
Abstract
BACKGROUND:
In nursing practice, cognitive failures can be evaluated as an essential indicator of the cognitive capacity of individuals.
OBJECTIVES:
This study aimed to determine the validity and reliability of the Persian version of the Workplace Cognitive Failures Scale (P-WCFS) among Iranian nurses and its relationship with personality traits.
METHODS:
Data collection had two phases: 1) The P-WCFS prepared through a standard translation process. Then the content validity was evaluated by a panel of specialists. Reliability Cronbach’s coefficient alpha obtained 0.91 from a pilot study. 2) For measuring neuroticism and conscientiousness used the Goldberg Personality Questionnaire. Exploratory and confirmatory factors analyzed in two separate parts of the sample (n = 351). SPSS (v 18) and STATA 14 performed for Statistical analysis. Spearman correlation and Pearson correlation coefficient used to measuring the convergence and examine the relationship between the subscales of the questionnaire.
RESULTS:
Cronbach’s alpha was 0.92, which showed a high level of reliability for this questionnaire. The three-factor model of WCFS was well-fitted. The reliability of all three sub-scales was a reasonable level. Cognitive failures and its subscales had negative and strong relationships with conscientiousness and neuroticism. The highest internal consistency was related to memory subscale, and all scales had a success rate of 100%.
CONCLUSIONS:
This study showed the P-WCFS has high reliability and validity and can be used in nursing society.
Introduction
Cognitive failure is the individual inability to complete and perform a task that he can typically perform [1]. Some common examples of cognitive failures are throwing away what we intended to keep in grip, not remembering a familiar name, or taking a medicine that we did not aim to consume instead of another medicine [2].
According to the studies, there is a positive relationship between unsafe behavior and occupational accidents in the workplace, and a higher score of cognitive failure [3]. Also, a significant relationship between the experience of accident and high-level cognitive failures [4]. Cognitive failures can act as a mediator between work interruptions and near-misses [5]. Those with more cognitive failures are less likely to pay attention to the external environment, which can lead to cognitive failure and errors [6]. The study by Wallace and Chen showed a strong relationship between cognitive work deficits in the workplace and outcomes such as unsafe behavior, occupational accidents, and other job variables [7]. However, measurement of daily slip and lapses error can predict unsafe behaviors in the workplace [8, 9]. Therefore, cognitive failures are attractive because of the desire to measure individuals’ cognitive and mental capacities through the evaluation of cognitive failures, especially in ergonomics and human errors field [2].
Cognitive failures in the workplaces not only related to the requirements and working conditions but also associated with personality traits [7]. A lot of researches consider cognitive failure as a personality trait [3], with relatively high stability [2]. People with high conscientiousness, who desire to do a task well, disciplined, and organized, have reported fewer cognitive failures [10].
Although, the proven relationship between cognitive failure and accident-prone and occurrence of accidents, the nature of these failures in the workplace has been less studied with a special job-based cognitive tool [3]. Several studies among nurses have identified cognitive failures as a valuable and essential factor concerning job characteristics [11], daily working conditions [12], adverse events [13], workflow interruptions [5], and job stress [14, 15]. Nurses, as the major part of the healthcare workforce, play a more active role in patient care and play an essential role in improving patient safety [16]. Considering the importance of cognitive failure in nursing society and its relationship with personality dimensions, safety behaviors, and medical errors in therapeutic settings, it seems necessary to use a tool that can assess cognitive failure in the work environment. Therefore, this study aims is to provide a valid and reliable Persian tool to measure cognitive failures among nurses.
