
Abstract
Background
Uremic tumoral calcinosis (UTC) has been analyzed in uremic patients on hemodialysis, but little is known about UTC in peritoneal dialysis (PD). In this study, we aimed to characterize UTC in uremic patients on PD.
Methods
We retrospectively reviewed uremic patients on PD who developed UTC over a 9-year period. Clinical, radio-logic, and laboratory features; treatments; and outcomes in those patients were assessed. One of the patients (case 7) is described as a case example.
Results
The study enrolled 7 patients with a mean age of 41 years. Mean time from PD to UTC was 45.3 months. All patients were anuric but adequately dialyzed. Cardinal symptoms were local tenderness and limited range of joint motion. Lesions were mostly multifocal (n = 6) and predominantly involved shoulders, hands, feet, hips, and wrists. Metatarsophalangeal joint UTC was misdiagnosed as tophaceous gout in 2 patients. Main laboratory findings were hyperphosphatemia (7.9 ± 0.8 mg/dL), high CaxP product [>65 mg2/dL2 (range: 81.1 ± 11.5 mg2/dL2)], secondary hyperparathyroidism (SHPT) with various levels of intact parathyroid hormone (iPTH: 592.2 ± 315.2 pg/mL; <250 pg/mL in 2 patients). Medical treatments for UTC included P restriction, non-Ca-based phosphate binders, and adequate dialysis with low-Ca dialysate, but all treatments were ineffective. Parathyroidectomy (n = 3) can partially ameliorate UTC, but only 1 patient (case 7), who had extremely high iPTH (1085 pg/mL), manifested hungry bone syndrome (HBS) and had remarkable resolution of UTC. By contrast, in patients who underwent renal transplantation (n = 3), UTC completely resolved by about 1 year after surgery.
Conclusions
Uremic tumoral calcinosis develops in anuric PD patients with uncontrolled hyperphosphatemia; it is usually multifocal, occurring around the weight-bearing joints or overused smaller joints. Aggressive medical therapy alone is ineffective, and parathyroidectomy appears to be unsatisfactory except in the presence of severe SHPT with postoperative HBS.
The prevalence of UTC ranges from 0.5% to 3% in uremic patients on hemodialysis (HD) (3,4). Medical treatment for UTC includes dietary phosphorus restriction, non-Ca phosphate binder, calcimimetics, optimal control of secondary hyperparathyroidism (SHPT), and intensive HD with low-Ca dialysate. Surgical excision, parathyroidectomy (PTX), and renal transplantation are recommended for persistent or refractory UTC (5,6). Most of the experience with management for UTC has been reported for patients on HD, not for those on peritoneal dialysis (PD). Furthermore, UTC has rarely been reported in PD. Here, we report a typical PD patient who developed UTC, and we analyze the radiologic, laboratory, and clinical features of UTC in patients on PD at our center.
Methods
Case Presentation
A 45-year-old woman (case 7 in Tables 1–3) with end-stage renal disease secondary to immunoglobulin A nephropathy had been on automated PD since December 2007. Her weekly Kt/V was 1.78, and her weekly creatinine clearance, 51.1 L. Her peritoneal membrane transport, based on a dialysate-to-plasma ratio of creatinine of 0.49, was low. Her daily urine output had been about 500 mL at the beginning of PD, but she became anuric in July 2009. She had shown persistent hyperphosphatemia and hypercalcemia and significant SHPT since June 2009 (Figure 1). Non-Ca phosphate binders such as lanthanum carbonate (750 mg 3 times daily) and calcimimetics (cinacalcet 60 mg daily) were added to control her hyperphosphatemia and severe SHPT after withdrawal of Ca carbonate (950 mg 3 times daily) and calcitriol (0.5 μg daily), but all failed. At 3 months before presentation, chest radiographs were relatively normal, without tumoral calcification.
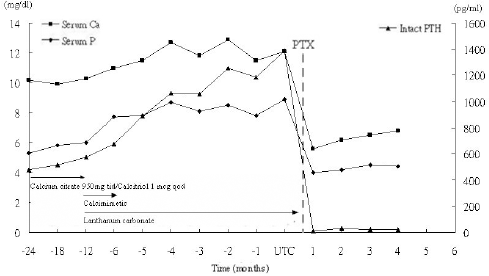
Serial changes of serum Ca, P, and intact parathyroid hormone (PTH) before and after parathyroidectomy (PTX) in the patient. UTC = uremic tumoral calcinosis.
