
Abstract
BACKGROUND:
Healthcare workers typically perform their work under adverse conditions, increasing their susceptibility to developing burnout syndrome (BO). The paucity of research on the relationship between organizational identification (OI) and perceptions of organizational justice has created the need to address this topic more deeply.
OBJECTIVE:
This study aimed to assess the relationship between OI and BO, identifying whether perceptions of organizational justice act as mediating variables.
METHODS:
In total, 402 healthcare workers (physicians, professionals, and nursing assistants) completed Colquitt’s (2001) Organizational Justice Scale, Mael and Ashforth’s (1992) Organizational Identification Scale, and Maslach’s (1986) Burnout Inventory. Two competing structural equation models were evaluated.
RESULTS:
Our partial mediation model showed that the direct relationship between OI and BO was not significant (β= –0.16; p = 0.07). Therefore, a total mediation model was selected, showing that the indirect effects of OI on BO through perceptions of distributive justice (β= –0.16; p = 0.00) and interpersonal justice (β= –0.11; p = 0.02) were significant.
CONCLUSION:
Adjusting the processes of health institutions considering a vision of organizational justice and increasing the worker’s sense of belonging to his or her organization and his or her work team would, in turn, result in a lower probability of experiencing burnout syndrome.
Introduction
A series of economic, regulatory, technological, and social changes in the Western world have originated new ways of hiring, work organization, and relationships with organizations [1]. However, some consequences of these changes are evaluated negatively, becoming dysfunctional for the individual. For example, from the well-being point of view, these changes generate stress, uncertainty, and job insecurity, while, from the organizational point of view, they generate a more significant burden, less control of work, and fewer learningopportunities [2].
One of the occupational groups that have felt the most considerable impact of these changes is healthcare workers, who have been addressed on numerous occasions in the scientific literature as a labor group at high risk for situations affecting their health and well-being. Specifically, in scenarios of health system reform and privatization of services, job insecurity has increased, and job satisfaction has decreased [3] while work has intensified [4]. As demands at work increase, a sustained rise in the physical and cognitive effort is required, which in the long term depletes the worker’s resources, leading to the development of various health problems, including burnout syndrome [5].
Social identification is conceptualized as a multidimensional construct with several elements that act in coordination to produce the influence that belonging to a group has on self-concept [6]. One of the elements of the social identification construct is the cognitive one, which includes a sense of unity between the workers and their organization, this element is self-defining and shapes the way in which the members of a group think about themselves [7, 8]. This component is the main focus of organizational studies based on a social identification approach. Another component is the evaluative element, which analyses the value that each individual places on their belonging to a group and ultimately determines what they think and feel about themselves [6].
According to social identity theory, organizational identification is the psychological bond that connects people to their organizations. As stated by Mael and Ashforth [9], evidence shows that this internalization that the individual makes of his or her relevant group in the work context is essential for the presence of stress or burnout [10]. However, the results on the effect that organizational identification could have on health are controversial. Organizational identification can take on a wide range of possible values, including a positive relationship based on greater control, support, and resilience [11]; an absent relationship [12], or a negative relationship based on a higher commitment, leading to more hours worked and subsequently to burnout [13].
On the other hand, organizational justice expresses the degree to which individuals believe that the results they receive and how they are treated within an organization are fair, equitable, and in sync with moral and ethical principles [14]. The most popular classification of the dimensions of this construct includes distributive justice, referring to fairness in the comparison that each worker makes about his or her contributions and results with others inside and outside the organization, and procedural justice, referring to the fairness that members of an organization feel in the decision-making process [15, 16]. Later, in 1986, a new dimension called interactional justice was introduced [17], defined as perceived fairness in interpersonal dealings. A subsequent study postulated that this last dimension of justice should be divided into two to broaden its discriminating capacity: interpersonal justice, understood as fairness in interpersonal behavior of courtesy, dignity and respect received during decision-making on procedures and distribution of results, and informational justice, referring to fairness in terms of explanations and information provided by management during decision-making[18].
Organizational identification processes comprise, in turn, social comparison processes, according to a worker’s categorization of his or her organization and himself or herself as an employee [19]. According to social identity theory, a worker’s evaluation of the stressors to which he or she is exposed depends on his or her self-categorization as a member of a group [20]. These comparisons can lead to perceptions of organizational justice/injustice [21]. According to the group value model, a high perception of organizational justice can make individuals feel respected and proud to be part of an organization, enhancing their identification [22].
