
Abstract

Renal Replacement Therapy (RRT) in Latin America
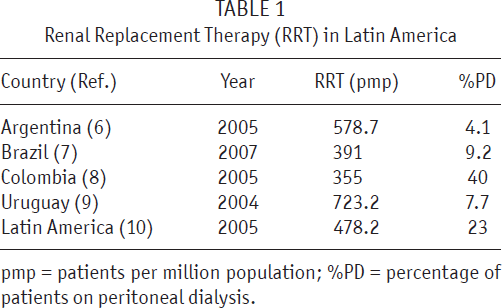
pmp = patients per million population; %PD = percentage of patients on peritoneal dialysis.
Argentina is a country in southern South America with a territory of 2791810 km2 (Figure 1). In 2007, its estimated population was 39356000 and its average population density was 14.1 inhabitants/km2 (14). That year, the Gross Domestic Product per capita was US$6050, life expectancy was 75 years, and 98.5% of children were enrolled in primary school (15). The National Health System (NHS) is covered by the Public Health System, the Social Securities, and the Private Health System. Through the Mandatory Medical Program, the NHS provides patients with a variety of essential services, such as hemodialysis (HD) and PD (16). In Argentina, the use of intermittent PD started in the 1960s. Toward the end of 1978, the first catheter for continuous ambulatory PD (CAPD) was implanted in a patient in Buenos Aires, with material produced locally. In 1980, Travenol materials became available, which reduced the rate of peritonitis from 1 episode every 4 months to 1 episode per year. In the late 1990s, PD became more widely known and had its main development (17). In spite of the rapid introduction of the double-bag system and the increased availability of cycling machines for automated PD (APD), the proportion of patients on PD compared to HD was still low, with a prevalence of only 5.5% at the end of the decade (18). Afterward, with the economic crisis in 2001, the cost of PD rose steeply and many patients had to be transferred to HD. At present, as will be discussed later, the use of PD is low.

Map of South America shows Argentina and main cities.
In 2004, the Sistema Nacional de Información de Procuración y Transplante de la República Argentina (SINTRA; National Information System for Procurement and Transplantation in Argentina) was created; it enables access to the Registro Nacional de Insuficiencia Renal Crónica Terminal (National Registry of Terminal Chronic Renal Failure). Because it is mandatory, this Registry shows the true number of patients currently on RRT in Argentina. It includes 95% of the patients and dialysis centers in the country (19). That report, prepared using SINTRA's data for the period 2004 – 2005, shows that, in 2005, 5416 new patients began treatment with chronic dialysis, which represents 140.34 patients pmp. However, only 2.3% initiated substitute therapy with PD. That same year, there were 26976 cases of patients on RRT, with a rate of 578.7 patients pmp, 4.1% on PD. There are 454 dialysis centers in Argentina, most of which are private and perform 93.9% of all RRT in the country. Of these 454 centers, 290 provide HD, 8 provide PD, and 156 provide both. This means that 34.4% of the centers are able to perform either HD or PD and 1.7% only PD. As the authors of the paper remarked, there is a large disparity between the availability of centers to perform PD and the prevalence of patients on PD (6). Even though there are dialysis centers that can do PD in all the provinces, 62% of such centers are located in Buenos Aires (20). Also, information about outcomes of patients on PD is scarce. There are only a few reports and many of them are in symposium papers with small numbers of patients (21-24). In this context, the Asociación Nefrológica Buenos Aires (Nephrology Association of Buenos Aires) organized the Peritoneal Dialysis Cooperative Study Group, which, in 2002, started a voluntary registry of patients and later a cooperative study, the aims of which were to describe patient characteristics and outcomes obtained with PD.
Materials and Methods
This was an observational, retrospective multicenter study in which 15 PD centers in 6 provinces took part. We studied prevalent and incident patients that started PD between 1 January 1992 and 31 December 2007.