Methods
Participants
Considering both factors analyzing (EFA and CFA), the sample size of 300(81.52% of the study population) met the criteria that sample size must be at least ten times the number of variables involved in the questionnaire for an adequate execution of the factorial analysis model [17]. In this study, nurses who worked in public hospitals in Shiraz (six hospitals) were surveyed. In total, 635 questionnaires were distributed among nurses, and 388 completed questionnaires returned (response rate was 61%), 20 questionnaires excluded due to work experience under a year, and defects in the completion and the completion without reading. The data collection phase lasted from February to June 2016. For performing sampling at different shifts (at least three shifts per hospital), all departments of each hospital were referred. The consent letter was obtained from the participants after a brief face-to-face explanation about the purpose of the study and made assure about the confidentiality of the information.
Instruments
WCFS: Wallace and Chen presented the “Workplace Cognitive Failure Scale” (WCFS) to evaluate cognitive failures in the workplace. In a healthy population, it can measure the cognitive resources of individuals, including attention regulation, memory function, and action exertion. This questionnaire has 15 items, each item score on a 1–5 Likert scale (respectively, never, very rarely, occasionally, often, and always). Scale dimensions of WCFS are calculated based on the mean and standard deviation. Higher scores in the WCFS represent more errors; the tool structure is similar to the general cognitive failure questionnaire [7].
Goldberg’s Big Five 50 personality markers: Along with other studies [4, 18], Personality traits assessed in this study, we used the “Goldberg’s Big Five 50 personality markers” (GPO) that it has 50 items and suitable psychometric properties [19]. For assessing each personality area, ten items were considered, and each question scored from one to five, and each personality scale has a score of between 10 and 50. Like the other studies, we considered the relationship between neuroticism and conscientiousness with cognitive failure [3, 18]. In Goldberg’s research, Cronbach’s alpha coefficient for conscientiousness was 0.79, and for neuroticism was 0.86 [19]. In a study conducted by Khormaie in Iran [20], Cronbach’s alpha of the Persian version was 0.88 for neuroticism and 0.80 for conscientiousness. In Goldberg’s research, Cronbach’s alpha coefficient for conscientiousness was 0.79, and for neuroticism was 0.86 [19].
Data collection procedure
The study was developed in two phases. In the first phase, the linguistic, and content validity of P- WCFS was checked after obtaining permission from the author of the reference document of the WCFS questionnaire through email. In the second phase, the required data was collected from the sample of nurses in governmental hospitals in Shiraz. For linguistic validity, first, the English version of the WCFS was translated into Persian by two fluent English-language translators independently. After the forward translation, both translators and an ergonomist resolved any discrepancies and integrated translations into the only version. The only version was retranslated from Persian into English by two different translators working independently to confirm its accuracy to the original questionnaire. Lastly, a fluent English speaker checked the final questionnaire version and verified it [21, 22]. Ten experts asked to comment on the content validity of each question and the ability to transmit the message to the nurses, and the necessary changes made based on their opinions. For confirmation of content validity, the content validity index (CVI) and the content validity ratio (CVR) were calculated [23]. The value of CVR was obtained at 0.83. No questions were deleted at this time. For determining the CVI, three criteria: simplicity, specificity, and clarity were separately examined and evaluated on a 4-part Likert scale for each one, and its value was calculated to be 0.68. After completing the above steps in a pilot study to a preliminary review of internal consistency, 22 nurses in one hospital completed the P-WCFS. Cronbach’s alpha evaluated internal consistency, and it was 0.91, and the questionnaire has good reliability. Finally, this stage led to the preparation of the P-WCFS questionnaire. In the second phase, the questionnaire distributed to the study population, and factor analysis was performed based on the collected data.
Statistical analyses
Statistical analyses were performed using SPSS v. 25 (IBM Corp., Armonk, NY, USA) and STATA MP 14 (Stata Corp., College Station, TX, USA) software. Internal consistency was calculated by Cronbach’s alpha (the recommended limit was α ≥7.7) [24, 25], and structural validity was evaluated through factor analysis. Considering the appropriate sample size, “Exploratory Factor Analysis” (EFA) was carried out in 184 participants. Then according to the preliminary results, a “Confirmatory Factor Analysis” (CFA) was per-formed on the remaining 184 participants. Spearman’s correlation coefficient was used to measure convergence, and the Pearson correlation coefficient was used to examine the relationship between the subscales of the questionnaire.
