
Abstract
Laparoscopy is an effective method of implantation for peritoneal dialysis (PD) catheters. Use of the laparoscopic technique is increasing because of its potential advantages over other techniques. In most patients, selection for PD is based on negative criteria, and because of the need for general anesthesia, the laparoscopic technique can be life-threatening in these patients. On the other hand, local anesthesia is insufficient for laparoscopic catheter implantation. To avoid the need for general anesthesia and to achieve patient safety and satisfaction, we designed a type of conscious sedation (dissociative conscious sedation) and compared the efficacy of subcutaneous (SC) and intravenous (IV) ketamine added to narcotics in patients scheduled for laparoscopic implantation of a PD catheter.
Methods
Our prospective randomized double-blind study enrolled 60 adult patients with chronic renal failure who were scheduled for laparoscopic implantation of a PD catheter. Patients were randomly assigned to one of two groups: one receiving IV ketamine, and the other receiving SC ketamine. In both groups, patients were premedicated with IV midazolam 0.015 mg/kg, fentanyl 1–2 μg/kg, and lidocaine 1.5 mg/kg. Patients then received 0.6 mg/kg ketamine either intravenously (IV group) or by subcutaneous injection at the anterior aspect of the forearm (SC group). If systolic blood pressure (BP) increased more than 20% from baseline or exceeded 170 mmHg, IV nitroglycerine (TNG) 50 μg was administered incrementally (repeated 50-μg doses). After a desirable level of conscious sedation was achieved, local anesthesia and nitrous oxide pneumoperitoneum were applied, and the PD catheter was implanted under laparoscopic guidance. Heart rate and BP were measured throughout the procedure. Adverse effects and recovery events were recorded.
Results
All patients tolerated the procedure well. Administration of TNG was significantly more frequent in the IV ketamine group. Pain intensity during the surgery was similar in both groups. Both groups were comparable with regard to heart rate, but patients in the SC ketamine group had a significantly lower systolic BP at the 2nd measurement and a lower rate–pressure product at the 2nd, 4th, and 5th measurements. All patients in the SC ketamine group were cooperative during surgery and experienced uneventful recoveries; mild hallucinations were observed in 5 patients in the IV ketamine group. In the IV ketamine group, 3 patients lost the ability to cooperate during surgery. All catheters were successfully placed.
Conclusions
Dissociative conscious sedation is an acceptable alternative to general anesthesia in laparoscopic implantation of the PD catheter. Ketamine by the SC route is as effective as, but safer than, IV ketamine.
Keywords
One of the major drawbacks to the acceptance of laparoscopy is the necessity for general anesthesia, because insufflation of gas into the abdominal cavity produces peritoneal pain. Given that candidates for PD catheter implantation are patients with end-stage renal failure who have severe coexisting medical problems that put them in a high-risk category for general anesthesia, laparoscopic implantation of the PD catheter under local anesthesia is becoming more and more popular (4).
Peritoneal insufflation with N2O produces neither peritoneal irritation nor the metabolic effects of insufflation with CO2, including hypercarbia, acidosis, and cardiac arrhythmias (5-8). However, our previous study (9) showed that using N2O does not eliminate the need for appropriate sedation during the procedure, indicating that gas insufflation is the major source of pain in laparoscopic procedures. In 2006, MJJ designed dissociative conscious sedation to overcome this insufflation-related pain and to keep patients relaxed and conscious during the procedure.