Data Collection and Definitions of Variables
Demographic, clinical, and epidemiological data were obtained. During the observational period of the study, the spike system, twin-bag, and APD were used. However, patients were considered to be on CAPD or APD, depending on the treatment received at the moment of the study, regardless of any previous modality. Presence of diabetes mellitus and previous treatments with HD for 3 months or more (previous HD) were also recorded. Mortality, hospitalization days, incidence of peritonitis, and reasons for dropout from PD were evaluated. The dialysate-to-plasma ratio of creatinine in the fourth hour was obtained from the last peritoneal equilibration test carried out in each patient. Values of weekly total Kt/V urea and weekly total creatinine clearance/1.73 m2 (ClCr) were obtained from the average of the determinations performed during the last year of follow-up. Patients whose diuresis at the start of PD was lower than 100 mL/ day were considered anuric.
Statistical Analysis
To estimate patient survival, all patients that were transplanted, switched to HD, or lost to follow-up were considered censored. For technique survival, the outcome of interest was switch to HD or death due to peritonitis. Patients that died from other causes, received a transplant, or were lost to follow-up were also considered censored. The Kaplan–Meier method was used to calculate survival and time free of peritonitis, and the log rank method was used to compare survival curves. Hospitalizations due to creation of vascular or peritoneal access were not taken into account. Data are expressed as median ± standard deviation or as percentage, as appropriate. The confidence interval (CI) was estimated at 95% and a value of p < 0.05 was considered significant. The statistical analysis was performed with SPSS 7.5 (SPSS Inc., Chicago, IL, USA).
Results
Patient Characteristics
A total of 739 patients were studied: 52% males, 48% females; mean age 48.56 ± 16.08 years, 18.54% older than 65 years. Mean time of follow-up on PD was 33.8 ± 30.23 months (median 23.9 months). Table 2 shows the most relevant demographic and clinical data. At the beginning of PD, 66.7% of patients had been previously treated with HD for more than 3 months, for a mean time on HD of 48.2 ± 49.6 months (median 15.9 months); 60.1% of patients were on CAPD and 39.9% were on APD. Table 3 shows the main data for adequacy and membrane transport. Figure 2 shows distribution of transport characteristics determined by peritoneal equilibration test.
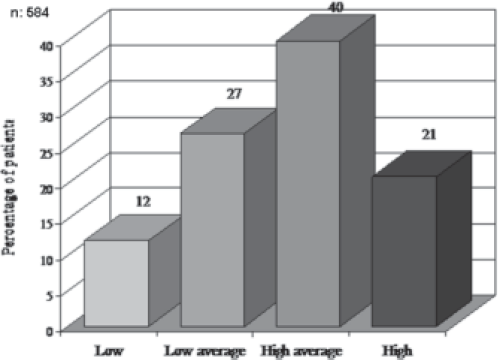
Membrane transport according to peritoneal equilibration test.
Demographic and Clinical Data
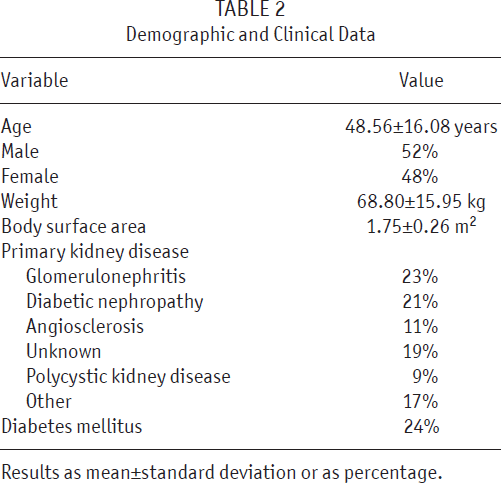
Results as mean±standard deviation or as percentage.
Mean Adequacy and Membrane Transport Data
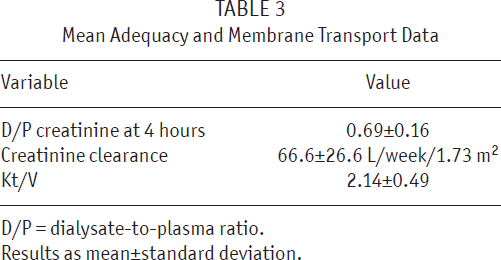
D/P = dialysate-to-plasma ratio.
