
Abstract

Treatment of End-Stage Renal Disease (ESRD) in the UK
The Introduction of RRT to the UK: The provision of RRT for the treatment of acute renal failure started in the UK during and immediately after the Second World War (1). Michael Darmady, in Wiltshire, was among the first to use hemodialysis (HD), developing his own dialyzer based on the Kolff design (2). It was considered by some clinicians to be a barbaric treatment. Pioneered by Stanley Shaldon from Royal Free Hospital and Hugh de Wardener from Charing Cross, the application of HD to chronic renal failure began in 1962 following the first meeting of the International Society of Nephrology in Evian. It was decided to establish units for HD in each region of the UK and within 3 years there were 35 units providing dialysis for chronic renal failure patients (3). Peritoneal dialysis (PD) also began at this time, in both Newcastle and Edinburgh (3,4), initially in the form of intermittent PD performed on an inpatient basis. By 1978, as catheter connection technology improved, this method had been superseded by continuous ambulatory PD (CAPD) performed in patients’ own homes. The UK led the way in the field of renal transplantation in Europe at this time, having performed 138 transplants in 1969 (5) and 9054 by 1981, compared to 3432 in the Federal Republic of Germany and 1036 in Spain (6).
Increasing Incidence of Treated ESRD: Over the past 30 years there has been increasing provision of RRT, with rising numbers of incident RRT patients. The relative proportions of this increase, which are from increasing disease incidence as opposed to unmet need (patients previously not treated), have not been accurately studied. There is some evidence that the incidence of ESRD has been increasing over the past 30 years due in part to an aging population, increased prevalence of obesity and diabetes, improved survival from cardiovascular disease, and an enlarging and aging ethnic minority community (7). In the UK, between 1994 and 1998, prevalence of diabetes in males rose from 2.0% to 2.5% (8) and admissions for angioplasty among diabetics rose 15-fold between 1996 and 2005 (9). These increases may be due in part to increased recognition of type 2 diabetes and increasing willingness to treat these patients for their additional medical problems.
Combining the registry data from the European Renal Association–European Dialysis and Transplantation Association (ERA-EDTA) reports until 1990, data from UK national renal surveys, and then later data from the UK Renal Registry, it is possible to track the rising incidence of treated ESRD, as shown in Figure 1.
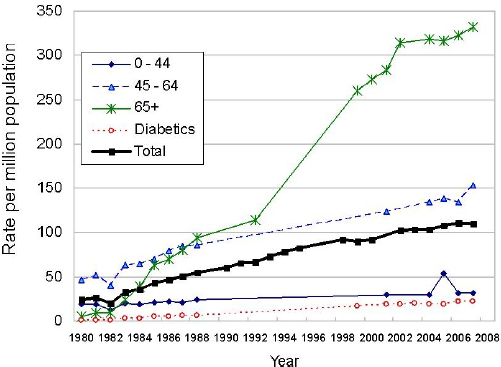
The rate of new patients starting renal replacement therapy each year by age group and diabetes status. Based on data from ERA-EDTA registry (10-17), National Renal Surveys (12), and UK Renal Registry (www.renalreg.com).
In the UK, expansion in the numbers of patients on RRT was hampered partly by funding restrictions. This was an issue that was initially fought against by patient groups (which later became the Kidney Alliance) and some individual clinicians until, in 1984, it became one of the tenets of the Renal Association (3). In 1984 the combined support of these groups resulted in the Minister for Health urging health authorities to spend more on RRT and set a target of 40 new patients per million population (pmp) by 1987 (10). By 1987, the incidence (acceptance) rate had actually risen to 60.2 pmp, although this was still far below European levels and also below the required level of 80 pmp estimated by Feest and colleagues (11).
The 1995 National Renal Survey responses revealed that there were several constraining factors preventing further expansion: 76% of centers had funding issues, 80% lacked physical space, 70% lacked trained nursing staff, and 22% lacked medical staff (12). In the period to 1998 there was little expansion in the number of HD facilities and so these increasing numbers of patients were accommodated by expanding the numbers of patients per renal center, the use of twice weekly HD, and by expanding home dialysis modalities.
International studies have supported the observation that levels of spending on health care are associated with rate of RRT (13). The recent increasing incidence of RRT provision in the UK is due to improved funding and changes in government policy and guidance, in addition to liberalization of physicians’ attitudes to referral for dialysis in light of improving patient survival (14,15). This has resulted in a rising median age of patients starting on RRT and an increased prevalence of dialysis patients with significant comorbidity.
In 1981, the number of new patients commencing RRT in the UK with a diagnosis of diabetes mellitus was 1.2 pmp, or 5% of incident patients. This compared with 25% of incident patients in Scandinavia at this time (16), although that may have been due partly to higher prevalence of type 1 diabetes in some Nordic countries. By 2008, increasing rates of diabetes mellitus and improved survival despite cardiovascular disease had resulted in 24% of incident RRT patients in the UK having diabetes as the cause of their renal disease (17).