Reports show that the relationship between organizational identification and organizational justice can occur in two ways: directly, from the observed association between the two constructs, and indirectly, as an effect on other organizational behaviors. Directly, the correlation between the level of overall organizational justice and organizational identification was moderate and significant, showing a strong relationship between employees’ perception of justice and view of managers and their levels of organizational identification, in a study of 1223 teachers [23]. Indirectly, a report from Gulluce and Kahyaoglu showed that overall organizational justice and its dimensions could be associated with organizational identification behavior, and procedural justice was the strongest predictor [24].
Cristina Maslach [25] conceptualizes burnout as a response to chronic stress that leads to professional burnout and originates in the work context. This syndrome consists of three independent but related dimensions: emotional exhaustion, referring to physical and emotional fatigue occurring in the absence of resources to cope with the demands of work; reduced personal achievement, referring to feelings of incompetence and lack of personal achievement at work; and depersonalization, denoting negative, apathetic, and indifferent responses to people and one’s work. The organizational theory postulated that organizational stressors are the most relevant in the origin of burnout. Among these factors are identification and organizationaljustice.
Burnout syndrome is considered a public health problem [26] due to its increasing incidence rate, adverse effects on workers’ health and well-being, and impact on the health system. Currently, this syndrome has migrated from an explanation based on personal factors to predominant organizational factors. Several studies have reported the relationship between the identification that a worker has with his or her organization or work team and its decrease in the presence of burnout [27, 28].
Regarding organizational justice and burnout syndrome, an inverse relationship has been observed in different studies. In this regard, Brotherige indicates that distributive and procedural justice are associated with emotional exhaustion in bank employees [29]. In teachers, Loerbrocks et al., observed that low levels of organizational justice and high levels of effort-reward imbalance were independently related to a higher probability of suffering burnout syndrome and considering the possibility of leaving the teaching profession [30]. Likewise, procedural justice had a significant adverse effect on teachers’ emotional exhaustion and personal fulfilment, although not on the depersonalization dimension [31]. In another study, Topbaş et al. took a sample of nurses, finding a statistically significant negative association between emotional exhaustion scores and perceptions of distributive, procedural, and informational justice, while scores on the depersonalization scale were only negatively associated with distributive justice [32]. Thus, based on empirical evidence, it is considered that the perception of injustice in the workplace acts as a direct stressor to which chronic exposure can lead to burnout syndrome.
In addition to a direct effect, there is also empirical evidence indicating that organizational justice has a mediating effect between some organizational behaviors and the genesis of burnout syndrome [33]. Specifically, the evaluation of justice that an individual makes about his or her workplace can modify this syndrome’s development.
Prior research has provided initial support for the direct relationship between organizational identification and burnout. However, to our knowledge, no other study has investigated if this relation could be mediated by the employees' fairness perceptions. The present study aims to close this gap by testing the potential indirect effect of organizational identification over burnout, through the mediating influence of organizational justice perceptions, and assessing the differential role of justice dimensions, in a multioccupational group of healthcare workers.
Considering the theoretical and empirical background, the objectives of the present study were: To evaluate the association between organizational identification and burnout syndrome in healthcare workers, and to determine whether the perception of organizational justice mediates this relationship.
Hypothesis:
H1: Organizational identification is negatively related to burnout syndrome.
H2: Perceptions of organizational justice (distributive, procedural, interpersonal, informational) are positively related to organizational identification (H2a) and negatively related to burnout syndrome (H2b).
H3: Perceptions of organizational justice (distributive, procedural, interpersonal, informational) mediate the relationship between organizational identification and burnout syndrome.
Methods
Participants and procedure
This research adopted a quantitative, observational design.
It was framed within the guidelines of the associative-explanatory [34], since its purpose was to explore the functional relationships between a particular group of variables to explain their behavior. According to Ato et al., three characteristics allow to operationally define this type of non-experimental study: the existence of a single sample of participants that is not usually randomly selected; the measurement of two or more variables that are generally of a quantitative nature; and the availability of a correlation or a covariance matrix for the statistical analysis. In this research, the explanatory design is composed of a measurement and a structural model, with both latent and observed variables. These models are known as structural equation models (SEM) [34].