Results as mean±standard deviation.
Outcomes
Of a total of 494 patients that dropped out from PD, 178 (36.0%) died, 201 (40.7%) were transferred to HD, 75 (15.2%) received a transplant, 38 (7.7%) were lost to follow-up, and 2 (0.4%) recovered renal function. The main reasons for switching to HD were peritonitis (54.7%), inadequate dialysis or ultrafiltration failure (22.1%), patient/family decision (15.6%), and other causes (7.6%).
Patient Survival and Mortality
The gross mortality rate was 8.41 deaths per 100 patient-years. We were able to determine the cause of death in 175 patients: cardiovascular in 90 (51.4%), infection in 59 (33.7%), and other in 26 (14.9%). Peritonitis was associated with 31% of deaths due to infection.
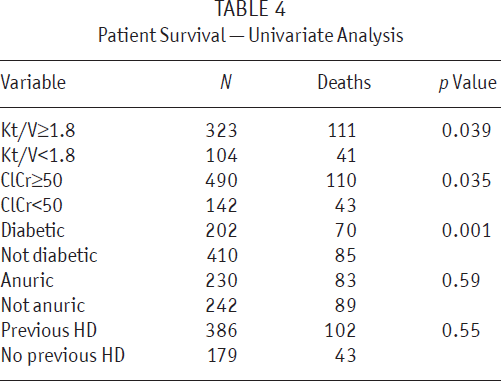
Patient survival after at least 3 months on PD (Figure 3) was 93%, 84%, 78%, 65%, and 50% at 12, 24, 36, 60, and 96 months, respectively. The univariate analysis (Table 4) showed a significantly higher survival rate in nondiabetic patients (p < 0.001), as well as in patients with Kt/V ≥ 1.8 (p = 0.039) and in those with ClCr ≥ 50 L/ week/1.73 m2 (p = 0.035). There were no differences in survival rates between patients with and patients without previous HD, or between anuric and nonanuric patients.
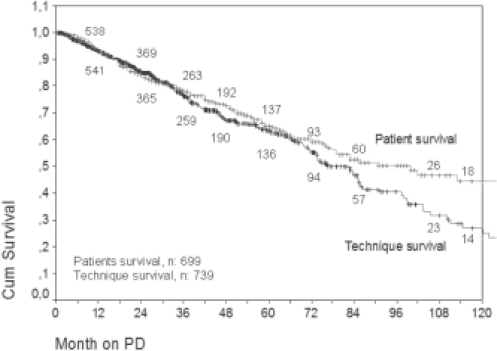
Kaplan–Meier plot for patient and technique survival. PD = peritoneal dialysis.
Patient Survival — Univariate Analysis
Morbidity
The hospitalization rate was 2.95 hospital days per patient-year; that is, there were 3548 hospital days in 1205 patient-years. Mean duration of hospitalization was 8.32 ± 12.8 days (median: 4 days).
At least 1 episode of peritonitis was observed in 437 of 739 patients (59.1%); the peritonitis rate was 0.47 episodes per patient-year, or 1 episode every 25.43 patient-months. The probability of remaining free of peritoneal infection was of 63%, 45%, and 31%, at 12, 24, and 36 months, respectively (Figure 4). Fifty percent of the patients had their first episode of peritonitis by 20.1 months (95% CI: 17.1 – 23.1).
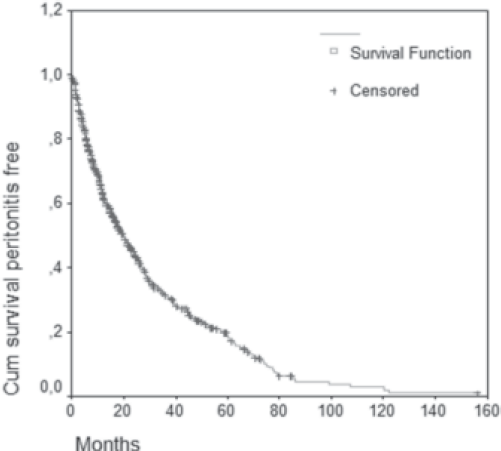
Kaplan–Meier plot for probability of remaining peritonitis free.