Demographic Characteristics of Peritoneal Dialysis (PD) Patients with Uremic Tumoral Calcinosis
BMI = body mass index; GN = glomerulonephritis; IgA = immunoglobulin A; tid = three times daily; bid = twice daily; tiw = three times weekly; qd = every day; CAPD = continuous ambulatory PD; APD = automated PD; PET = peritoneal equilibration test; D/P Cr: dialysate–to–plasma ratio of creatinine; CCr = creatinine clearance.
Clinical Findings, Therapy, and Evolution in 7 Patients with Uremic Tumoral Calcinosis
B = bilateral; MCP = metacarpophalangeal joint; MTP = metatarsophalangeal joint; IP = interphalangeal joint; Tx = transplantation.
Averaged Biochemistry Findings Within the 6 Months Preceding Uremic Tumoral Calcinosis
PTH = parathyroid hormone; ALP = alkaline phosphatase; BUN = blood urea nitrogen.
In April 2010, this patient began to complain of left shoulder and cervical region tenderness, rigidity, limited range of motion (ROM), and numbness, with a hard palpable mass between neck and scapula. Radiographs showed a well-defined periarticular lobulated calcified mass, without any direct bony invasion, over her left shoulder [Figure 2(A)] and an irregular calcified mass over her right hip joint area. Pertinent laboratory studies revealed high serum levels of Ca (12.9 mg/dL), inorganic P (8.5 mg/dL), alkaline phosphatase (ALP, 491 IU/L), and intact parathyroid hormone (iPTH, 1385 pg/mL). Based on the characteristic radiographic findings and metabolic derangements, UTC associated with tertiary hyperparathyroidism was suspected. A parathyroid nodule about 2.0 cm within the right thyroid gland region was identified. No ectopic parathyroid enlargement was observed on 99Tc–sestamibi scan. Parathyroidectomy was instituted for the intractable SHPT and resultant UTC. After PTX, the patient developed apparent hungry bone syndrome (HBS), manifesting rapid symptomatic hypocalcemia (decline to 5.6 mg/dL from 12.9 mg/dL) and normalization of hyperphosphatemia (decline to 4 mg/dL from 8.7 mg/dL), which was treated with intermittent intravenous Ca supplementation and regular calcitriol 1 μg daily. Serum Ca concentration was kept at approximately 7.0 mg/dL for 4 months. Notably, most of the UTC resolved dramatically in the 3 months after the successful PTX [Figure 2(B)].
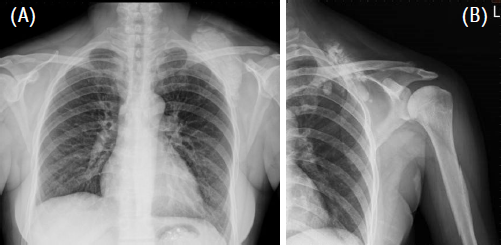
Radiographic changes of a giant uremic tumoral calcinosis in the vicinity of the acromiosternal joint (A) before and (B) 3 months after parathyroidectomy for severe secondary hyperparathyroidism.
Patient Review
We collected data for all patients undergoing continuous ambulatory PD (CAPD) at our single medical center from March 2001 to May 2010 when the integrated medical information system was built. During that period, the cumulative number of CAPD patients was 426 (209 men, 217 women; mean age: 53.9 years), and the total modality drop-out was 271. Diagnosis of UTC was based on characteristic radiographic features: lobulated peri-articular calcifications of more than 2 cm at large joints (elbow, shoulder, hip, knee) or of 1 cm at small joints (hand, wrist, foot). Patients with a diagnosis of calcific uremic arteriopathy (CUA) or calciphylaxis, another syndrome of extraskeletal calcification associated with ischemic cutaneous necrosis, were excluded. Eligible patients with UTC were enrolled for analysis. By reviewing medical records, we analyzed demographic distribution, PD parameters, relevant medications, clinical presentation, laboratory profile, radiologic features, treatments, and outcomes.