In many centers, catheters are routinely placed by the fluoroscopic approach [although the efficacy of this method is not well characterized (10)] or by using a peritoneoscope or open dissection under local anesthesia. Various methods of sedation and anesthesia have been described for catheter placement (11). Ketamine is an N-methyl-d-aspartate receptor antagonist with opioid receptor activity (12). This parenteral anesthetic agent has a documented analgesic effect at sub-anesthetic doses. Multiple studies have used continuous subcutaneous injection of ketamine for cancer pain (12-14), post-herpetic neuralgia (15), postoperative analgesia (16-18), and analgesia for acute musculoskeletal trauma (19). However, the use of single-dose subcutaneous (SC) ketamine in conjunction with intravenous narcotics for the induction of dissociative conscious sedation in laparoscopic procedures has not previously been reported. “Dissociative conscious sedation” is defined as the use of intravenous (IV) or SC infusion of low-dose ketamine in conjunction with narcotics to achieve an acceptable level of sedation, pain relief, and amnesia. This method was designed and used for the first time in a previous study by our group (9), but the present report is the first to describe this anesthesia method in detail.
In the present study, we evaluated the efficacy of SC as compared with IV ketamine dissociative conscious sedation. With both routes of ketamine administration, fentanyl was used as the associated opioid.
Patients and Methods
Our prospective randomized double-blind study enrolled 60 adult patients with chronic renal failure. Approval for the study was obtained from the ethics committee of Tehran University of Medical Sciences, and all patients provided written informed consent. The randomization was based on random permuted block. To reach a statistical power of 80%, each group included 30 patients. Neither the supervising anesthesiologist nor the surgeon knew the route of injection for the ketamine; the drugs were administered by a separate anesthesiologist. The primary endpoints of the study were the severity of intraoperative pain and the surgeon's satisfaction with working space and surgical view.
All patients were scheduled for laparoscopic implantation of a PD catheter. Case selection for PD was based on negative criteria (vascular access problems, severe cardiovascular disease), and therefore all study patients were in poor condition, with severe fluid and electrolyte imbalances, making general anesthesia unsuitable, and possibly life-threatening, for them. Patients with a history of psychological disorders, coronary artery disease, uncontrolled hypertension, increased intracranial pressure, intracranial mass lesions, or an open eye injury or other ophthalmologic disorder were excluded from the study.
Anesthesia Technique
All procedures were performed in the operating room. Patients were continuously monitored using standard techniques including electrocardiography, pulse oximetry, and noninvasive sphygmomanometry. All patients were premedicated with IV midazolam 0.015 mg/kg, fentanyl 1–2 μg/kg, and lidocaine 1.5 mg/kg (to prevent cardiac dysrhythmia). Patients were then randomly assigned to receive 0.6 mg/kg ketamine either IV (IV group) or by SC infusion at the anterior aspect of the forearm (SC group).
If systolic blood pressure (BP) increased more than 20% from baseline or exceeded 170 mmHg (or both), IV nitroglycerine (TNG) 50 μg was given in incremental doses (repeated 50-μg doses) until systolic BP reached 140 mmHg. Oxygen 4 L/min was administered by face mask while the patients were breathing spontaneously. Additional IV fentanyl (50 μg) was administered during the surgery if needed to improve the patient's comfort and pain relief.
After 8 – 10 minutes, or when a desirable level of conscious sedation had been achieved, the surgery was started. “Desirable level” was defined as a level that still permitted the sedated patient to respond appropriately to verbal commands. The main aim of this sedation method is to maintain spontaneous ventilation and to elicit sufficient patient cooperation to tense the abdominal musculature, facilitating insertion of the pneumoperitoneum needle and the port cannulae.
Surgical Technique
The surgical technique for laparoscopic PD catheter implantation was detailed in our previous report (9). Briefly, trocar insertion is facilitated by asking the patient to push out and tense the abdominal wall when required. Local anesthesia is achieved by infiltrating the soft tissue with lidocaine HCL 1%. Peritoneal N2O insufflation pressure is limited to a maximum of 12 mmHg. Two laparoscopic ports are used for catheter implantation: a 5-mm disposable trocar to permit insertion of the laparoscopic camera, and a traditional Tenckhoff trocar device (TR-400: Medionics International, Markham, ON, Canada). A 5-mm skin incision is made 2 cm below the left costal margin at the anterior axillary line. The catheter is then placed. After completion of the surgery, patients are transported first to the post-anesthesia care unit and then to the ward. All patients receive metoclopramide 10 mg at the end of the surgery.