Since 1981 the number of patients aged over 65 years commencing RRT has risen from 5.5 pmp (25% of the incident RRT population) to 327 pmp in 2008 (50% of the RRT population) in the UK. The overall number of new patients commencing RRT has stabilized over the past 3 years in the UK, with falling numbers seen in the over 65 years age group. This is possibly due to the increasing recognition that a subgroup of more comorbid patients may not have increased life expectancy with dialysis therapy (18).
Incident rates of RRT are now similar to those seen in many other Northern European countries (UK 109 pmp, Norway 113 pmp, The Netherlands 118 pmp, Finland 92 pmp) although much lower than in the USA (361 pmp) and Greece (190 pmp). It is possible that these differences persist due to a combination of lower incidence of ESRD in the population, persisting “unmet need,” and greater acceptance of the role of conservative non-dialytic treatments for ESRD in the UK.
Regional Variation in RRT Incidence: It was noted early on that patients living near a major renal center, often also a renal transplant center, were more likely to be referred for and commenced on RRT (19). Geographical distance from the renal center was also an independent predictor of poor survival once on RRT (20). These facts led to the development of the National Renal Purchasing Guidelines in 1994 — which were designed to improve equity of access to RRT (21) — and resulted in the provision of satellite HD centers situated in district general hospitals or on stand-alone sites, or, in the case of Wales, the development of commercially provided HD facilities to care for NHS patients (22). In 1993, 20% of HD stations were in satellite units, increasing to 33% by 1995 (23); this percentage continues to rise today. A Health Technology Assessment comparing therapy in satellite HD centers with main centers demonstrated equal patient survival, better achievement of HD dose, reduction in patient travel times, and greater patient satisfaction (24). Regional variation in RRT incidence persists today even after adjusting for the differences in the underlying ethnicity and age structure of the general population. How this variation may be explained is the subject of ongoing work at the UK Renal Registry. There is evidence, however, that rates of referral to nephrology for patients with chronic kidney disease stage 4 or 5 are still only around 15% of the expected rate (Judge A, unpublished observations).
The Changing Popularity of PD (figure 2)
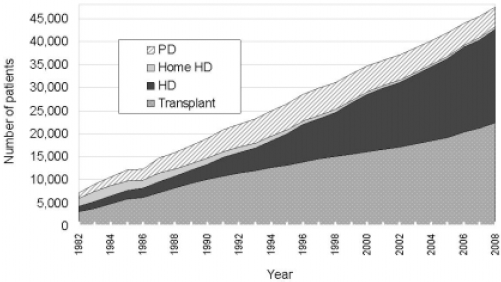
Growth in numbers of prevalent renal replacement therapy (RRT) patients in the UK by modality of RRT at the end of each year from 1982 to 2008. Based on data from ERA-EDTA registry (10-17) and UK Renal Registry (www.renalreg.com), including data from non-reporting centers. PD = peritoneal dialysis; HD = hemodialysis.
Peritoneal dialysis originated as a treatment for acute renal failure and was used from 1946 through to 1975 initially by a urologist in Colchester, acknowledging the aid of a local garage in construction of equipment (25). In 1976, Popovich and Moncrief developed the “novel portable/wearable peritoneal dialysis technique,” which was to become known as CAPD. The first commercial 2-L PD bags became available from Baxter in 1978 and made CAPD possible for chronic renal failure.
In the 1980s, the fall of home HD (HHD) as a percentage of the total dialysis population was due to the increasing numbers of patients commencing RRT on PD. In 1981, PD patients represented 20% (881 patients) of the dialysis population; by 1986 this was 40% (2492 patients) and it reached a peak of 47% in 1992 (5290 patients). The usage of PD has now started to fall as a percentage of the total dialysis population. The number of patients on PD reached a peak of 5920 in 1998 and is now also continuing to fall annually, with 4200 on PD at the end of 2008, accounting for only 17% of the dialysis population.
In 1978, HHD was used by 65% of all the dialysis patients (1881 patients). Its use started to decline as an overall percentage to 61% (2125 patients) by 1981, 45% (1684 patients) by 1986, and 11% (863 patients) by 1995. Use of HHD has continued to decrease each year and now stands at 2.1% (530 patients) of the total dialysis population in 2008.
Transplantation has expanded in line with the increasing RRT numbers. In 1978, 43% (2286) of all RRT patients had a functioning transplant, in 1981 this was 44.9% (3538), and in 1986 this was 49.7% (6139). The number of patients with a functioning transplant continues to increase annually although, as a percentage of the total RRT population, it peaked at 53.8% in 1990 (10160). At the end of 2008 there were 22300 patients with a functioning transplant, or 47% of the RRT population.
The growth in PD during the 1980s to 1990s was due to both funding and space restrictions within the existing dialysis centers (26). The renal unit in Newcastle, for instance, was able to increase its RRT program by 50% when CAPD was introduced (27). The subsequent decline in PD began when increased funding for renal services became available and coincided with the inception of the hub-and-spoke model of HD provision, which reduced patient travel times (28). In 1978 there were only 58 HD facilities, increasing to 154 by 1998 and 279 in 2008. This expansion in the number of HD facilities is temporally related to a decrease in the use of home dialysis therapies (Figure 3).