Demographic data included age, sex, body mass index, cause of uremia, history of arthritis or trauma, duration of PD, residual renal function, adequacy of dialysis in terms of weekly creatinine clearance and total (peritoneal and kidney) Kt/V, peritoneal transport status according to a standard peritoneal equilibration test, administration of vitamin D3 analogs and various phosphate binders, and the Ca concentration in peritoneal dialysate.
Clinical manifestations included location and size of the UTC; presence of local swelling, tenderness, and ulceration generated by repetitive friction; limited joint ROM; and neurologic symptoms (numbness or paresthesia).
Laboratory data were collected and analyzed based on the averaged serum Ca, P, CaxP product, iPTH, ALP, aluminum, total protein, albumin, and lipid profile within the 6 months before the diagnosis of UTC. Significant SHPT and high CaxP product were defined as iPTH exceeding 400 pg/mL and CaxP exceeding 65 mg2/dL2 respectively (6).
Treatments and their outcomes were assessed. Medical therapy included a P-restricted diet, Ca or non-Ca phosphate binders, and intensive PD with low-Ca dialysate (2 mEq/L). Surgical intervention included local lesion excision, PTX in selected patients with moderate-to-severe SHPT, and renal transplantation. Systemic and lesion outcomes were both incorporated. The former focused on co-occurrence of cardiovascular disease or mortality, and the latter represented changes in the lesions themselves. For the present study, we categorized the local outcome for each UTC lesion as complete remission (complete disappearance of the lesion), partial remission (improvement in symptoms or lesions), or resistance (lack of clinical or anatomic improvement).
Results
Demographic and Dialytic Features
Our study identified 7 patients with UTC [6 women, 1 man; mean age: 41 years (range: 21 – 55 years); Table 1]. Most had lower body mass index (average: 20.85 kg/m2). The causes of uremia were unrelated to the development of UTC. Mean interval from PD initiation to onset of UTC was 45.3 months (range: 17 – 84 months). All patients had lost their residual renal function, becoming anuric (24-h urine < 100 mL), but all were adequately dialyzed (weekly Kt/V > 1.7) before the emergence of UTC. Peritoneal equilibration test revealed 4 patients with high-average transport, 2 with low-average transport, and 1 with low transport. Before study start, all patients had been taking Ca-based phosphate binders; 4 were also taking vitamin D3 analogues at the same time.
Clinical Manifestations
In order of frequency, lesion sites (Table 2) were shoulder (n = 7 in 5 patients), hand (metacarpophalangeal joint, n = 7 in 5 patients), foot (n = 5 in 3 patients), hip (n = 5 in 4 patients), wrist (n = 3 in 2 patients), elbow (n = 2 in 1 patient), and ankle (n = 1). The sizes of the UTC lesions were highly variable. Most patients had multiple lesions (86%, n = 6), except for 1 patient with a solitary lesion where a local contusion had previously occurred. The most common manifestation was tenderness (71%, n = 5), followed by limitation of joint ROM (43%, n = 3) and skin ulceration caused by repetitive friction (43%, n = 3). Neurologic symptoms attributable to intermittent cubital tunnel syndrome was found in 1 of the 7 patients.
Radiographic Picture
As shown in Figure 3, radiographs showed extensive calcifications involving periarticular soft tissues, without bony invasion or joint destruction. Imaging by 99Tc–MDP bone scan showed characteristic multifocal hot spots indicating increased nucleotide uptake over the periarticular soft tissue surrounding the involved joints (Figure 4). Interestingly, until the confirmation by radiography, UTC at the metatarsophalangeal (MTP) joint was, because of its location and the local tenderness, initially misdiagnosed as tophaceous gout in 2 cases.

Radiographs of uremic tumoral calcinosis, showing massive calcification of the periarticular region without direct bony or joint invasion at (A) shoulder, (B) elbow, (C) hands, (D) hip, and (E) foot.

Whole-body bone scan showing periarticular calcinosis with preservation of bony structure.