For the present study, we measured each patient's O2 saturation, heart rate, systolic BP, and rate–pressure product at baseline (T1), before skin infiltration (T2), after insertion of the 1st and 2nd trocars (T3, T4), and at the end of surgery (T5). To evaluate arterial CO2 (paCO2), an arterial blood gases analysis was performed about 30 minutes after the start of sedation. Facial expressions and other signs of pain sensation by the patients were recorded throughout the surgery. Post surgery, we asked the patients if they had any recall of events or pain during the procedure. The surgeon's satisfaction regarding the surgical exposure was also assessed at the end of the procedure. Any adverse effects of the present method of conscious sedation—defined as apnea, hypoxemia (O2 saturation < 93%), hypoventilation (paCO2 > 45 mmHg), laryngospasm, or upper airway obstruction—were recorded. We defined “serious adverse events” as the need for positive pressure ventilation, insertion of an oral or nasal airway, or endotracheal intubation, and “minor adverse events” as respiratory events requiring minimal intervention (stimulation, supplemental O2, head repositioning) (20).
Statistics
Data are expressed as mean ± standard deviation or as number of patients. Parametric data were analyzed using the independent samples t-test. For categorical data analysis, the chi-square or Fisher exact test was used. Statistical calculations were performed using the SPSS software application (version 14.0: SPSS, Chicago, IL, U.S.A.). Differences were considered significant at p < 0.05.
Results
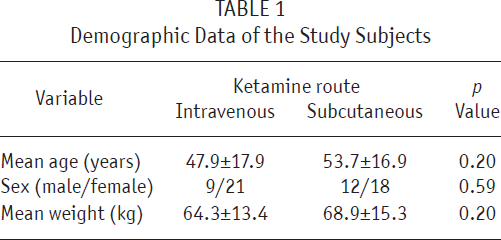
No patient was excluded from the study. Mean age in the study group was 50.67 ± 17.52 years, and 35% of the patients were men. We observed no significant demographic differences between the study groups (Table 1).
Demographic Data of the Study Subjects
As Table 2 shows, TNG administration was significantly more frequent in the IV ketamine group. Pain intensity during the surgery was similar in both groups, as was patient recall both for the surgical events and for pain. Heart rate was also comparable between the groups (Figure 1); however, patients in the SC ketamine group had a significantly lower systolic BP at T2 and a lower rate–pressure product at T2, T4, and T5 (Figures 2 and 3). The average paCO2 was significantly lower in the IV ketamine group. Surgeon satisfaction was similar in both groups (Table 2).
Clinical Data of the Study Subjects
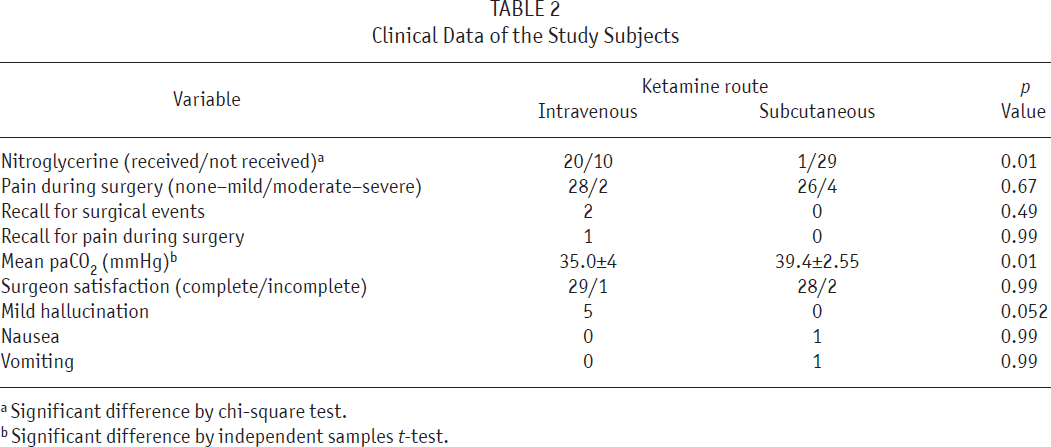
Significant difference by chi-square test.
