to moderate quality and the use of lighter instruments was a small component of the conclusions drawn. By comparison, the four intervention studies all strongly recommended the use of light and wider diameter instruments, as they showed a significant benefit to MSD prevention [29–31]. These interventions ranged from low to moderate quality.
Regarding research into exercise and therapies to assist with MSD prevention, only one systematic review and six interventional studies were identified on this topic. The systematic review mentioned that lack of exercise exacerbates symptoms [17], however this was not a focus of the review. Of these intervention studies, one was deemed high quality, two moderate quality and the remainder low or very low quality. There were thirteen expert opinion articles identified that recommended some form of exercise or therapy to minimise MSD development.
Continuing education was mentioned briefly within two of the systematic reviews and was the subject of only three studies. Of the systematic reviews, Hayes et al. showed that whilst 97% of dental hygiene training programs taught basic operator positioning, only 32% provided additional teaching on topics such as ergonomics and preventative exercise [3]. Roll et al. concluded that ergonomic training appears to decrease MSD experience [17]. Of the 26 intervention studies, only three, one of which was a case study, incorporated ergonomics education and assessment into their methodology. None of these papers can be categorised as being of high quality.
Content analysis revealed the following gaps in the literature: There have been no comprehensive systematic reviews on the role of exercise and therapy on MSD prevention. There is an overall lack of high-quality intervention studies across this topic. There is an overall lack of research regarding intra-operative prevention methods outside of ergonomic equipment use. There is an overall lack of research regarding the effect of exercise and therapy on MSD prevention in dental practice. There is an overall lack of research regarding the effect of ergonomic training and education on MSD prevention in dental practice. Expert opinion articles are being published despite a lack of dental-specific research.
This review has demonstrated that the body of knowledge around MSD prevention for dental clinicians is limited and mostly of poor quality.
The intervention studies identified in this review were few and tended to be of very low to moderate quality. Previous systematic reviews which often had low or very low numbers of included papers that met inclusion and exclusion criteria. Some of the common reasons for the low quality include: Lack of blinding: Many of the intervention studies required the provision of equipment which meant the participants could not be blinded. There was also often a lack of assessor blinding as well. Both these factors contribute to an increased risk of bias in the reported results. Lack of randomisation: Many of the interventions identified allowed for self-selection into the intervention/ non-intervention group. One example of this is the study by Lindegard et al. [21] which was the largest investigation identified, with over 500 participants. Lack of randomisation increases the risk of bias. Small sample size: Only four intervention studies had more than 100 participants. Small sample sizes decrease statistical power and increase the risk of type II (false negative) errors. Convenience sampling of student participants: More than half of the studies utilised student clinicians as all or part of their cohort. Whilst younger clinicians have been found to have higher rates of MSD experience [32, 33], student clinicians do not have the same clinical workload that a qualified dental professional would experience. Students are also likely to spend more time performing out-of-clinic tasks such as studying at a desk that might impact their MSD experience.
Another issue is the relevance of studies in the pre-clinical setting with mannequin teaching models. Whilst this is a reasonable approximation of clinical dentistry, it does not allow patient-related factors such as unexpected movement to be accounted for, therefore conclusions drawn may not be generalisable to clinical practice on patients. It also does not allow for the added element of stress that can arise when treating patients who themselves may physically react to treatments provided. Student training within a pre-clinical setting remains a valid educational strategy, however it may be preferable to measure outcomes after they are qualified clinicians to determine if the results are clinically relevant.