Results
In this study, the mean age of participants was 29.5, and 71.30% were aged less than 30 years old, and 316 (85.9%) of participants were female, and 52(14.1%) of participants were male, and 178 (48.36%) of them were married. Job experience in 64% of people was less than five years, 17.1% were 5–10 years, and 19% were above ten years. In this study, 28.5% of the nurses were working in ICU, 23.8% in the emergency departments, 15.1% in the surgery departments, and 32.3% in other departments of the hospitals.
The results of the WCFS score showed that the lowest score was in the action sub-scale (1.94±0.75), and also scores of attention (2.12±0.88) and memory (2.10±0.82) were high (Table 1).
Internal reliability coefficient of P-WCFS and personality traits
Internal reliability coefficient of P-WCFS and personality traits
The Factor analysis was performed in two exploratory and confirmatory phases to determine the construct validity of the P-WCFS. First, for 184 participants, EFA was done by using the principal axis factoring and direct oblimin rotation method. The Kaiser-Meyer-Olkin (KMO) test for sampling adequacy was calculated to ensure that the sample size was sufficient and its value was 0.92. Then, to determine that the correlation between the variables is not equal, the Bartlett test of sphericity was used, whose value calculated to be 1456.09 (df = 105, p < 0.0001), which is significant and shows that the correlation of the data in the population is not zero. According to the results of EFA, similar to the original version of the WCFS, three factors structure suggested for new WCFS which is accounting for 56% of total variances.
The factor loading results presented in Table 3. The factor-item loading values over 0.4 consider as satisfactory for the allocation of that item to the factor. The factor loading of the effects of items were expected, except question 11, which was placed on the attention subscale. Considering the theoretical basis and factor load of this item (0.497), the research team put question 11 in the subscale of the action [7] (Table 2).
Exploratory factor loading for three scales of P-WCFS
Internal sustainability P-WCFS and sub-scales based on gender, marital status, work experience, and job sections
To assess how well three factors model fit to observed data, a CFA was carried out by Structural Equation Modeling (SEM) by using the STSTA software. The results of CFA in the remaining 184 nurses confirmed the results of EFA. There are several fit indices to evaluate factor analysis models. The χ2 ratio to the degree of freedom (χ2/df), Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean square Residual (SRMR), Comparative Fit Index (CFI), and Tucker-Lewis Index (TLI) used in this study. The fit indices of the new WCFS were as follows: the χ2 of the three-factor model with df = 86 was 147.547, and the χ2/df was 1.71 also other fit indices were; RMSEA = 0.062, CFI = 959/0, TLI = 950 = 0 and SRMR = 0.042, that showed acceptable fit for three factors model. Figure 1 also shows the standard values for the WCFS, which resulted in the CFA step.