The participants were convenience sampled from four healthcare organizations. In the case of this study, the census constituted 569 healthcare workers (physicians, nursing professionals and nursing assistants) employed at all four healthcare organizations (3 private and one public) in the city of Medellín, with a minimum work seniority of six months who were invited to complete the questionnaire. Pregnant workers were excluded since, according to Colombian legislation, they are considered a vulnerable group for research [35]. Questionnaires that registered more than 10% of missing data werediscarded.
The present study was subject to evaluation by the Ethics Committees of CES University (code 869-CI) and the participant health organizations. Participation was always anonymous and voluntary and required the signature of an informed consent form. No incentives were offered to respond to the survey.
Measures
Organizational justice
Participants’ perceptions of organizational justice (OJ) were explored using Colquitt’s Organizational Justice Scale [36], validated for Colombian workers by Ruiz-Suarez et al. [37]. This instrument contains 20 items classified into four dimensions: procedural justice (7 items; α= 0.71; e.g., Have the procedures for giving rewards been applied consistently in the same way to all employees?), distributive justice (4 items; α= 0.90; e.g., Do your rewards reflect the effort you have put into your work?), interpersonal justice (4 items; α= 0.75; e.g., Has your boss or supervisor avoided inappropriate jokes or comments?) and informational fairness (5 items; α= 0.84; e.g., Have explanations regarding procedures for rewarding you been reasonable?). All items were rated on a five-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). The average of each dimension obtained a score from 1 to 5; the higher scores indicated a greater perception of fairness, and the overall reliability was .94.
Organizational identification
Organizational identification (OI) was measured using a five-item scale developed by Mael and Ashforth [38] and adapted to Spanish by Walesska Schlesinger et al. [39]. In addition, in the study conducted by Jones and Volpe, a Cronbach’s α coefficient of.79 was obtained [40]. Respondents were asked to report their levels of perceived oneness with their workplace. Items included, “When I talk about my organization, I usually say ‘we’ rather than ‘they”’, “when someone criticizes my organization, it feels like a personal insult”. In this current study, the Cronbach’s alpha coefficient was .80.
Burnout syndrome
Burnout syndrome (BO) was measured through the Maslach Burnout Inventory - Human Services Survey (MBI-HSS), developed by Maslach and Jackson [41]. This instrument was specifically designed for service professions and captures three dimensions of burnout: emotional exhaustion, depersonalization, and diminished personal accomplishment. The inventory consists of 22 items classified as follows: Emotional exhaustion (EE): (9 items, α= 0.75) measuring the feeling of being emotionally drained by job demands, e.g., I feel emotionally exhausted by my job. Depersonalization (D): (5 items, α= 0.70) measuring the degree of distance, feelings, and coldness related to the care subject, e.g., I do not really care about what happens to some of the people I serve. Personal achievement (PA): (8 items, α= 0.79) measuring the degree of job satisfaction and feelings of competence, e.g., I have achieved many valuable things in this job. Each item is scored on a Likert scale ranging from 0 (never) to 6 (every day).
Data analysis
Initially, descriptive and correlation analyses were performed for all the variables in the study. Next, the proposed theoretical model was tested using the statistical package Mplus v.8.6. Two competing structural equation models were evaluated. The Structural Equation Modelling (SEM) technique allows testing models including latent variables with complex relationships. For instance, SEM can help researchers to validate partial or full mediation models including variables measured with multi-item scales. In our study, we initially tested a partial mediation model, considering H1 (i.e., a direct relationship between OI and BO). We also validated a second model where the perception that organizational justice mediates the effect of OI on BO. There were certain breaches to the normality assumption; therefore, we used the maximum likelihood estimator with robust standard errors (MLR). The goodness-of-fit of the SEM models was assessed using the following indexes: chi-square (χ2), comparative fit index (CFI), and root mean standard error of approximation (RMSEA). An adequate goodness-of-fit was indicated by χ2 not significant 3, CFI close to.95, and an RMSEA close to.06 [42]. Because χ2 is sensitive to sample size, correlations of residuals were analyzed to detect local sources of a misfit. Correlations of residuals greater than.30 indicated dependence between responses [43]. For factor loadings, a criterion value of <0.40 was assumed [44]. Covariates were only included in the analyses if they were associated with B.O. (P < 0.05) in separate regression analyses. Accordingly, we included age, daily working hours, and gender.