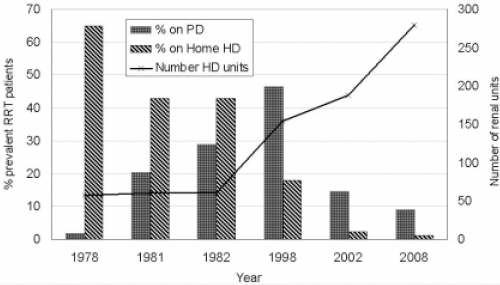
Use of home dialysis therapies over time. Based on data from ERA-EDTA (10-17), Blank et al. (29), and UK Renal Registry (www.renalreg.com). PD = peritoneal dialysis; HD = hemodialysis.
Between-center variation exists in PD usage: 7% of patients in Cambridge commenced RRT on PD in 2008, compared with 55% in Manchester (17). This variation has arisen due to a combination of factors, including physician choice, lack of HD space, and lack of resources to expand HD facilities, which occurs particularly in urban settings (30). Some centers found that the housing in urban socially deprived areas meant limited storage space for PD fluids, precluding its use.
Once there was greater availability of HD stations, the higher rates of “technique failure” that were thought to exist at that time in PD patients compared with HD patients, even after adjustment for pretreatment prognostic factors such as age and presence of comorbidity, may have contributed to the continued decline in PD rates. Analyses at that time showed that, after censoring for death and transplantation, 3-year PD technique survival was 63% (31). A major cause of technique failure was peritonitis, with peritonitis rates of 1 in 14.7 months for CAPD and 1 in 18.1 months for automated PD (APD; p ≤ 0.05) according to an audit study from London from 2002 to 2003 (32), and 1 in 18.6 months for CAPD and 1 in 20.3 months for APD in Scotland from 1999 to 2002 (33). Rates of peritonitis are falling over time: in 1978 peritonitis rates on CAPD were much higher, at 1 in 4.9 to 1 in 7.6 patient–months (34).
Improvements in connection technology helped reduce peritonitis rates, changing from a standard technique of repeated connections between the Tenckhoff catheter and the dialysate bag to using a Y-shaped connector to provide physical separation between the connection and the catheter. A “flush before fill” technique was added to eliminate contaminants before the installation of the next bag of sterile dialysate (35). Seven centers continue to employ the “connect PD” technique for some of their patients, a term coined by the UK Renal Registry to describe what was previously known as “standard CAPD”.
Types of PD: The next advance was continuous cycling PD (CCPD), termed automated PD (APD) by Baxter Healthcare, which was developed in 1981 and performed each night or on several nights per week with or without a daytime fill. This modality leaves the patient relatively free from having to undertake dialysis exchanges during the day and so appeals to those with work or family commitments and also to those patients reliant on a helper to perform their exchanges. Assisted PD is a recent innovation employing a paid trained assistant to help with these exchanges.
In 1997, 33% of the incident RRT population were on CAPD at day 90 and 2% were on CCPD. Since 2000, the numbers treated with CCPD have increased so that, in 2008, 13% of the incident RRT population were on CAPD at 90 days and 7% were on CCPD (Figure 4). In 2008, 10 UK renal centers offered CAPD only and 4 centers CCPD only (36).
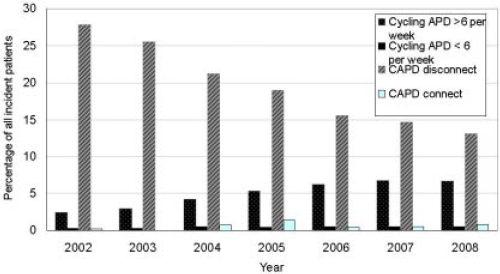
Peritoneal dialysis modalities used by incident patients at day 90 from 2002 to 2008. Based on data from UK Renal Registry (25). APD = automated peritoneal dialysis; CAPD = continuous ambulatory peritoneal dialysis.
The increasing use of CCPD, despite its higher financial cost, has been supported by evidence from the 2007 Cochrane review that CCPD has lower peritonitis rates compared to CAPD [rate ratio 0.54,95% confidence interval (CI) 0.35 – 0.83], lower hospitalization rates (rate ratio 0.60, 95% CI 0.39 – 0.93), and similar survival (relative risk 1.49, 95% CI 0.51 – 4.37) (37). A recent review reiterates these benefits and also finds no clinically significant difference in preservation of residual native renal function (38).
Conclusions
Provision of RRT in the UK has been driven by changing evidence and physician experience as well as by financial factors. Home dialysis therapies dominated the early days of RRT but now are utilized by a smaller proportion of current dialysis patients. Home HD usage has fallen well below targets suggested by NICE, although the evidence basis for these targets is hotly debated (39). Increasing concern about HD line-related septicemia (40) and tightening of the NHS purse over the next 5 years may stimulate regrowth of home dialysis modalities.
Footnotes
The authors do not have any conflict of interests to declare.