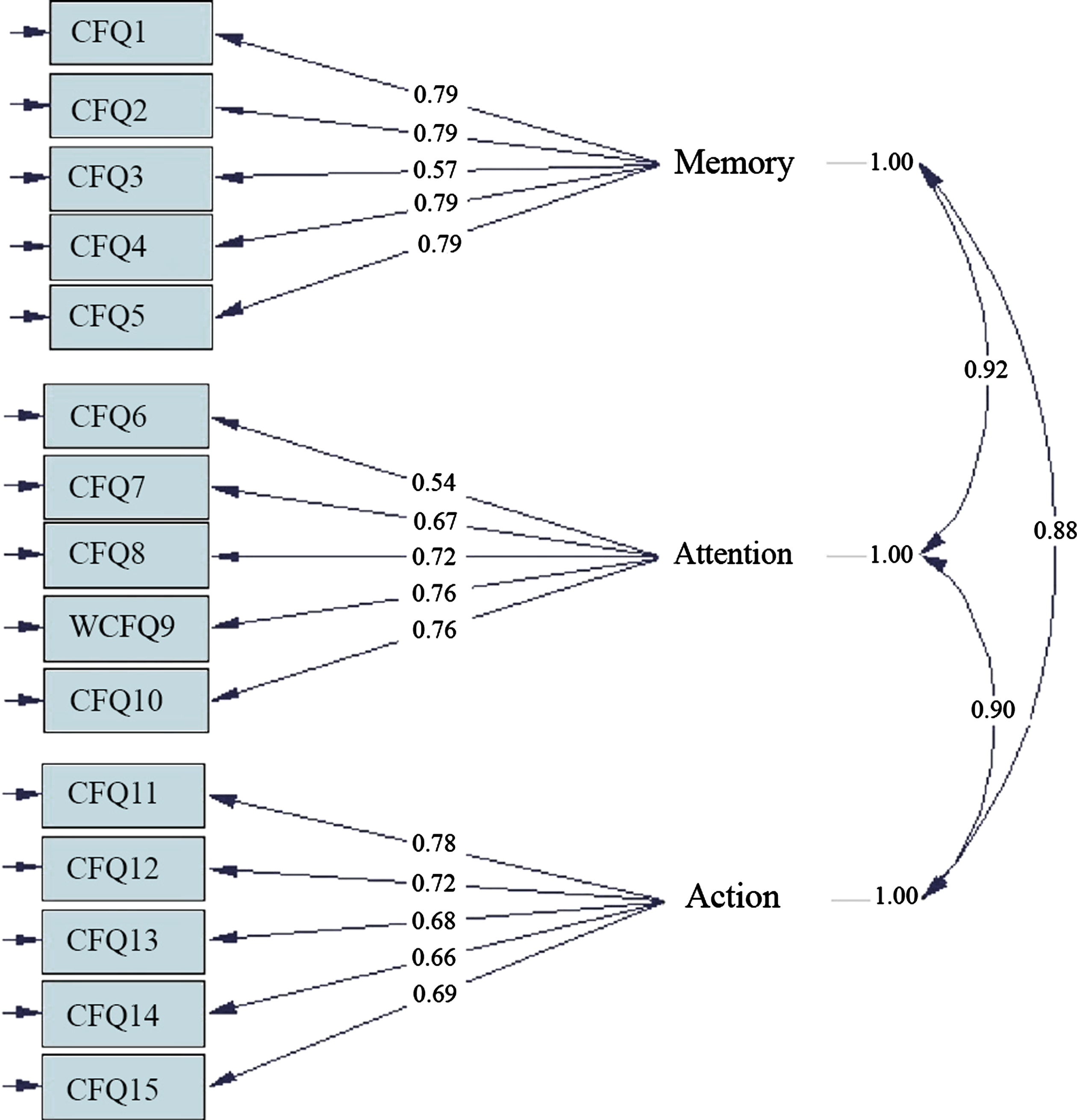
Path diagram revealing the standardized parameters relating items to relevant factors. All parameters were statistically significant, and all three factors were correlated significantly (P-value < 0.05).
For representing the reliability of P-WCFS used the Cronbach’s alpha coefficient and for the overall reliability, the Cronbach’s alpha value was 0.92. The alpha values of the three subscales of WCFS were 0.85, 0.81, and 0.84. Also, the reliability and internal consistency based on gender, marital status, work experience, and departments showed that sustainability was acceptable in all cases; the results of the reliability analysis set out in Table 3.
The Spearman correlation was used for calculating the convergent validity of items and subscales, as well as between sub-scales with each other. The highest internal consistency related to the sub-scales of memory, and all scales had a 100% success rate; Table 1 presents the convergent validity results. Calculating the correlation of WCFS with personality used the Pearson correlation coefficient test (Table 4); both dimensions of neuroticism and conscientiousness had a reverse relationship with cognitive failures and its subscales.