Results
In total, 402 of 569 workers responded to the survey, representing a response rate of 70.65%. The participants (283 women and 111 men) had a median age of 33 years RIQ (28–40) and a median length of service of 5 years RIQ (2–10)±7.38 years. In addition, 44.6% had a single marital status. The highest proportion of participants had a technical level of education (45.3%), and university education (24.4%). Moreover, 34% were physicians, 15.7% were nursing professionals, and 50.2% were nursing assistants. Most of the participants worked in the hospitalization service (35%). Table 1 presents the characteristics of the participants in the sample studied.
Characteristics of the sample under study
Characteristics of the sample under study
The initial structural model included the three dimensions of BO separately and showed a poor fit (χ2= 2670.89, df = 1058, p = 00; CFI = 0.82; RMSEA = 0.06). Moreover, to reduce model complexity and maintaining the three dimensions of BO, the scales of the MBI-HSS were parsed. Indicator 15 was omitted in this operation since its factor loading in the depersonalization dimension was below the expected value. Additionally, the procedural and informational justice dimensions did not significantly correlate with any of the BO dimensions. Therefore, these perceived justice dimensions were eliminated from the model. The distribution of the retained items is shown in Table 2.
Descriptive statistics of the retained items
As a result of these additional specifications, the selected indexes showed that partial and full mediation models fit satisfactorily (Table 3). Although the χ2 proved significant, analysis of the correlations of the residuals did not indicate local misfits. No differences in fit were observed in any of the other coefficients. However, in the specific results of the partial mediation model, the direct relationship between OI and BO was not significant (β= –0.16; p = 0.07). Therefore, the total mediation model was selected.
General fit of the structural models
Additionally, results of the total mediation model showed that the indirect effects of OI on BO through perceptions of distributive justice and interpersonal justice were significant. These results suggest that both DJ and INTJ mediate the effect of OI on BO. The standardized total and specific indirect effects are displayed in Table 4.
Standardized total and specific indirect effects
Thus, the rejection of the partial mediation model, the non-existence of a direct relationship between OI and BO in the model, would indicate that the study’s first hypothesis (H1) is rejected. However, the full-mediation model validated in our study suggests that OI and BO are related, but indirectly (Table 3). Noteworthy, the indirect effect of OI on BO specified as part of the validated model resulted negative and significant (Table 4). Therefore, the results of our study suggest that the negative relationship between those variables exists but is indirect (Fig. 1).
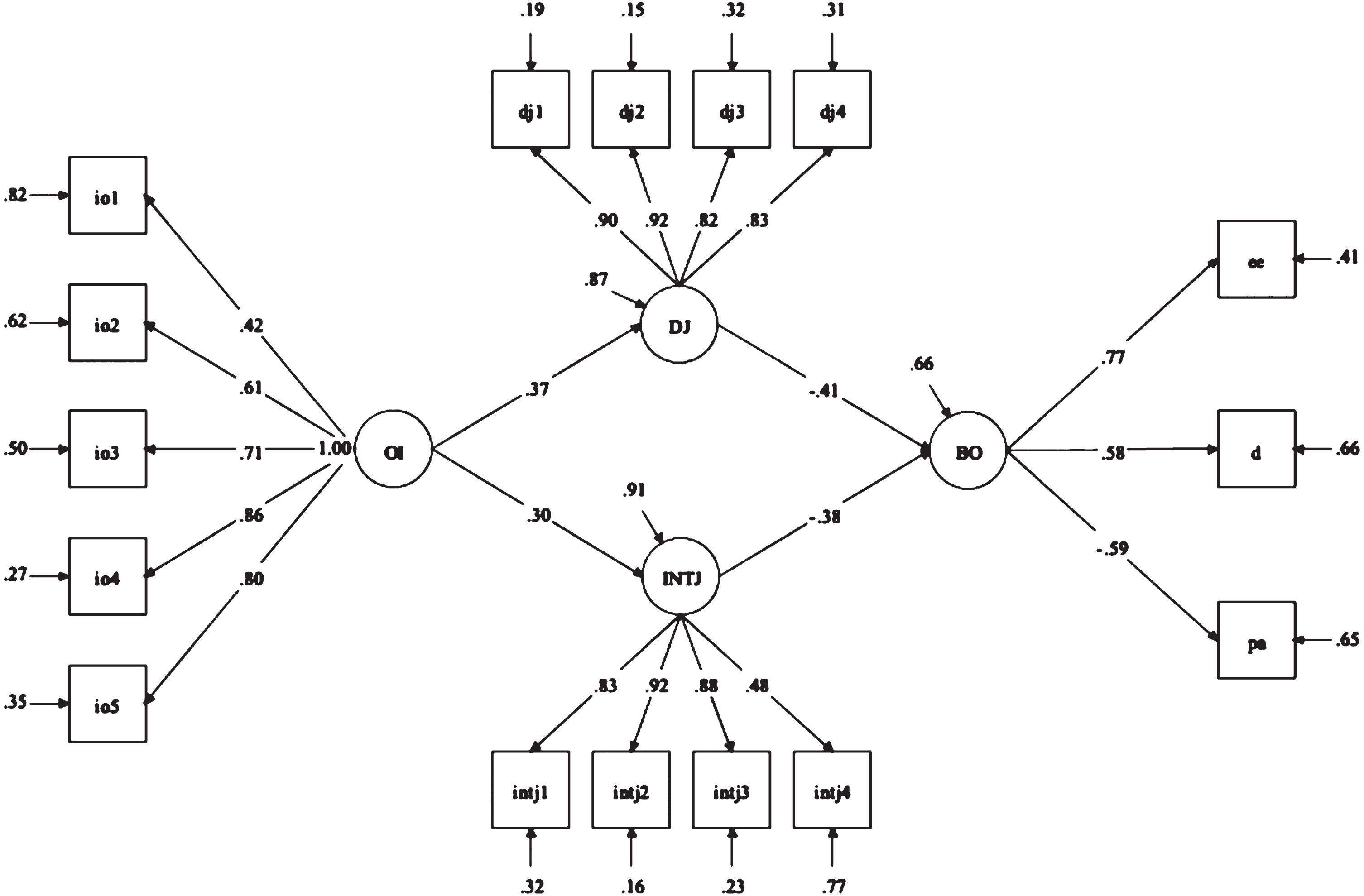
Structural model of total mediation. N = 402; Estimator = MLR; All coefficients significant at the P < 0.01 level.
Noticeably, after introducing the control variables, the model estimates continued to be significant. The correlations between the latent variables of the model and the controls are shown in Table 5.
Correlation matrix