Technique Survival
As shown in Figure 3, technique survival was 93%, 84%, 74%, 61%, and 39% at 12, 24, 36, 60, and 96 months, respectively [median: 73.8 months (95% CI: 66 – 82)].
The main reasons for dropping out were peritonitis (54.7%), low ultrafiltration or inadequate dialysis (22%), patient/family decision (16%), and other causes (8%).
Discussion
Even though the prevalence of patients on RRT in Argentina is higher than the average for Latin American countries, the percentage using PD is very low. Considering that CAPD was introduced in this country three decades ago, and that 35.7% of the dialysis centers are able to provide this treatment, the number of patients on this modality should be considerably higher. The use of PD exceeds HD only in pediatric patients: 77.8% of patients younger than 4 years old and 52.6% of those under 10 are on PD as RRT. Above this age, its use decreases progressively (25). The prevalence of PD for all ages is 4.1%, which is one of the lowest percentages in the region and is similar to that in other countries where the use of PD is not frequent, such as Germany and Japan (1). Although there is no study explaining the low prevalence of PD in Argentina, and identifying the reasons for its low use is beyond the objectives of this study, many of the factors involved will be briefly explained here.
In 2006, the mean age of incident patients on RRT was 58.7 years, with 41.1% of patients over 65 years of age (25). Elderly patients have trouble with self-care, their spouses probably are old too, and their children or other younger members of the family are not available to aid them due to their own activities. In general, elderly dialysis patients require external help, which is not always available to them and this discourages them from choosing PD. Late referral is an important factor. It may be observed that 62.8% of patients that started HD in 2007 did so with a temporary catheter. They had been referred to a nephrologist late and did not have enough time to get acquainted with different options of dialysis (20). Another factor to consider is the medical residency programs, where the training of young nephrologists is biased toward HD and education on PD has a small place. Also, many nephrologists with more experience in their practice consider PD a second-line treatment that demands greater dedication and more time. All this negatively influences the younger generations of nephrologists, who also see a greater labor demand on HD. There are no financial incentives for physicians that may favor one or another modality of dialysis. The reimbursements given to the units providing dialysis may be up to 20% higher in PD. However, the most important payer pays the same amount (about US$1270 monthly) regardless of modality (HD or PD), which means US$106 per session of HD. In addition, in Argentina there are no local producers of PD supplies; reuse of dialyzers is allowed and some supplies for HD are manufactured locally, which may favor HD from the economic viewpoint. All these factors lead to less frequent use of PD. Most patients that start this treatment do so as a negative selection, having been transferred from HD due to exhaustion of their vascular access.
The Asociación Nefrológica Buenos Aires offers a course for PD that aims to teach and spread the use of this modality. This course is attended by nephrologists from different places in Argentina and from neighboring countries. In recent years, a steady increase in the use of PD as the first option in RRT has been observed. Between 1992 and 1996, 17 patients started PD; between 1997 and 2001, 103; and between 2002 and 2007, 119 (data not shown previously). Therefore, if this trend continues, an increase in PD use in the near future is expected.
In the past few years, there have been growing numbers of publications on PD coming from developing countries (8,12,13,23,26-30), but this present study is the first multicenter study that shows the state of PD in a large region of Argentina.
Patient survival is similar to that reported by other Latin American authors (12,27-30) and authors from other parts of the world (31-34). Univariate analysis showed lower survival in diabetic patients and in patients with Kt/V lower than 1.8 or ClCr lower than 50 L/week/ 1.73 m2. Diabetes mellitus is well-known to predict mortality (35,36), while Kt/V is more controversial and its increase beyond a certain level does not seem to improve outcomes (37). With respect to this, the evidence given by two clinical studies in patients on CAPD affirmed that Kt/V should not be lower than 1.7 – 1.8 (38,39).