The most adequately researched area of dental work-related MSD prevention is that of ergonomic equipment use including visual enhancement, seating options and ergonomically designed tools. There was general consensus that the use of optical enhancement such as loupes or prismatic glasses improves operator body positioning [23, 24] Currently, this consensus is reflected in the recommendation of vision enhancement in the published expert opinions [34, 35]. This finding differs in fields outside of dentistry. Research regarding loupes and headlight use among medical surgeons determined that the added weight of these devices increases the degree of cervical flexion and could be contributing to postural issues [36, 37]. One explanation as to why loupes use is more beneficial in dentistry could be due to the seated nature of modern dentistry as compared to medical surgeries which are completed with the clinician in a standing position. Further investigation should focus on providing higher quality data and on specifying the most advantageous type of visual enhancement such as differentiating between loupes, prismatic glasses, operating microscopes etc.
There was also a consensus in favour of the use of saddle-style chairs. The use of saddle-style chairs in comparison to conventional dental stools improved operator posture [18] and lowered ergonomic risk [19]. This finding is supported by evidence outside of dentistry. Gadge et al. showed that the Bambach saddle chair “consistently promoted a greater trunk to thigh angle for all subjects, a position associated with optimum sitting posture” [38]. Similarly, saddle chair use has also been shown to decrease musculoskeletal discomfort amongst microsurgery surgeons [39]. Parallels can be drawn between dentistry and microsurgery work tasks as both require high levels of concentration and precision within small fields of vision. Interestingly, one expert opinion paper recommended anterior support rather than back support to decrease sustained muscle activity which is a leading cause of MSDs [40]. This is a concept that should be explored in future research as it is a novel approach to postural support. Until further evidence is synthesised, it is appropriate to continue recommending saddle-style chairs for use by dental clinicians.
Another ergonomic improvement was the use of light, wide diameter silicone instruments in place of heavy, narrow diameter metal handled instruments for hand and wrist MSD prevention. Whilst the available interventional studies are of low to moderate quality, there is consensus that the use of lighter, wider diameter instruments decreases the development of hand and wrist pathologies [29, 31]. Interestingly, wider diameter pens have also been found to decrease wrist discomfort when writing [41]. This is an analogous action to providing dental treatment as dental handpieces are usually held with a pen grip.
Whilst ergonomic equipment use is an essential component of MSD prevention, there is a lack of research into other forms of MSD prevention that can be undertaken in the workplace, such as the effect of taking breaks during the workday, appointment booking strategies, etc. An example of this outside of dentistry has been the benefit of micro-breaks during surgery to allow surgeons to follow a stretching regime [42]. Perhaps actions can also be taken by dental practitioners outside of the work environment to decrease risk of MSD development. A randomised control trial showed that surgeons who completed a prevention program incorporating ergonomic education and targeted physical activity showed significant improvement in general health, lower back pain and analgesic consumption[43]. Similar research regarding the effect of exercise and physical therapies to assist with dental work-related MSD prevention is scarce and could be conducted to improve knowledge in this area.
Nemes et al. conducted the highest quality interventional regarding the effect of physical therapy in dental work-related MSD prevention. Study numbers were large and there was a lengthy follow up period, unlike most of the other interventions identified. This study demonstrated that a combination of medication and physical therapy intervention produced the best overall outcome as compared to medications alone. Whilst the recommendation was for “relaxation, stretching and general strengthening”, Nemes et al. also suggested that ‘this programme should be individualised for each musculoskeletal disorder” [22]. One issue with this study was the multi-modal nature of the intervention involved. More research is required to determine which component is the most relevant, or whether a combination is more effective.
The effects of therapeutic exercise were examined in two moderate quality intervention studies. Letafatkar et al. demonstrated that therapeutic exercises targeting muscle co-ordination and proprioception, muscular endurance and muscle strength significantly decreased pain experience and improved cervical and shoulder angles [44]. Gupta et al. showed that head forward positioning significantly improved with deep cervical flexion training [45]. These studies show a trend regarding the benefits of using targeted therapeutic exercise. This trend is also supported in a broader sense, a randomised control trial conducted on surgeons demonstrated that following a targeted exercise regime decreased MSD experience [43]. There is a need to further investigate the effect of therapeutic exercise for dental work-related MSDs before recommendations can be made with confidence.
