
Abstract
Background
Many studies have shown the renoprotective effect of angiotensin-converting enzyme inhibitors (ACEi) and angiotensin II receptor blockers (ARBs) in patients with chronic kidney disease stages I–IV. Two randomized controlled trials (RCTs) showed a positive effect of AII inhibitors on residual glomerular filtration rate (rGFR) in peritoneal dialysis (PD) patients. However, these studies were small and were performed in a highly selected group of PD patients. Our aim was to confirm the above findings in a larger number of prospectively followed PD patients.
Methods
First we analyzed the time course of decline of rGFR in 452 incident PD patients that were not anuric at the start of dialysis and that had structured follow-up data, with measurements at 3, 6, 12, 18, 24, 30, and 36 months after the start of dialysis. Changes in rGFR over time were analyzed with a linear mixed model for repeated measures. In addition, Cox regression models were used to estimate the risk of developing anuria. In a second approach, we aimed to repeat the above analyses in a selected group of patients that theoretically could have been randomized and therefore resembled the population studied in the 2 mentioned RCTs. In this group the follow-up was restricted to 1 year.
Results
201 patients were treated with ACEi/ARBs and 251 did not take these drugs at the start of PD. More patients from the treated group had diabetes and used more antihypertensive medications. The time course of decline of rGFR was not different between the 2 groups over the 3 years of PD treatment (p = 0.52). Less than 25% of patients from each group became anuric and there was no difference in time to development of complete anuria between the treated and untreated groups. In the second approach, 130 patients were included: 37 were treated with ACEi/ARBs and 93 were not. Again, no difference was found between the 2 groups with respect to the rate of decline of rGFR and time of anuria development.
Conclusion
Our findings are not in line with the results of previous RCTs. The biggest limitation of observational studies is the inability to avoid confounding by indication. However, a RCT in such a setting also does not give a reliable answer. Given all the benefits of ACEi/ARBs, the medications should not be withheld from PD patients. However, their renoprotective effects may often be overruled by other factors influencing the time course of rGFR.
The aim of our study is to confirm the results found in the RCTs in a large cohort of PD patients with a long prospective follow-up, using both intention-to-treat and as-treated designs.
Methods
Patients
The patients were selected from the database of the Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD). This was a large, prospective, multi-center cohort study in which patients with end-stage renal disease from 38 dialysis centers in The Netherlands were followed from the initiation of dialysis until transplantation or death. At the start of dialysis, all patients were older than 18 years and had never received renal replacement therapy in the past.
All 585 incident patients that had started renal replacement therapy with PD in the period between 1 January 1997 and 1 July 2007 were considered for the current analyses. In order to study the time course of rGFR, the patients that were anuric already at the start of PD therapy were excluded. To be included, patients had to have a measurement of rGFR available at the time point 3 months after the start of dialysis as well as data on the use of ACEi, ARB, and other antihypertensive medications (β-blockers, calcium channel antagonists, diuretics). After inclusion, patients were followed for as long as PD therapy continued.
Data Collection
Demographic data, as well as data on comorbidity and primary kidney disease, were collected within 1 month prior to the start of dialysis treatment. During the follow-up, data on blood pressure, proteinuria, body mass index, use of antihypertensive medications, and RRF were collected at 3, 6, 12, 18, 24, 30, and 36 months after the start of dialysis.
Primary kidney disease was classified according to the codes of the European Renal Association–Dialysis and Transplantation Association (ERA-EDTA)–European Renal Association Registry (16). Using the Davies’ Comorbidity Index, comorbidity was scored as none, intermediate, or severe based on the number of comorbid conditions (17). Cardiovascular disease was recorded if one of the following conditions was present: angina pectoris, myocardial infarction, congestive heart failure class III–IV, peripheral vascular disease, or cerebrovascular accident.
Residual renal function was expressed as rGFR and was calculated as the mean of 24-hour creatinine and urea clearances corrected for body surface area (mL/min/ 1.73 m2). A 24-hour urine collection was done prior to the monitoring visit at the outpatient clinic and a blood sample was drawn at the visit. The rGFR was set to zero when urine production was < 200 mL/24 hours. When a patient had a rGFR of zero at two consecutive time points, he was defined as anuric from the first time point that the rGFR was zero.
