
Abstract

Comparison of the Larger Published Studies of Enterococcal Peritonitis
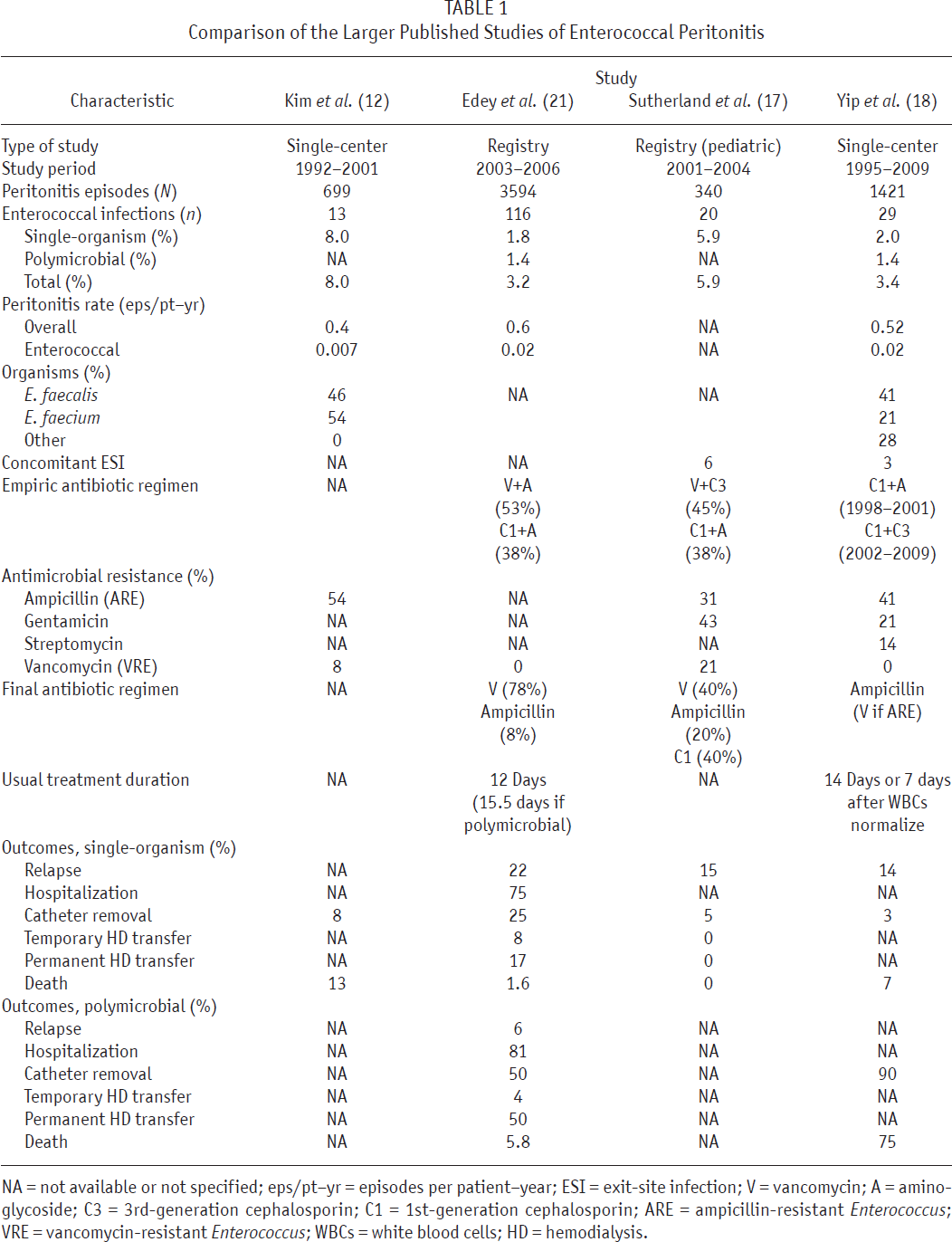
NA = not available or not specified; eps/pt–yr = episodes per patient–year; ESI = exit-site infection; V = vancomycin; A = amino-glycoside; C3 = 3rd-generation cephalosporin; C1 = 1st-generation cephalosporin; ARE = ampicillin-resistant Enterococcus; VRE = vancomycin-resistant Enterococcus; WBCs = white blood cells; HD = hemodialysis.