Laboratory Characteristics
As shown in Table 3, the patients uniformly presented with hyperphosphatemia (range: 7.0 – 8.9 mg/dL; mean: 7.9 mg/dL) and high CaxP (range: 69.3 – 102.7 mg2/dL2; mean: 81.1 mg2/dL2). Hypercalcemia was observed in 3 patients (43%), and significant SHPT with iPTH above 400 pg/mL in 5 patients (71%). Serum ALP was increased in 5 patients (71%). Mean serum albumin in the group was 3.8 g/dL (range: 3.3 – 4.1 g/dL).
Treatments and Outcomes
Medical therapy, including dietary P restriction, low-Ca dialysate, and aggressive use of phosphate binders, either with Ca compounds (n = 7) or non–Ca compounds (lanthanum carbonate, n = 2), were all ineffective. Three patients (cases 1, 2, and 7) underwent PTX. Despite a dramatic fall in serum PTH, a remarkable resolution of UTC, and significant relief of clinical symptoms after PTX, 1 patient (case 7) was found, within 3 months, to have more severe hyperparathyroidism, a much higher ALP level, and development of obvious HBS with hypocalcemia and hypophosphatemia. The other 2 patients, who had had a moderate degree of SHPT, did not develop frank HBS and did not achieve a satisfactory reduction in UTC after PTX. Figure 5 shows the serial changes in serum PTH, Ca, and P before and after PTX in these 3 patients. Successful allograft renal transplantation was eventually completed in 3 patients, including 2 who had previously undergone PTX as already described. Complete resolution of UTC was achieved within the first postoperative year.
Discussion
We characterized UTC in uremic patients on PD over a 9-year period, identifying 7 patients with UTC, 6 of whom were women. All were anuric but adequately dialyzed. Pain and limited ROM caused by the mass effect of UTC were the most common symptoms. Lesions were mostly multifocal, with shoulders, hands, feet, hips, and wrists being the predominant sites. Uncontrolled hyperphosphatemia with varying degrees of SHPT were the universal laboratory finding. Medical control was relatively ineffective in resolving UTC. Remarkable resolution of UTC was achieved with PTX in 1 patient, but with development of HBS; results were unsatisfactory in 2 other patients.
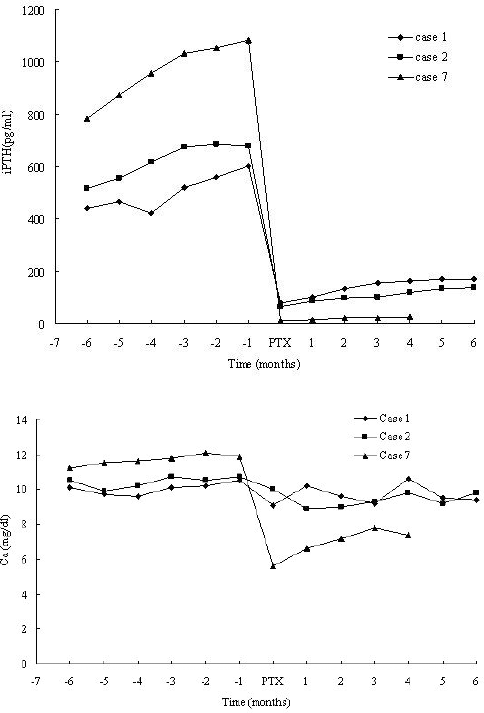
Serial changes in intact parathyroid hormone (iPTH) and Ca levels for 3 patients with uremic tumoral calcinosis and secondary hyperparathyroidism before and after parathyroidectomy (PTX).
Compared with previous reports of UTC in Asian HD patients, the interval from the start of PD to the onset of UTC was shorter (45.3 months vs. 63.3 months on average). Only 43% of the PD patients (3 of 7) had been dialyzed for more than 3 years, which contrasts with 87.5% of patients (7 of 8) dialyzed with HD (3). The average time from dialysis start to the development of UTC was 40.8 months in 6 previously reported PD patients (Table 4), which is similar to the interval in our report (7-12). Multiple factors may be responsible for the shorter time to UTC development in anuric patients on PD, including relatively low clearances of P because of higher peritoneal transport (4 of 7 patients in the present study) and a relatively excessive P intake from the regularly recommended high-protein diet containing approximately 14.6 mg P per gram of protein (13,14).