Determining the relationship between personality dimensions and cognitive failures
This study set out with the aim of validating the P-WCFS among the Iranian nurses. Persian version of the WCFS consists of 15 items. The WCF assessment is mainly through questionnaires that these tools show people’s opinions about their cognitive function [3]. This study was performed based on a similar process in Germany, Korea, and other countries [11, 26]. Linguistic validity, cultural adaptation, and content validity assessed in the standard forward-backward translation process and expert judgment method that results were acceptable. The reliability of this tool was measured using Cronbach’s alpha method. Construct validity checked through factor analysis in two exploratory and confirmatory phases.
The overall reliability of the new WCFS version was excellent (α > 0.9), the reliability of all three sub-scales of memory, attention, and practice was good [24]. Following the present results, previous studies showed similar results to ours; the Korean version of WCFS Cronbach’s alpha was about 0.9 [13]. In the Korean version, all three sub-scale of memory, attention, and action were good (0.8 < α< 0.9), also in the WCFS German version, all three sub-scales were within the range of (0.7 < α< 0.8) [11]. Compared to the reliability coefficient of the German and Korean versions, the P-WCFS has the best internal consistency [13, 24].
According to the results of EFA, similar to the original version, three factors structure suggested together explained 56% of total variances, and the results of CFA confirmed these results. Based on recommended values, fit indices and acceptable indices were: χ2/df < 5 and smaller value shows better fit, RMSEA < 0.08, CFI and TLI > 0.95 and SRMR < 0.05 [27–30]. Compare to acceptable values in the P-WCFS three-factorial model, three of five indices (χ2/df, RMSEA, SRMR) were very good, and the other two indices (CFI, TLI) were good, so overall, this model showed very good fitness and convergence. We can say the present model has a very good fit, and the results of the EFA phase are confirmed. Compared to the English version of the questionnaire (χ2/df = 1.85, RMSEA = 0.09, SRMR = 0.04, CFI = 0.91) [7], it can be deduced that the P-WCFS is desirable and even more suitable in some indices. Like the German version, this study has analogous fit indices, and this study aligned with other studies led in the three-factor structure model.
A significant association with two personality traits of conscientiousness and neuroticism demonstrated convergent validity for the P-WCFS. Several studies highlight the strong correlation between conscientiousness and neuroticism. Conscientious people are expected to experience fewer cognitive failures, and in contrast, individuals who score high on neuroticism are more likely to make cognitive failures [3, 11]. In this study, scoring of the neuroticism scale is such that higher scores represent more emotional stability and calmer. In fact, a significant correlation that participants who reported lower conscientiousness and more neurotic report higher scores of WCFS, confirming the scale’s convergent validity.
The study sample consisted only of Iranian nurses, which may need some justification for the applicability of P-WCFS in other worker populations. Considerably Further research might explore the applicability of P-WCFS on broader and more diverse people to alleviate these limitations.
Conclusion
In the present study, the translation process, cultural adaptation, reliability, and construct validity analysis of P-WCFS were made for Iranian nurses. Therefore, the present study showed that the P-WCFS had a good reputation and was well used in nursing society. Our findings showed the P-WCFS has a good structure and validity as well as the validity of the items within the item were good. It has a well-organized sub-scale for measuring workplace cognitive failures among Iranian nurses. Also, according to the factor analysis, we recommend the results of P-WCFS analysis based on the three suggested sub-scales (memory, attention, action). Although this questionnaire was used in the medical and nursing care environment, the P-WCFS questionnaire can be used in studies of cognitive sciences, ergonomics, and human error in various occupations.
Footnotes
Acknowledgment
The present study was sponsored by Shiraz University of Medical Sciences in the form of a master’s degree dissertation project no. 9919-04-01-94. The authors of the paper express their appreciation to Mr. Mohsen Varzandeh for managing the translation process, as well as all heads of departments of hospitals, head nurses, and nursing staff who participated in the study.
Conflict of interest
None to report.