Other therapies examined included the use of high frequency transcutaneous electrical nerve stimulation which significantly decreased pain and fatigue in the short term for several hours after application. This positive effect did not produce long lasting results as benefits did not persist the day after [46]. The practice of yoga was also shown to be beneficial with bi-weekly yoga classes decreasing pain experience among dental hygiene students [47]. This highlights the breadth of possible preventative modalities which could be explored in the future.
It is interesting to note that regarding exercise and therapies, there were almost as many expert opinion publications identified as there were scientific intervention studies. This scoping review has highlighted the need and desire for further knowledge on MSD prevention in the workplace among dental professionals [40]. However, there is a lack of reliable evidence to help guide their actions. Despite the lack of scientific evidence, expert opinion articles frequently included exercise regimes that were advertised as preventative against MSD development [48–50]. These exercises routines either had no evidence cited or have been modified from generalised MSD research. The effectiveness of these exercise routines have not been evaluated for dental health professionals specifically. This serves to highlight that recommendations are being made in this space that are not justified or validated and reiterates the need for more robust research to examine the potential preventative nature of targeted exercise regimes.
One final area of interest is the effect of education in the prevention of MSDs. This was the least explored topic. Whilst there were brief mentions of education within two of the systematic reviews only three intervention studies covered this topic, one of which was a case study. Bedi et al. demonstrated that less than a third of subjects applied ergonomics to their practice after further education [51]. No specific reasons were given for the low rate of implementation however possible reasons could include lack of workplace support, lack of necessary resources or lack of personal motivation. In another study, Partido and Wright used photographs of dental students and asked them to self-assess their posture during the intervention period. They found that the intervention group using photos improved their ergonomic scores and postural awareness whilst the control group without photos did not [52]. This suggests that personalised teaching tools may have a greater impact on outcome. However, both papers were of low to moderate quality and definitive conclusions cannot be drawn. There is a particularly large gap in research into MSD prevention education and this warrants further investigation.
Limitations
This scoping review, whilst conducted in a comprehensive and systematic manner, still has some limitations. First, due to the nature of scoping reviews involving synthesis of broad and descriptive data as compared to a systematic meta-analysis, the search terms used are less defined and therefore less targeted. This means that while broad generalisations and large gaps in the literature were identified, specific recommendations could not be made and therefore further research would be required. For example, while a consensus was reached that use of optical enhancement is beneficial, a specific recommendation on which type of glasses, loupes or microscopes are best practice cannot yet be made.
There is also a possibility of bias when conducting scoping reviews as with any form of information synthesis. Bias was limited in this study as much as possible by having two independent researchers review the papers identified and through the use of validated instruments such as a CASP assessment tool and the Downs and Black assessment tool. These methodologies aim to limit bias, however, some inherent bias may still be present.
Conclusion
The prevention of MSDs among dental professionals would be of a great benefit to dental clinicians. The current consensus regarding the prevention of dental work-related MSDs includes the use of optical enhancement, a saddle chair and light, and use of wide diameter silicone handled instruments, however more robust research is required.
There is a large gap identified in the available research relating to the use of exercise, physical therapy, and education in the prevention of dental work-related MSDs. Further research is required, specifically the production of high-quality intervention studies.
Footnotes
Acknowledgments
The authors thank Mr Wilfred Villareal, librarian, Brownless Biomedical Library, The University of Melbourne, for assistance with search terms and search strategy.
Author contributions
Dr. Jean Wu, Prof. Michael McCullough and Prof. Mary Galea contributed to the concept and methodology of the review. The literature search, data collection and analysis were performed by Dr. Jean Wu and Prof. Michael McCullough. The first draft of the manuscript was written by Dr. Jean Wu. Prof. Mary Galea, Prof Michael McCullough and Dr. Maya Panisset critically revised the work.
Conflict of interest
None to report.
Ethics approval
Not applicable.