Significant difference by independent samples t-test.
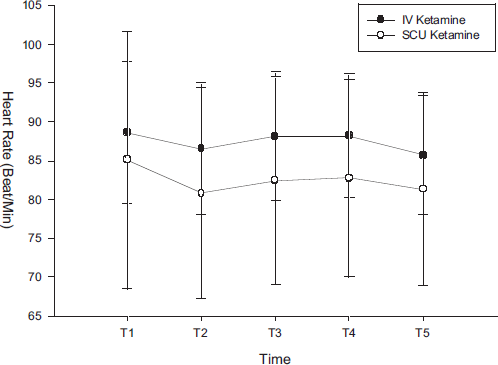
Changes in heart rate at various times during the surgery.
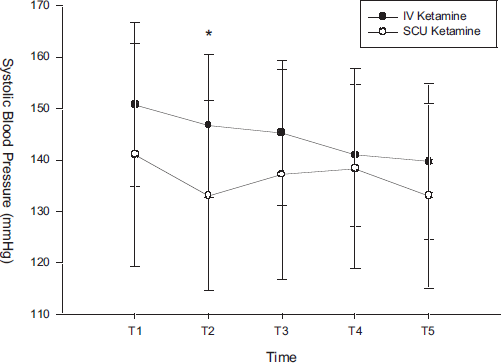
Changes in systolic blood pressure at various times during the surgery.

Changes in rate–pressure product at various times during the surgery.
All patients in the SC ketamine group experienced uneventful recoveries without psychological adverse effects including emergence reactions, hallucinations, feelings of malaise, delirium, and salivation. Mild hallucinations were observed in 5 patients in the IV ketamine group. In the IV ketamine group, 3 patients lost their ability to cooperate, but all patients in the SC ketamine group retained the ability to cooperate. In both groups, all catheters were successfully planted. Mean operative time in the IV ketamine group was 30.2 minutes (range: 20 – 45 minutes); it was 28.3 minutes (range: 20 – 40 minutes) in the SC ketamine group.
Discussion
The present study shows that dissociative conscious sedation (use of IV or SC infusion of low-dose ketamine in conjunction with narcotics to achieve an acceptable level of sedation, pain relief, and amnesia) is an effective method in patients undergoing PD catheter implantation. Patients remain cooperative, but are sufficiently sedated and pain-free. More specifically, the study shows that SC administration of ketamine for induction of conscious sedation is accompanied by a significantly lower rise in systolic BP and rate– pressure product before skin infiltration, after insertion of the 2nd trocar, and at the end of surgery. At the same time, no changes in pain intensity, recall rate during the surgery, and surgeon satisfaction are observed.
Although N2O has an analgesic effect and is not irritating, our experiences during a previous study (9)—a large series of this form of laparoscopy—showed that neither local anesthesia by itself, nor a combination of local anesthesia and ordinary methods of sedation, is sufficient to induce an acceptable level of pain relief. By contrast, Lipscomb et al. (21) found no difference in intraoperative and postoperative pain between N2O and CO2 pneumoperitoneum for laparoscopic sterilization. It therefore seems that gas insufflation is the major source of pain in laparoscopic procedures.
Palter and Olive (22) found two kind of insufflation-related pain. The first was described as an immediate sharp burning sensation with the onset of insufflation (which did not interfere with success of the procedure). The second was described as a crampy dull pain or a feeling of fullness that was relieved by lowering the intra-abdominal pressure to less than 10 mmHg and the CO2 volume to less than 1 L. This second type of pain interfered with the success of the procedure because it led to intolerable pain.