The use of ACEi/ARB as well as other antihypertensive medications was documented “yes” or “no” at every checkup time point (see above). When “yes” was indicated, the patient was considered to have used the medication during the period preceding the check-up.
Analysis of Data
To study the time course of rGFR with respect to the use of ACEi/ARB, two different approaches were applied. In the first, we performed an analysis of the cohort on an intention-to-treat basis. All included patients were assigned to either the ACEi/ARB group or the control group based on the use of the medication during the first 3 months of PD treatment. When a patient used ACEi/ ARB during this period, regardless of taking these medications before the start of dialysis, this patient was assigned to the treatment group. If ACEi/ARBs were not taken at the start of PD or during the 3 months after the start, the patient was included in the control group. After that, we compared the time courses of rGFR between the groups for the 3 years of follow-up.
In the second approach we aimed to create conditions similar to those of the two referenced RCTs. Therefore, we restricted our study to a 1-year follow-up and included only those patients that theoretically could participate in the randomization process. For this purpose we selected those patients that survived for at least 1 year on PD and excluded those with strict indications for ACEi/ARBs, such as myocardial infarction, congestive heart failure, cerebrovascular accidents. Unlike in the RCTs, we performed our analysis on an “as treated” basis and therefore included only those patients that had been continuously treated with ACEi/ARBs in the first year of PD (ACEi/ARB group) and those who had not received these medications in this period (controls). The time course of rGFR during the first year on PD was compared between the two groups.
Statistics
To compare patients’ baseline characteristics we used standard descriptive statistics. Student's t-test was applied to compare continuous variables and the chi-square test was used to compare categorical data. To analyze the effects of ACEi/ARB medication on the decline of RRF, we constructed generalized mixed models for repeated measures. The random-effects mixed model with unstructured covariate matrix was applied to study differences in rGFR over time between the two groups. The multivariate model contained rGFR as dependent variable and treatment group as well as the number of measurements (time) as independent variables. The independent variables were first analyzed separately and then with an interaction. In addition, the model contained mean arterial blood pressure, proteinuria, and the use of antihypertensive medications as repeatedly measured variables. We also made adjustments for age, gender, diabetes, and cardiovascular disease as recorded at baseline.
In addition, we performed a Cox proportional hazards model to evaluate the risk factors for becoming anuric during the first 3 years of PD therapy with respect to treatment with ACEi/ARBs. The multivariate model contained age, gender, diabetes, cardiovascular disease, as well as rGFR, mean arterial blood pressure, and proteinuria at 3 months after the start of PD.
All statistical analyses were performed using SPSS statistical software, version 14.0 (SPSS Inc., Chicago, IL, USA). A p value of 0.05 or less was considered significant.
Results
Intention-To-Treat Analysis
Patients: Of the 585 incident PD patients, we excluded those who discontinued PD therapy within the first 3 months (n = 36), were anuric at 3 months after the start of dialysis (n = 34), or had data missing for rGFR during the first 6 months (n = 25). The remaining 490 patients were assigned to the ACEi/ARB or the control group. Patients that used these drugs at the start of PD but stopped right after it were excluded (n = 38). The remaining 452 patients were included for the current analysis. Those patients that used these medications at 3 months after the start of PD, regardless of taking them prior to the start of dialysis, were included in the treated group (n = 201). Those patients that had not used these medications at the beginning of dialysis or up to the first 3 months were assigned to the control group (n = 251).
Compared to the included patients, the excluded ones more often had cardiovascular disease, had lower rGFR, and used less ACEi at the start of dialysis. Other baseline characteristics were not different between in- and excluded patients.
Of the 201 patients from the ACEi/ARB group, only 90 started to use them after the first 3 months of PD.