Previous Cases of Uremic Tumoral Calcinosis in Continuous Ambulatory Peritoneal Dialysis (PD) Patients Reported in the Literature
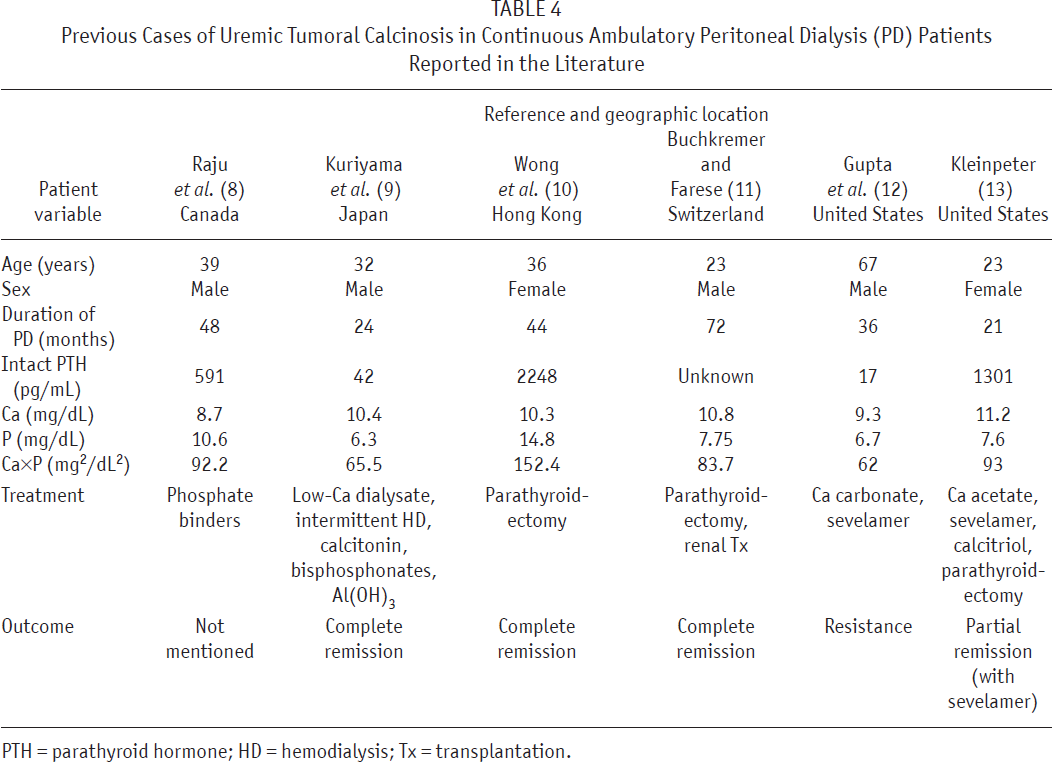
PTH = parathyroid hormone; HD = hemodialysis; Tx = transplantation.
The incidence of UTC in PD patients was estimated to be 1.6% (7 of 426), similar to that in HD patients in a Japanese study (1.9%, 8 of 423). However, a significant proportion of patients on PD may eventually switch to HD for reasons such as technique failure, peritonitis, ultrafiltration failure, or renal transplantation (n = 61 at our center). These patients were still included in the denominator. Patients on PD visit their physicians less frequently than do those on HD. This difference in visit interval may lead to a diagnosis of UTC being delayed until overt symptoms appear. It may be that the true incidence of UTC in PD patients is being underestimated.
The UTC per se rarely induces inflammation or pain. Tenderness is usually attributed to the mass effect of the lesions. Consistent with reports relating to HD patients, UTC in PD patients is mostly multifocal rather than solitary, as in the present study. Lesions are typically observed around the weight-bearing and easily overused joints such as (in order of frequency) shoulders, elbows, and hips (15). Notably, we observed that the first MTP joint, which is not much involved in weight-bearing and is not usually overused during daily activities, was a preferential site of UTC in the female patients of the present study. Local injuries around MTP joints from the wearing of high-heeled shoes by women may be a contributing factor. Moreover, UTC around the MTP joint was misdiagnosed as tophaceous gout in 2 patients until radiography demonstrated radiopaque UTC rather than radiolucent tophi.