Considering the high volume of insufflating gas (4 – 6 L/min) required to produce an intra-abdominal pressure of 10 – 15 mmHg for an appropriate laparoscopic view (23), the process can be painful enough to interfere with the success of the procedure. Dissociative conscious sedation was therefore designed to provide an optimum situation for the patient, the surgeon, and the anesthesiologist. We used ketamine as an adjuvant to narcotics in our study. Ketamine by the IV route has been used as a sedative in the case of painful blocks (24) and, more commonly, for sedation or supplemental anesthesia during long or uncomfortable procedures. In most studies that used ketamine to supplement regional anesthesia, IV ketamine 0.5 mg/kg has been used (25).
Subcutaneous or transcutaneous infiltration of ketamine is one of several ways to administer ketamine (26). In the present study, we used ketamine because of its known advantages, and SC infusion was chosen to attenuate the drug's adverse effects.
Ketamine by the SC route has several advantages as compared with IV ketamine. First, the gradual absorption of SC ketamine produces a lower level of serum ketamine, which considerably attenuates the side effects. It has been shown that psychomimetic side effects can be prevented by keeping the plasma concentration of ketamine at or below 150 ng/mL (27). Psychomimetic side effects have not been reported after rectal ketamine administration, which is known to result in low plasma levels (28). Subcutaneous infusion might therefore provide analgesia without hallucinations or other psychomimetic effects (12,16). Our results are consistent with the foregoing findings. We observed no psychological adverse effects in the SC ketamine group, and this route of administration, using a sub-anesthetic dose of ketamine, has the advantage of a lower risk of side effects while still controlling pain (29). Very low doses of ketamine have been shown to produce analgesia in the region of both the spinal and the cranial nerves while maintaining alert consciousness (13). Our results show that comparable levels of (sufficient) pain relief and amnesia were achieved in both the SC and the IV ketamine groups, with the patients remaining conscious and cooperative.
Ketamine is also known to have major cardiovascular side effects. It has been shown that, in some patients, ketamine may temporarily increase heart rate and BP by increasing sympathetic nervous system activity (30)—although the effect may be less common in severely ill patients (31). It has also been observed that the cardiovascular effects of ketamine occur to a lesser degree, but are more protracted, with intramuscular as compared with IV administration (32). Caution has therefore been advised in patients with cardiac disease (30). Because of the case selection method in this present study (negative criteria), ketamine was administered in patients with a poor general condition because of vascular access problems and severe cardiovascular disease. These patients had severe fluid and electrolyte imbalances that could result in serious complications with the use of other anesthetic drugs, and there is some evidence that, because of its combined sedative and analgesic properties and its favorable effects on hemodynamics, ketamine has been considered for sedation of heart attack patients in a critical care unit (33). By contrast, the cardiac complications of uremic patients—which include volume overload, congestive heart failure, pulmonary edema, pericarditis, and (in rare cases) pericardial tamponade—are typically accompanied by low cardiac output. During anesthesia, the most important way to prevent decreased cardiac output is to maintain spontaneous ventilation (34). By using low-dose ketamine to maintain spontaneous ventilation during dissociative conscious sedation, greater cardiac output and greater patient safety are maintained. Our results showed that the patients in the SC ketamine group had a significantly lower systolic BP at T2 and a lower rate–pressure product at T2, T4, and T5. A lower plasma level can be assumed to be accompanied by fewer rises in systolic BP and rate–pressure product. In fact, the predominant characteristics of dissociative conscious sedation by SC ketamine are maintenance of hemodynamic stability, spontaneous ventilation, and the patient's conscious cooperation.
Nausea and vomiting are among the most common side effects with laparoscopic procedures, especially in uremic patients, and so we administered metoclopramide to all study patients.
Conclusions
Dissociative conscious sedation is an acceptable alternative to general anesthesia for laparoscopic implantation of the PD catheter, and SC ketamine is as effective as, but safer than, IV ketamine.