Baseline characteristics of the studied cohort are summarized in Table 1. A difference in primary kidney disease was present between the two groups. This was due to a higher number of diabetics in the treated group. More of the ACEi/ARB patients used antihypertensive medications at the start of PD. In particular, patients from the treated group used diuretics and calcium channel blockers more often than controls. No other differences between the two groups were found. When comparing controls with the 90 patients that started to use ACEi/ARBs only after 3 months of PD, similar differences were detected (data not shown). With respect to PD modality, there was no difference in use of continuous ambulatory PD and automated PD between the two groups at any time point (data not shown).
Patients’ Baseline Characteristics at Three Months After Initiation of Peritoneal Dialysis (PD)
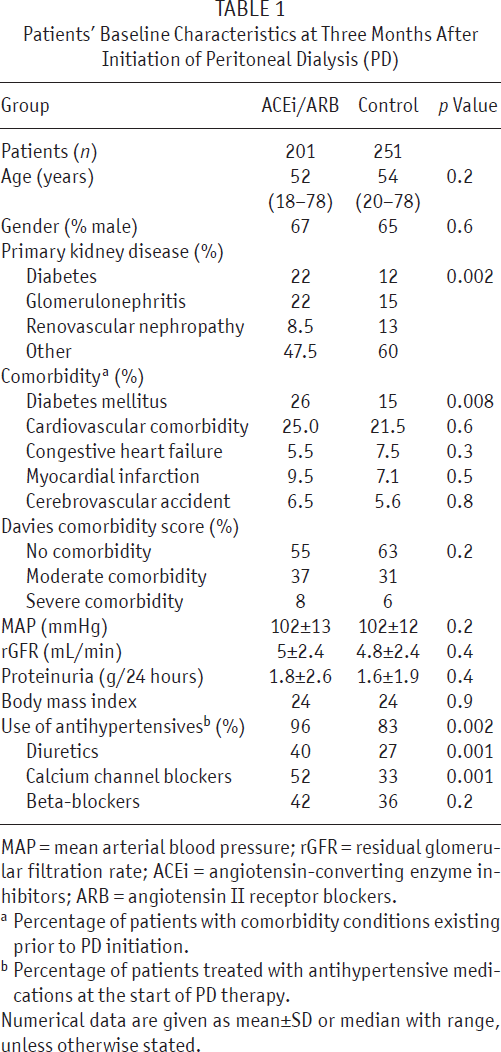
MAP = mean arterial blood pressure; rGFR = residual glomerular filtration rate; ACEi = angiotensin-converting enzyme inhibitors; ARB = angiotensin II receptor blockers.
Percentage of patients with comorbidity conditions existing prior to PD initiation.
Percentage of patients treated with antihypertensive medications at the start of PD therapy.
Numerical data are given as mean±SD or median with range, unless otherwise stated.
Decline of rGFR: To compare the time course of rGFR between the two groups during the first 3 years of PD treatment, we applied a generalized linear mixed model for repeated measures as described above. The results of the unadjusted analysis are shown in Figure 1(a). We found no difference in rate of decline of rGFR between the two groups (p = 0.49). Figure 1(b) presents the results of the adjusted analysis, which also showed no difference (p = 0.52).