Several investigations in the 1990s (13,14) and early 2000s (12) reported that enterococcal peritonitis was an infrequent cause of PD peritonitis (up to 8% of all cases) and that it was associated with older patient age, poorer response to empiric antibiotics (including ampicillin), higher rates of hospitalization, higher rates of relapse and repeat peritonitis, and higher rates of death than were seen with gram-positive infections. Absolute rates of enterococcal peritonitis were not reported, except by Kim et al. (12), who observed an enterococcal peritonitis rate of 0.007 episodes per patient–year (Table 1).
In 2010, Edey et al. (15) reported an analysis of peritonitis as recorded in the Australian and New Zealand Dialysis and Transplant (ANZDATA) Registry database between October 2003 and December 2006 (Table 1). In their study, enterococcal infection accounted for 3.2% of all cases of peritonitis, with an absolute rate of 0.02 episodes per patient–year and a single-organism rate of 0.01 episodes per patient–year. The key findings were that, although enterococcal peritonitis tended to be associated with older age, there were no demographic or clinical characteristics that reliably predicted the isolation of enterococci from dialysate. Moreover, nearly half of all cases of enterococcal peritonitis (45%) were associated with the isolation of other organisms. Only 8% of cases were treated with intraperitoneal ampicillin in line with the 2005 and 2010 recommendations from the International Society for Peritoneal Dialysis (1,16), but 78% were treated with vancomycin monotherapy despite concerns regarding the possible emergence of vancomycin-resistant enterococci (VRE). Pure enterococcal peritonitis had outcomes similar to those in non-enterococcal or Staphylococcus aureus infections, but the isolation of additional organisms was associated with a fall in the antibiotic cure rate to 40% from 59%. Importantly, timely removal of the PD catheter (within 1 week of the onset of refractory enterococcal peritonitis) was associated with a significant reduction (to 74% from 100%) in the risk of permanent transfer to hemodialysis. A major limitation of this group's investigation was the lack of available data pertaining to the antimicrobial susceptibilities of the enterococci isolated.
That limitation was recently addressed in children by Sutherland et al. (17), who reported on the clinical characteristics, treatment, antimicrobial susceptibilities, and outcomes of 20 cases of enterococcal peritonitis recorded in the International Pediatric Peritonitis Registry (Table 1). In that series, enterococcal peritonitis accounted for 5.9% of peritonitis episodes. All 20 patients developed peritonitis despite the use of prophylactic antibiotic therapy at the exit site, and Enterococcus was isolated from skin in 1 patient. Resistance to ampicillin, first-generation cephalosporins, third-generation cephalosporins, gentamicin, and vancomycin was observed in 31%, 95%, 85%, 43%, and 21% of episodes respectively. However, despite the high level of resistance to cephalosporins and not-insignificant resistance to vancomycin in vitro, patients who had received empiric treatment with those antibiotics did very well, and overall, outcomes were excellent. Only 1 catheter had to be removed, all patients remained on PD, and all experienced a fully functional recovery. Those results stood in stark contrast to gram-negative peritonitis episodes, in which the in vitro susceptibility to antibiotics closely matched the clinical picture.
In this issue of Peritoneal Dialysis International, Yip et al. (18) present a retrospective, single-center study focusing on the clinical course and outcomes of 29 cases of enterococcal peritonitis in 23 PD patients (Table 1). In keeping with the results of previous studies, they found that enterococci accounted for 3.4% of all peritonitis episodes, were associated with isolation of additional micro-organisms in 41% of cases, and occurred at an absolute rate of 0.02 episodes per patient–year and at a single-organism rate of 0.01 episodes per patient–year. Their findings are virtually identical to those observed in the ANZDATA study (15).