Uncontrolled hyperphosphatemia, with high CaxP product, was the most uniform laboratory abnormality in PD patients with UTC. A CaxP product above 60 – 68 mg2/ dL2 is well known to facilitate extraosseous (vascular and visceral) calcification (6). It is reasonable to suggest uncontrolled hyperphosphatemia with a high CaxP product as a “forme fruste” for the development of UTC. Other systemic predisposing factors for UTC such as severe SHPT, hypoparathyroidism, and adynamic bone disorders, aluminum intoxication, excessive use of Ca-based phosphate binders or of active vitamin D (or both), and alkalosis have been proposed, but significant SHPT was the only symptom found in 5 of our 7 patients. Significant SHPT with iPTH exceeding 400 pg/mL tends to mobilize skeletal Ca and phosphate into circulation, theoretically facilitating extraosseous calcification and UTC formation (3,6,16–19). Meanwhile, local factors such as articular or periarticular trauma, hematoma, inflammation, abnormal pH, transforming growth factor β expression, or de novo overproduction of calcifiable matrix proteins can be a potential “second hit” stimulus to foster the formation of UTC in the milieu of background hyperphosphatemia and higher CaxP product (20-23). In the present study, 1 patient (case 3) developed UTC adjacent to the hip joint several months after a traffic trauma.
In HD patients, medical therapy, including non-Ca phosphate binders to reduce Ca and phosphate reabsorption, modification of HD with longer session durations, increased frequency, and the use of low-Ca dialysate to enhance Ca and phosphate clearance, can mobilize the Ca deposits of UTC (24-26). Response to medical therapy in our patients was quite variable, but appeared to improve over time. However, the effect on UTC was unsatisfactory even with aggressive use of non-Ca phosphate binders, calcimimetics, low-Ca dialysate, and increased dialysis doses in our PD patients. Aggressive medical measures combined with intermittent HD has been reported to achieve complete resolution of UTC in a PD patient (8). The reasons for the equivocal response of UTC to medical control in PD patients remains unclear. Perhaps the timing and duration of intensive medical control and the different underlying mechanisms of UTC may be related.
Surgical intervention—including resection of focal lesions, PTX, and renal transplantation—has been suggested for symptomatic UTC. Surgical excision of UTC performed in 1 patient achieved immediate relief of nerve compression and joint limitation, with cosmetic improvement, but that approach was unhelpful for UTC elsewhere. The efficacy of PTX—meant to attenuate PTH-mediated skeletal Ca and P efflux into circulation and soft tissues—remains controversial in the treatment of UTC. To the best of our knowledge, Wong et al. (10) reported the only case of UTC in CAPD successfully eradicated by PTX (Table 4). In the present study, 3 patients (cases 1, 2, and 7) underwent PTX because of co-existing UTC and SHPT. Although a dramatic fall in serum PTH was observed in all cases of successful PTX, a remarkable dissolution of radiologic UTC and resolution of clinical symptoms was found in only 1 patient who had much higher serum ALP activity preoperatively and who developed overt HBS postoperatively. The other 2 patients, who did not exhibit a marked increase in serum ALP preoperatively and who did not develop frank HBS postoperatively, achieved unsatisfactory reduction in UTC after PTX. Although HBS is not universal after PTX, its development depends on the severity of SHPT and the presence of extraskeletal calcification. After PTX, UTC may act as a reservoir for Ca and P mobilization and re-mineralization of bone. Once the Ca and P required for bone formation are resorbed, the size of UTC lesions may perhaps not be further reduced. However, if SHPT is more severe, then post-PTX HBS would be able to drive bone formation even in the presence of the protective effect of UTC. Serum ALP is a good predictor for the severity of HBS in dialysis patients undergoing PTX (27), which seems to provide a plausible explanation for a much higher serum ALP and the development of frank HBS after PTX resulted in a rapid dissolution of UTC. Nevertheless, only successful renal transplantation can achieve complete resolution of UTC within 1 year, as shown in our 3 patients who received grafts, including the 2 who underwent PTX without developing HBS.