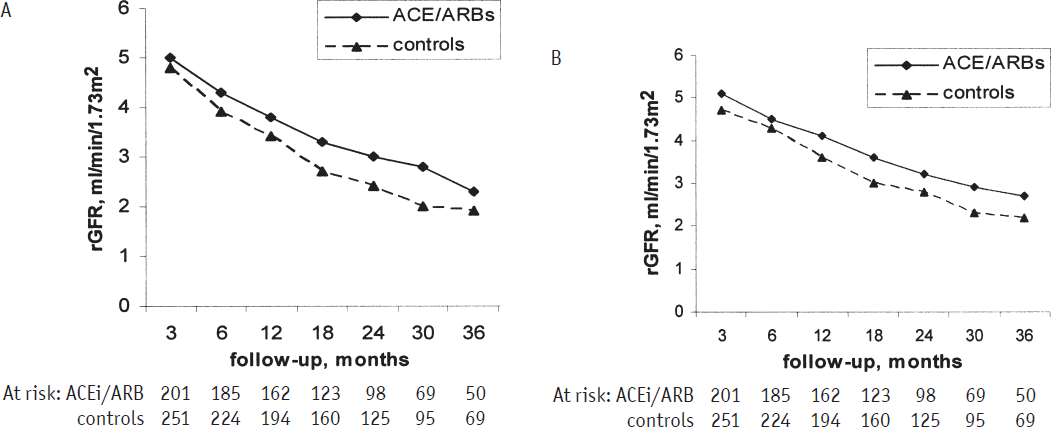
Unadjusted curves for decline in residual glomerular filtration rate (rGFR) were based on a generalized linear mixed model for repeated measures for all incident peritoneal dialysis (PD) patients with a follow-up of a maximum 3 years (A). Adjusted curves for decline in rGFR (B): Adjustments were made for mean arterial blood pressure, proteinuria, use of antihypertensive medications, age, gender, diabetes, and cardiovascular disease. ACE = angiotensin-converting enzyme inhibitors; ARB = angiotensin II receptor blockers.
Because the time course of rGFR could be influenced by baseline GFR, we repeated the mixed model analyses in subgroups of patients with low and high levels of GFR measured at 3 months after the start of dialysis. Subgroups were divided based on median rGFR values (4.6 mL/min/1.73 m2). The additional analyses showed a similar time course of RRF in the different subgroups (data not shown). In addition, because the time course of rGFR could be influenced by different durations of ACEi/ARB treatment, we repeated the analysis including into the treated group only the 90 patients that started to use the medications after they started dialysis. This change in design did not influence the outcome: no difference between the two groups was found (data not shown).
Due to dropout from the study because of transplantation, death, or switch to hemodialysis, we were able to record the development of anuria in only 20% of the patients. These were 49 patients from the ACEi/ARB group and 49 controls that became anuric within the 3 years of follow-up. In addition, we performed the Cox proportional hazards model to verify the relative risk of developing anuria with respect to the use of ACEi/ARB. A crude analysis showed a similar relative risk of becoming anuric for the treated group versus controls: hazard ratio (HR) 0.95 and 95% confidence interval (CI) 0.6 – 1.44. In the analyses adjusted for age, gender, diabetes, and cardiovascular disease, as well as for mean arterial blood pressure, proteinuria, and rGFR measured at the 3 months after the start of PD, the relative risk of anuria for the ACEi/ARB group versus controls showed no significant difference: HR 1.05 and 95% CI 0.61 – 1.48.
As-Treated Analysis
Patients: For the analysis based on the as-treated principle, we selected those PD patients that were not anuric at the start of dialysis and that remained on PD for at least 1 year. To be included, patients either had to be treated with ACEi/ARBs for the whole year or were not taking these medications at all during this period. We found 151 patients that fulfilled the above criteria. Additionally, to keep only the patients that theoretically could be randomized, we excluded those having severe cardiovascular comorbidity, that is, patients with congestive heart failure (7), myocardial infarction (13), or cerebrovascular accident (8) prior to the start of PD. Of the remaining 130 patients, 37 were treated with ACEi/ ARB during the first year on PD and the other 93 did not take these medications within the studied period. Comparison of the baseline characteristics is shown in Table 2. Patients from the treated and untreated groups had similar baseline conditions.