Note: **significant at P < .01; *significant at P < .05. The correlations, means, and dt of the factors were generated depending on the items retained by the structural equation analysis. Hence, they are presented after the latter.
Concerning the other two hypotheses of the study (H2 and H3), whereas DJ and INTJ proved to be mediators of the effect of OI on BO, the procedural and informational dimensions were not kept in the model. Perceptions of organizational justice is a multidimensional construct and we only found support to assert that two out of four of its dimensions mediate the effect of OI on BO. Specifically, our results suggest that the distributive and interpersonal dimensions of organizational justice were related to OI and BO and mediated the effect of the former on the latter variable.
This study aimed to evaluate the association between organizational identification and burnout syndrome in healthcare workers, specifically physicians, professionals, and nursing assistants, and determine whether perceptions of organizational justice mediate this relationship.
Our findings generate empirical evidence for a broader explanation of the effect of organizational identification on healthcare workers’ perceptions of justice and the effect of these perceptions on the presence of burnout syndrome. In addition, the proposed model was adequate, and adjustments in specific pathways enhanced it, following the expected values of the fit indexes.
Although evidence points to a beneficial effect of organizational identification [12], in our study, it did not have a direct protective effect on the presence of burnout in healthcare workers, consistently with other relevant studies [45, 46]. Like our results, the effect between organizational identification and burnout appears to occur through the mediation of other factors. For example, Avanzi et al. reported an indirect negative effect between identification and burnout via collective efficacy and social support [47] and, subsequently, peer support and workload [48]. A possible explanation of the absence of a direct effect could be the mediating variables influencing this relationship. For example, it is possible that in our study sample, the levels of collective efficacy and social support are low, which would result in a non-significant association.
Our study postulates an additional indirect relationship through the perception of organizational justice, mediating the relationship between organizational identification and burnout syndrome. According to the results of previous studies, it could be confirmed that the perception of organizational justice behaves as a protective factor against burnout [32, 50].
Concerning our study, the most significant difference between the proposed and final models is eliminating procedural and informational justice perception due to a lack of solid and significant correlation with burnout syndrome. In addition to motives to maximize model fit, studies established that although all dimensions of organizational justice behave as essential predictors of occupational outcomes [51], they act differentially. Since perceptions of distributive and interactional justice have been connected to a greater extent to individual outcomes such as job satisfaction and intention to quit [52, 53]. This is in line with the report by Yuan et al., who, through the theory of social identity, explained the impact of organizational justice on job satisfaction [54].
