
Abstract
Background
Training patients to perform peritoneal dialysis (PD) at home is key to good patient outcomes. Currently, no validated curriculum based on education concepts is available in the public domain, and training is not standardized. Few nurses are prepared to be effective trainers. The present study was designed to evaluate the efficiency and effectiveness of PD training using a new cycler designed with animation, visual images, and voice cues and provided by a qualified PD nurse with a standardized script to guide the trainer.
Methods
The study recruited 40 participants, including individuals naive to dialysis and current automated PD (APD) patients. Participants with visual, hearing, or touch impairments were purposely included to reflect the disabilities common to the general APD population. The participants encompassed a range of self-reported computer and technical experience and education levels. Experienced training nurses trained each participant, one on one, for 4 – 8 hours during a single day; the nurses followed the standardized script as the participants progressed through the cycler training curriculum. The pace of training was adjusted to meet individual abilities and needs. Participants were evaluated by the training nurse at the end of the training session for their proficiency in meeting the learning objectives.
Results
All 40 participants completed the 1-day training and successfully met all task objectives by the end of the day. Participant ages ranged from 23 to 73 years (mean: 53.8 ± 11 years), with the women (50 ± 12 years) being significantly younger than the men (57 ± 9 years, p = 0.05). Among the participants, 90% had visual impairments; 40%, hearing impairments; and 45%, touch impairments. Twenty-nine participants (73%) had multiple impairments. Median training time was 7 ± 0.13 hours, with a range of 5 – 8.25 hours. We found no correlation between the number of hours needed for successful training and age (r = 0.30). Training time did not differ significantly by sex, disability, computer or technical experience, or education level. The required training time was less for participants with previous PD experience (6.5 ± 0.7 hours) than for those naive to dialysis (7 ± 0.8 h), but at p = 0.056, the difference just missed being statistically significant.
Conclusions
The most striking finding is that, despite a variety of barriers to learning, all 40 participants were able to meet all the stated objectives of the study with 4 – 8 hours of training. Ability to meet the study objectives was not less for participants with limited education or limited technical or computer experience than for those with more education or more advanced technical and computer skills. Thus, the highly technical aspect of the new cycler is able to promote learning for a wide range of learners. The cycler provides automated instruction using audio, video, and animation, and those features, combined with a qualified training nurse using a standardized script, appear to be both efficient and effective.
Recently, Baxter Healthcare Corporation designed a new PD cycler with embedded animation, visual images, and voice guidance. Animation has recognized advantages for learning: it can accentuate important details and actions, and avoid the visual clutter that can diminish the effectiveness of a live-action video (2). The animations include annotative elements, such as arrows to point out special features and indicate the direction of motion. Animation of information that is not observable in the real world, such as the cleansing of blood through a semipermeable membrane, helps users to develop accurate mental models of complex concepts. The new cycler animations include voiceover and subtitles to enhance comprehension, and users are able to play, pause, stop, and repeat the content, and also to control the volume. The device has been designed to facilitate learning under the guidance of a qualified training nurse.
The purpose of the present study was to evaluate the efficiency and effectiveness of PD training conducted by qualified training nurses who use standardized scripted training together with the new cycler, which allows them to enhance the training with audio, visual, and animated instruction.
Methods
Curriculum Design and Rationale
The curriculum for PD training in this study included these components:
A standardized script to guide the training nurse through the learning process. The script reflects established practice in PD training, as well as established learning principles, and integrates the instruction within the new cycler.
Automated instruction incorporated in the new cycler, with audio, video, and animation to facilitate learning. The cycler is designed to be used under the guidance of a qualified training nurse. The cycler design was based on market research in 2006 involving 120 nurses and nephrologists in the United States, Europe, and Asia (Baxter Healthcare Corporation, personal communication, November 2012).
The training nurse adheres to the course script, which is based on steps derived from established principles for teaching psychomotor skills (3):
Conceptualization: Understanding the cognitive elements of the skill, why and when it is done (or not done), and the instruments or tools used to perform it.
Visualization: Observing the procedure from beginning to end, which acts as a model for achievement.
Verbalization: Hearing narration of the steps in the procedure, coupled with another demonstration, and narrating those steps.
Practice: Practicing individual parts of the procedure and then combining the parts.
Correction and refinement: Correcting any errors identified at this point, and then repeating practice until errors are eliminated.
Mastery: Achieving error-free repetition of the procedure.
Acquiring a motor skill is a unique process requiring brain function and muscle training. Thus, the curriculum follows the three distinct stages in learning procedural motor skills: cognitive learning, in which the learner describes or reads the steps; practice, in which the muscles repeatedly perform the steps; and autonomic response, in which the brain programs the steps.
The instructional process begins with an explanation of the process, its purpose, and the tools involved (conceptualization). The learner then observes each procedure as the trainer performs it (visualization). The cycler provides audio and visual cues and illustrations for each step of the procedure as it is watched. No practice by learners is allowed until they are able to state each step in order (verbalization). Learner practice is guided by the animated cycler: they simply press a button to repeat steps as many times as desired until they are ready to practice them themselves (practice, correction and refinement).
All participants were recruited by a private research agency and were between 21 and 75 years of age. The participant sample of Boston residents included a balanced distribution of ages and a range of experience using computer technology. Potential participants were excluded if they were illiterate, because they had to be able to read the steps of each procedure on the cycler screen. Recruitment targets included both current automated PD (APD) patients and those naive to dialysis. In addition, those with visual, hearing, or touch impairments were purposely included to reflect disabilities common to the APD population. The definition of “impaired vision” was that the subject could see large print, but not regular print, in newspapers or books without corrective lenses. “Impaired hearing” was defined as being able to hear speech at conversational levels without a hearing aid, but with difficulty when not in quiet listening conditions or in one-on-one situations. “Impaired touch” was defined as the presence of strength problems with hands, arms, or legs, but with retention of the ability to perform activities of daily living without difficulty. All visually impaired participants in the study wore corrective lenses on the training day, and hearing-impaired participants who had hearing aids also wore them during training. Participants self-reported their impairments, which were then evaluated in a telephone interview to meet the defined study criteria. Participants also self-evaluated their comfort with technology and computers as low, moderate, or high, and they self-reported their education level.