Baseline Characteristics of Patients in “As Treated” Analysis. Data Are Taken at Three Months After the Start of Peritoneal Dialysis (PD)
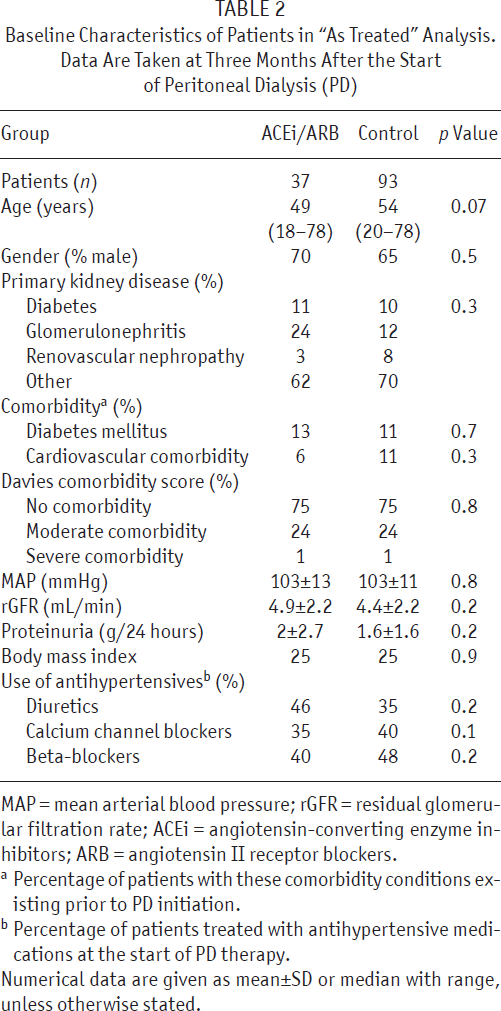
MAP = mean arterial blood pressure; rGFR = residual glomerular filtration rate; ACEi = angiotensin-converting enzyme inhibitors; ARB = angiotensin II receptor blockers.
Percentage of patients with these comorbidity conditions existing prior to PD initiation.
Percentage of patients treated with antihypertensive medications at the start of PD therapy.
Numerical data are given as mean±SD or median with range, unless otherwise stated.
Decline of rGFR: To compare the time course of rGFR between the two groups during the first year of PD treatment, we applied the general linear mixed model for repeated measures as described previously. The results of an unadjusted analysis are shown in Figure 2(a). No difference in rate of decline of rGFR between the two groups was found (p = 0.2). Adjustment for possible confounders did not bring a difference in the results (p = 0.23) [Figure 2(b)].
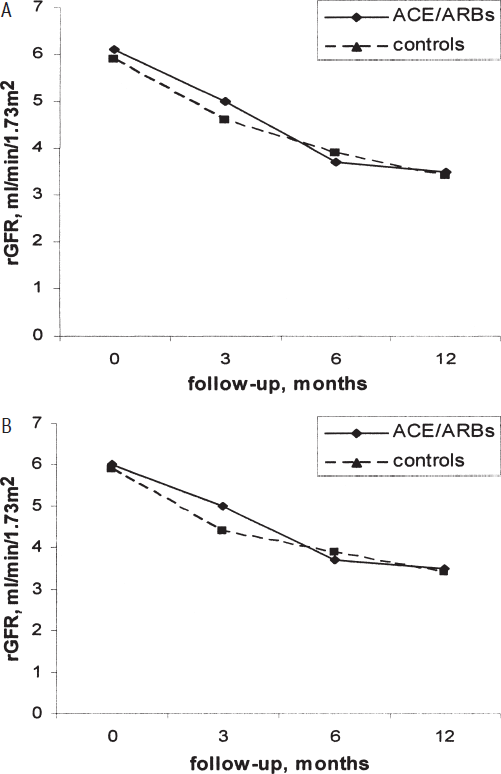
Unadjusted curves for decline in residual glomerular filtration rate (rGFR) were based on a generalized linear mixed model for repeated measures in as-treated analysis with 1-year follow-up (A). Adjusted curves for decline in rGFR (B): Adjustments were made for mean arterial blood pressure, proteinuria, use of antihypertensive medications, age, diabetes, and cardiovascular disease. ACE = angiotensin-converting enzyme inhibitors; ARB = angiotensin II receptor blockers.
One patient from the ACEi/ARB group versus 11 patients from the controls developed complete anuria during the first year of treatment (p = 0.1). Because less than 9% of patients developed anuria within the first year of PD treatment, the results of the Cox proportional hazards model were not informative (data not shown).
Discussion
The renoprotective effect of ACEi/ARB in PD patients as found in two RCTs could not be confirmed in the present prospective observational cohort study. This may be due partly to the selection of patients in the RCTs and partly to “confounding by indication.”
