
Abstract

It is relatively rare for a patient to spend more than two decades on peritoneal dialysis (PD). Here we report a male patient who underwent PD for more than 20 years.
The patient, a 42-year-old male, developed end-stage renal failure resulting from chronic glomerulonephritis in 1989. His creatinine level was 905 μmol/L but no creatinine clearance was measured. As he refused to accept hemodialysis, it was decided to start PD. In April 1989 a two-cuffed Tenckhoff catheter was inserted via a paramedian incision. After regular in-hospital training, he began home continuous ambulatory PD.
This patient was the third PD patient of our unit and he has always been treated and followed up at our unit. He is now 62.3 years old. His height is 1.68 m. In 1989 his body weight was 55 kg and it has been stable since 1989, at around 56 kg. He performed 2-L exchanges twice per day from May 1989 until March 1992 (Figure 1). At that time he was prescribed 6 L (4 L 2.5% dextrose, 2 L 1.5% dextrose) PD as he became oliguric and later anuric, developing fluid retention and fatigue, suggesting inadequate dialysis.
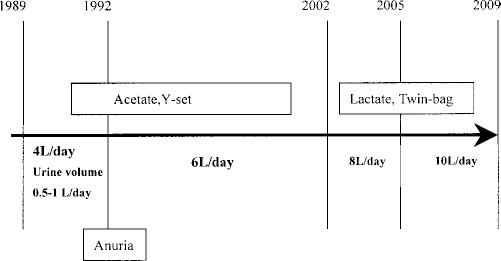
Follow-up during 20 years of treatment with peritoneal dialysis.
In 2002 the 24-hour volume had to be increased to 8 L (6 L 2.5% dextrose, 2 L 1.5% dextrose) due to low solute clearance. Three years ago, his prescription was changed to five exchanges in order to meet adequate ultrafiltration requirements.
The patient used a Y-connect system from March 1989 to July 2001, when he started using the Baxter twin-bag system, which he continues using without difficulty. He takes care of his exit site twice per week, applying povidone iodine and cleaning the site with sterile water, followed by application of a sterile dry dressing. The patient's dietary habits consist of several small meals during the day. Since 2001, he has been prescribed 12 – 15 compound α–ketoacid tablets to maintain his nutritional state.
This patient has never had any catheter problems and is still using the same two-cuffed Tenckhoff catheter that was inserted in 1989. He has had no tunnel or exit-site infection. He has had three peritonitis episodes but recovered successfully after treatment with antibiotics.
Over time, the patient's peritoneal permeability tended to rise (dialysate-to-plasma creatinine ratio increased from 0.66 to 0.82). Dialysis adequacy targets (Kt/V >1.7) have been achieved by gradually increasing the dose of PD. Serum albumin level suggested moderate hypoalbuminemia in the first 10 years of PD, but this improved in the second decade. Serum cholesterol and phosphorus levels have remained normal without treatment. The latest nutritional parameters are as follows: body mass index 19.6, serum albumin 33.5 g/L, total cholesterol 4.09 mmol/L, normalized protein catabolic rate 0.74, and protein intake 0.7 g/kg/day. He has mild anemia (hemoglobin 11.2 g/dL, hematocrit 35.1%) with erythropoietin treatment (100 U/kg/week). Subjective Global Assessment suggests mild malnutrition.
He reports no physical health problems except occasional fatigue and skin itching. His most recent hospitalization was in February 2009 due to volume overload. He stopped professional work when starting PD. His wife supports him in daily life and they have 2 children. He performs some physical activities every day.
Reports are available for a good number of patients that have survived on PD for 5 – 10 years (1,2). An analysis of 36 long-term patients from six North American centers showed that patients most likely to survive on PD for more than 10 years are relatively young at the start of PD, do not have diabetes, have few or no comorbid conditions, are female, have a low body weight, are well nourished, and have good family support. They also have low rates of hospital admission and peritonitis. It appears that, apart from the gender, our patient matches these criteria well. In addition, neither catheter-related mechanical (leak or bad drainage) nor exit-site infection was observed, likely contributing to an excellent technique survival (3). Although he was dialyzed by acetate-based dialysis solution for 13 years, he has not developed encapsulating peritoneal sclerosis (4).
His average hospitalization rate (23 days per year) is higher than that mentioned in the literature for a nondiabetic patient (5). Strict control of salt and fluid intake (<200 mL/day) help him overcome ultrafiltration limitations.
The presented case illustrates the potential for successful long-term PD treatment. Factors likely contributing to the outcome in this case include strong motivation, nondiabetic status, few peritonitis episodes, willingness to accept and comply to an increased dose, and dedicated family support.
Footnotes
The authors do not have any conflict of interests to declare.
Acknowledgment
The author is grateful for valuable comments on the manuscript by Anders Tranaeus, Medical Director, Baxter Asia Pacific, and Qiang Yao, Associate Medical Director, Baxter Renal, China.