Importantly, Yip et al. noted a significant rise in the rate of single-organism enterococcal peritonitis over the course of the study, to 0.01 episodes per patient–year in 2000 – 2004 and to 0.016 episodes per patient–year in 2005 – 2009 from 0.007 episodes per patient–year in 1995 – 1999. Equally worryingly, these authors found that ampicillin-resistant enterococci (ARE) accounted for 41% of all enterococcal isolates. All E. faecalis isolates were susceptible to ampicillin, and all E. faecium isolates were resistant. Recent use of antibiotics was a strong independent predictor of ARE peritonitis (odds ratio: 12.5).
Overall, outcomes in enterococcal peritonitis were similar to those in coagulase-negative staphylococcal peritonitis and better than those in Escherichia coli peritonitis. The catheter removal rate was very low (3%), although that finding may have reflected a tendency in Hong Kong to transfer PD patients to hemodialysis only as a last resort (19). However, the low catheter removal rate, prioritizing PD technique survival, may have come at the cost of a higher peritonitis death rate, which was 7% overall and as high as 75% in patients with polymicrobial enterococcal peritonitis. The authors did not further analyze the 20 cases of polymicrobial infections, which would have been an interesting extension to their study given the very different outlook reported for polymicrobial enterococcal infections by Edey et al. (15).
As in other studies, Yip and colleagues did not report the frequency and type of underlying intra-abdominal pathology. Peritonitis with ARE was associated with a primary response rate (83%) that was not significantly different from that for peritonitis caused by ampicillin-sensitive enterococci (94%), although ARE patients did receive a longer course of vancomycin. The authors did not observe any VRE episodes, but as the authors note, increasing rates of VRE commonly follow the appearance of ARE in the clinical environment (20).
What can we learn from these results so far?
First, in the general PD population, be they children, adults, Asians, Europeans, or North Americans, the reported incidences of enterococcal peritonitis seem to be quite similar: approximately 0.01 – 0.02 episodes per patient–year. More importantly, these incidences appear to be rising over time as are the frequencies of antibiotic resistance. Enterococci show a marked propensity toward the development of antimicrobial resistance, such that a large preponderance of isolates are now resistant to cephalosporins, and between 30% and 50% are resistant to ampicillin. Reassuringly, however, neither the in vitro resistance pattern nor the choice of empiric antibiotic regimen appears to affect short- or long-term clinical outcomes, which are comparable to those in gram-positive peritonitis and superior to those in other forms of gram-negative peritonitis.
Enterococcal peritonitis may be more common with older age, but there are no reliable clinical predictors of this complication when patients present with symptoms of peritonitis. The main predictor of clinical outcome is the isolation of additional organisms, which occurs in approximately half of all cases and is associated with very high rates of hospitalization, catheter removal, permanent transfer to hemodialysis, and death. Timely catheter removal also appears to have a significant impact on outcomes in enterococcal peritonitis. In particular, published series appear to demonstrate an inverse ratio between the rates of catheter removal and of mortality (Table 1), and one study (15) demonstrated that PD catheter removal within the first week of refractory enterococcal peritonitis is associated with a significantly higher likelihood of subsequent resumption of PD.
The 2010 update of the guidelines for PD-related infections from the International Society for Peritoneal Dialysis (1) recommend that a diagnosis of enterococcal peritonitis should warrant consideration of intra-abdominal pathology, that antimicrobial resistance should be monitored, and that susceptible organisms are best treated with intraperitoneal ampicillin. Episodes of ARE should be treated with vancomycin, and episodes of VRE should warrant consideration of therapy with linezolid or quinupristin–dalfopristin. Antibiotic therapy should be continued for 21 days, and timely catheter removal for refractory enterococcal peritonitis is likely to improve outcomes. The findings of Yip et al. (18) lend further support to those recommendations, although it should be emphasized that their study involved only a small sample of enterococcal episodes from a single center. Even if their findings are replicated in multicenter studies from other parts of the world, a number of important clinical questions remain unanswered, particularly with respect to the value of screening for intra-abdominal pathology in documented cases of enterococcal peritonitis and to the effectiveness of proposed strategies to prevent peritonitis caused by intestinal flora (such as laxative therapy for constipation and correction of hypokalemia). Those issues will be addressed only by improved collaborative research in the PD community and the fostering of multicenter and preferably multi-country peritonitis registries and clinical trial networks.
Footnotes
The authors have no financial conflicts of interest to declare.