The first RCT on a potential renoprotective effect of the ACEi ramipril was done in 60 prevalent PD patients with a GFR ≥ 2 mL/min/1.73 m2 (14). Due to the exclusion criteria (congestive heart failure, myocardial infarction within the preceding 6 months, clinically significant valvular disease, malignant hypertension or hypertensive retinopathy, history of hypertensive encephalopathy or cerebrovascular accident within the preceding 6 months, or history of bilateral renal artery stenosis) 145 patients could not be enrolled. The HR for the development of anuria was higher in the ramipril group than in the controls at 3, 6, and 9 months. Only at 12 months, the ramipril group had a significantly lower HR. Accordingly, rGFR was higher in the ramipril group only at 9 and 12 months.
The RCT with the ARB valsartan was performed in 32 incident patients (15). The exclusion criteria were similar to those in the ramipril trial. Remarkably, the renal creatinine clearance showed a marked increase after 6 months, followed by a slow decline to a value at 24 months that still exceeded the baseline value. The controls showed an initial decline followed by more or less stable values. The discrepancy between the two RCTs is remarkable: the first showed a temporary decrease following the instillation of ACEi; the second reported an increase after ARB. It can be hypothesized that the relatively small number of patients in the two RCTs could be the cause of the discrepancy.
The largest observational follow-up study (1032 incident PD patients from the US Renal Data System) showed that the development of anuria was positively associated with the presence of diabetes mellitus and congestive heart failure (12). ACEi and calcium channel blockers were both independently associated with a longer duration of the development of anuria. These renoprotective effects of ACEi and calcium channel blockers could not be confirmed in an observational study in 146 incident PD patients from Australia (13).
In the present study, no effect of ACEi/ARBs on the decline of rGFR or on the development of anuria was found. This was the case when the whole cohort was analyzed and also when the exclusion criteria used in the two RCTs were applied. Only a tendency to a longer duration before the development of anuria was found in the latter analysis.
The difference with the RCTs could be partially explained by confounding by indication, also known as selection by prognosis. The distinct difference between RCTs and observational studies, such as cohort studies, is that RCTs can provide evidence for a causal relation-ship because they have the potential to avoid confounding by indication (18).
The patients most often prescribed ACEi/ARBs use these drugs because of hypertension, heart failure, and diabetes mellitus. These conditions themselves are associated with a more rapid decline of RRF (12,19,20). Diabetes, however, was not confirmed to be a predictor of anuria development in an earlier NECOSAD analysis (19). This might be due to a lower percentage of diabetics and other possible differences in the studied population. Also, it cannot be excluded that some patients were treated with ACEi/ARBs to slow the decline in rGFR, although the first RCT on this issue in PD patients was only published in 2003. Prescription of ACEi/ARBs to prolong survival may have occurred based on results from the studies in predialysis patients (21,22). A positive effect on survival in hemodialysis patients was published in 2002 (23), while in PD patients such an effect is controversial (24,25).
Our study has some additional limitations. First, information about treatment with ACEi/ARB before the start of dialysis is not available. It may be that some patients were taking the medications but stopped prior to dialysis initiation. This could have influenced our outcome. Second, it is unknown exactly why the patients were prescribed ACEi/ARBs.
We conclude that a number of factors make it difficult to assess the effects of ACEi/ARB on residual renal function in the general PD population. Bias, caused by confounding by indication, can never be excluded despite all the adjustments that can be made. Potential renoprotective properties of angiotensin II inhibitors in PD patients could be overruled by other factors that influence decline of rGFR. The results of the two published RCTs suggest a favorable effect but both were done in a limited number of selected patients and some of the results are contradictory. None of the studies suggested a harmful effect of these medications. Given the many established indications for ACEi/ARB treatment in PD patients, the threshold for prescribing them should be low.
Footnotes
This study was supported by the Renal Discoveries Extramural Grant Program of Baxtr Healthcare. The authors have no conflict of interest to declare.