Our results suggest that the perception of distributive justice is a critical mediating element in the relationship between organizational identification and burnout syndrome. These findings align with Greenberg’s theoretical perspective on the connection between injustice and stress [55]. It shows that distributive injustice is a form of stressor; more specifically, it is considered a demand that affects the individual, generating burnout by investing resources to cope with it. Alternatively, in the mediation model, the dimension of procedural justice did not have a significant relationship with the dimensions of burnout, coinciding with Moliner’s report [56]. However, other studies proposed an interaction between these two dimensions of organizational justice that is more likely to be observed when workers have a higher organizational identification [57]. Likewise, the procedural dimension of justice is more relevant when favorable outcomes in the work environment are analysed [58]. Li, provides another potential explanation for this finding, arguing that the value that individuals attribute to distributive and procedural justice differs according to the cultural context surrounding their work and the occupational group to which one belongs [59]. This explanation coincides with the results reported from German and French teachers, whose perception of distributive justice was negatively associated with burnout [60]. However, the perception of procedural justice was only negatively associated with burnout in the group of teachers from Germany, which could be possibly explained because the French educational system is hierarchical, and its individuals seem to pay less attention to procedural justice information. Liljegren and Ekberg, examining the cross-sectional and 2-year longitudinal associations between perceived organizational justice, self-rated health and burnout, concluded that the global justice construct showed better goodness-of-fit indices than the threefold justice construct, but a differentiated organizational justice concept could give valuable information about health-related risk factors, therefore it is important to assess these two approaches as complementary [61].
Interactional justice makes individuals feel valued within an organization and provides them with information about their social relationships within the group [62]. In fact, according to Cropazano and Folger, workers’ judgments about this dimension require less information than judgments about distributive or procedural justice because they refer to the immediate environment and experiences in the workplace [15].
Our results should be interpreted considering a set of limitations. First, the cross-sectional nature of the research design limited the conclusions about the causal relationship between the variables. Second, the variables were measured through self-report instruments, possibly leading to overestimating associations due to shared variances. Consequently, to remedy the latter, we used procedural resources, such as separating the questions in the questionnaire so that cause and effect relationships could not be established, indicating to the respondents that there were no correct or incorrect answers to the questionnaires. This study has a limitation in generalizing the results because convenience sampling was used to obtain participants.
Future research perspectives concerning organizational identification should address the measurement of other variables that may mediate the relationship with burnout. Likewise, regarding organizational justice, we propose developing longitudinal studies, using the sequence of action of different dimensions of justice more explicitly, understanding how these perceptions change over time, and defining which dimension has a more significant effect on the others to facilitate intervention in health professionals. It is also important to replicate this study in other occupational groups with different work environments and conditions.
Conclusion
The model established in this study provides an important theoretical basis for studying organizational identification, organizational justice and burnout. First, it can be concluded that there was not a direct protective effect of organizational identification on burnout in healthcare workers, but organizational identification has an indirect influence on burnout by the mediation of organizational justice. Secondly, among the four dimensions of organizational justice, the perception of distributive justice is a critical mediating factor in this relationship, and procedural justice did not have a significant effect on burnout. Thus, our findings provide more effective theoretical guidance to understand the model of organizational identification and burnout, clarifying the role of organizational justice.
We expect that the study results draw attention to occupational health practice regarding the organizational factors that should be intervened to reduce burnout syndrome in healthcare workers. Moreover, it is necessary to develop initiatives to increase the levels of organizational identification through communicative strategies and socialization practices, besides creating a fair organizational environment, where forms and procedures for the distribution of rewards are explicit, and the treatment received by workers is perceived as fair. Besides, all these conditions should be a priority in future research and intervention of burnout.
Ethical approval
The study was approved by the Ethics Committees of CES University (code 869-CI) and the participating health organizations.
Informed consent
All workers gave their written informed consent to participate in this study.
Conflict of interest
The authors declare no potential conflicts of interest concerning the article’s research, authorship, or publication.
Footnotes
Acknowledgments
The authors warmly thank Clinica CES, Clinica Noel, Clínica Santa Ana, and Institución Prestadora de Servicios de Salud IPS Universitaria.
Funding
The authors did not receive financial support for the development of the research.