It has been stated that those patients that start PD as their first dialysis treatment have better survival than those that are switched from HD (40), and that loss of residual renal function is considered an adverse prognostic factor in PD (41,42). Some studies, however, have shown that low levels of residual renal function do not predict mortality in patients that have been transferred from HD to PD but that malnutrition, comorbidity, low ultrafiltration (43,44), and advanced age (45) do predict mortality. In contrast to the findings of better survival of patients transferred from PD to HD, Van Biesen et al. did not find differences in those patients transferred from HD to PD (46), and neither did other authors (44,47). In Argentina (30) and in other countries in Latin America, as many as 80% of patients on PD may have been on HD previously (48). A Brazilian study points out that 75% of patients were transferred from HD to PD and that this predicted neither mortality nor technique failure (7). Although our population was relatively young and there were few diabetic patients, our results coincide with respect to transfer: 66.7% of patients that started PD had previously gone through HD but this did not influence their survival.
As reported in other series (49-52), the main causes of mortality were cardiovascular and infectious. Together they represent 85.1% of the total number of deaths. The gross mortality rate was 8.41 deaths per 100 patient-years. Technique survival at 5 years was 61% and the main reason for dropout was peritonitis, which was responsible for 54.7% of the switches to HD. Technique failure of and dropout from PD vary in different reports (53-55). With a follow-up period similar to ours, which was 33.8 ± 30.23 months, 17.4% of patients were transferred from PD to HD in Turkey (56) and 42.5% in Europe (EAPOS study) (44). Japan reported a 67.5% dropout rate (57). This high percentage could be due to the fact that the follow-up was longer (53.6 months). In our records, the dropout is 40.7%, the main reasons being, as mentioned in these publications, peritonitis and inadequate ultrafiltration/dialysis.
The peritonitis rate was 1 episode every 25.43 patient-months and the probability of remaining free of infection at 12 months was 63%. Surveillance of peritonitis rate and time free of peritoneal infection is a very important quality marker in PD programs. The values observed in our patients are acceptable according to the guidelines supported by the International Society for Peritoneal Dialysis (58). Hospitalization time as morbidity marker was lower than the one reported for PD by SLAHN in the region (2.95 vs 4.2 days/patient-year respectively) (59) and similar to other reports (33).
The six provinces that participated in this study comprise 59% of the country's chronic dialysis population (25) and 72.4% of prevalent patients on PD between 2004 and 2007 (Marinovich S, personal communication). Considering the study period, 1992 – 2007, this registry includes 65% of all PD patients in Argentina. However, as mentioned earlier, data from the National Registry of Terminal Chronic Renal Failure for patients on RRT are complete and controlled, as from 2004. For this reason, this last percentage might not be precise with respect to the numbers of patients included in the total population on PD during that period.
We acknowledge that this study is limited by being retrospective. Since this is a voluntary registry, there are limitations due to the willingness, motivation, and decision to participate of the different dialysis centers. However, the data here presented have no precedent since they reflect the main characteristics and outcomes of the largest sample of patients on PD in this country. The continuity of The Peritoneal Dialysis Registry and the study of its data might be valuable tools to obtain continuous improvement in the quality of and outcomes on PD.
Appendix
Participants of the “Registro Argentino de Diálisis Peritoneal”: Mabel Alvarez Quiroga, Roberto Barone, Carlos Bonzano, Marina Bravo, Eduardo Célia, Carlos Forlano, Jorge Lobo, Alberto Locatelli, Gustavo Marcos, Gustavo Moretta, Cesar San Martin, Jorge Schargorodsky, Horacio Trevisani, Cristina Vallvé, Eugenio Victor (Buenos Aires); Javier De Arteaga (Córdoba); Roxana Rodriguez (Mendoza); Irene Hendel (Neuquen); María de las Mercedes Alba, Elisa Morales (Rio Negro); Raul Cejas (Santiago del Estero).
Footnotes
Jorge Lobo: Medical Director, Fresenius Medical Care Argentina; Mabel Alvarez Quiroga: Medical Coordinator, Fresenius Medical Care Argentina; Irene Hendel: Medical Director, Fresenius Medical Care Argentina. Other authors declare that no financial conflict of interest exists.