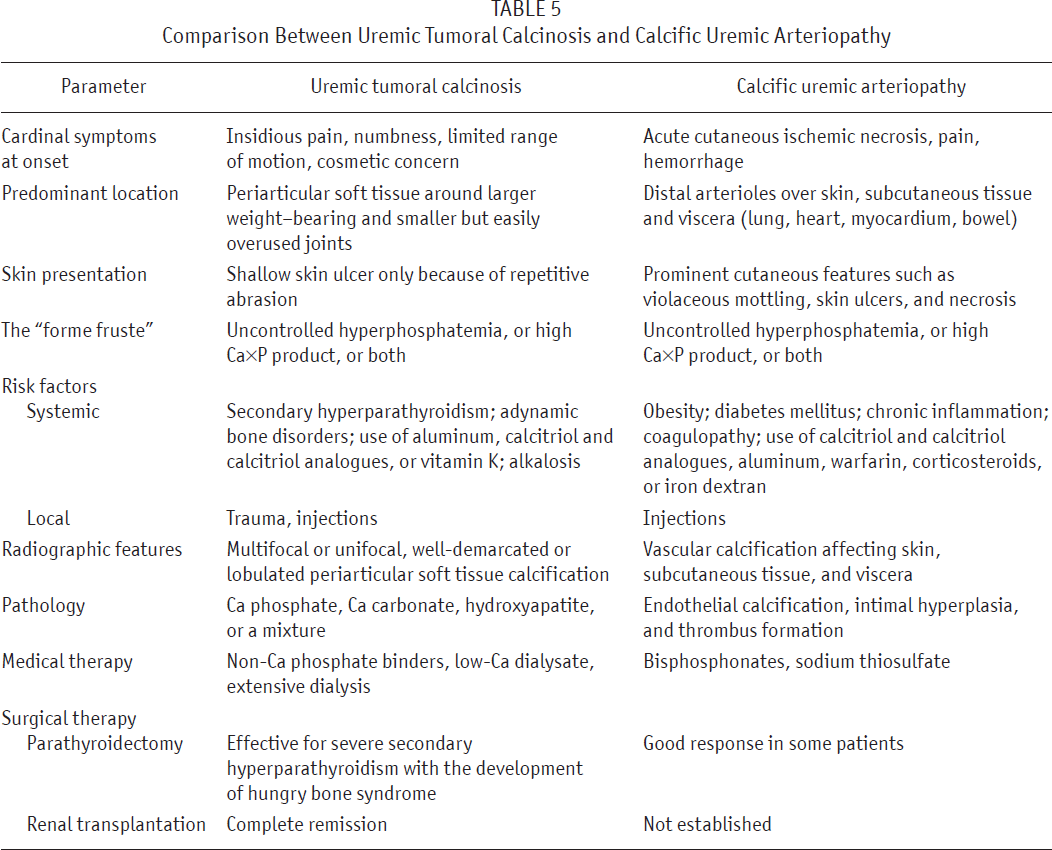
In dialysis patients, extraskeletal metastatic calcification can manifest as UTC in soft tissue of the periarticular region or as CUA, in which thrombosis in calcified small arteries or arterioles leads to infarction and infection of the affected tissues. Although UTC and CUA present similar laboratory pictures, with hyperphosphatemia, high CaxP product, and an increased incidence with time on dialysis, their clinical features, pathology findings, risk factors, and therapeutic options are distinctively different. Table 5 compares UTC and CUA.
Comparison Between Uremic Tumoral Calcinosis and Calcific Uremic Arteriopathy
Conclusions
In anuric PD patients, UTC development is signaled by laboratory findings of uncontrolled hyperphosphatemia with higher CaxP product. The condition is usually multi-focal, occurring around the weight-bearing joints or easily overused smaller joints. Aggressive medical therapy is relatively limited in its effect. Remarkable resolution of UTC is seen with PTX in patients who later develop HBS, but is usually unsatisfactory in other patients. Early and tight control of serum P in the normal range is likely to prevent the development of metastatic calcification in dialysis patients.
Footnotes
The authors have no potential conflicts of interest or financial sponsors to declare.