Trainers for the study were all experienced PD training nurses who attended a “train the trainer” workshop for 2 days to learn the new cycler computer-assisted program and to practice the scripted training process. Trainer capabilities were not individually evaluated.
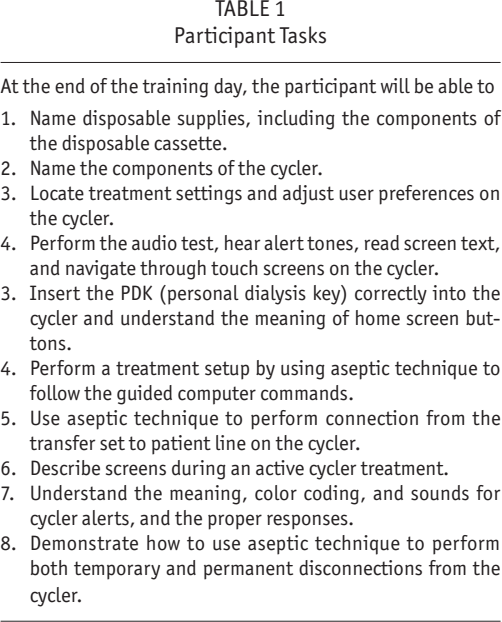
Training time began when the patient entered the training room with the training nurse and lasted until the participant met all stated objectives for the day. Included in the training time were two 15-minute breaks, one in the morning and the other in the afternoon, plus a 1-hour lunch break. All participants received between 4 and 8 hours of one-on-one training from the training nurse. Training took place in a private room in a research facility; the room had a door and contained 2 tables, 2 chairs, dialysis supplies, and the automated cycler. Training nurses followed the training script on a laptop as they and the participant progressed through the cycler training curriculum. The goal was for the participant to meet 8 learning objectives (Table 1) in a single training day. The training nurse adjusted the pace of training to meet individual abilities and needs.
Participant Tasks
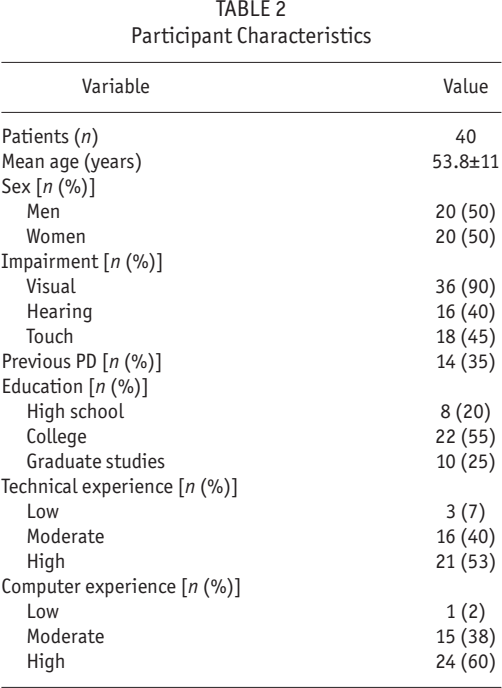
Participant Characteristics
Although patients usually train at least 5 days for PD, for the purposes of the present study, the participants received a single day of training lasting between 4 and 8 hours, with the standardized curriculum. All participants wore a PD apron with a PD catheter to perform all dialysis procedures. Participants with a personal PD catheter (that is, they were active on PD) were not allowed to perform any study procedures using their own PD catheter. At the end of the study day of training, the training nurse used a checklist that reflected the learning objectives listed in Table 1 to evaluate the participant for proficiency. To be deemed successful, participants had to meet all the objectives. The hours required to train each participant were recorded.
Statistical Analysis
Data are expressed as means with standard deviations or as medians with ranges, as appropriate for the distribution. We used the Student t-test to compare continuous variables, a one-way analysis of variance to compare groups, and a simple correlation to evaluate the relationship between variables. Statistical significance was deemed to be p > 0.05.
Written informed consent was obtained from each participant according to the Food and Drug Administration's Medical Device Use-Safety methodology and the International Organization for Standardization's Medical Devices—Application of Usability Engineering to Medical Devices standard (ANSI/AAMI/IEC 62366:2007). The test involved participants interacting with the medical device hardware and software user interfaces, essential accessories, disposable elements, and learning tools in a simulated-use environment.
Results
All 40 participants completed the study day of training. All 40 participants successfully met all task objectives by the end of the day. No participant was unable to meet the full set of learning objectives in the allotted study time.
The mean age of the study participants was 53.8 ± 11 years, with the women being significantly younger than the men (50 ± 12 years vs 57 ± 9 years respectively, p < 0.05). Ages ranged from 23 to 73 years. Of the study participants, 90% had visual impairments, 40% had hearing impairments, and 45% had touch impairments. Twenty-nine participants (73%) had multiple impairments: 3 had visual, hearing, and touch impairments; 13 had vision and hearing impairments; and 13 had vision and touch impairments. Participants represented a wide range of education levels and self-reported levels of technology and computer experience (Table 2); however, only 1 reported a low level of comfort with computers, and only 3 claimed a low level of comfort with technology. A college or higher-level education was reported by 80% of the participants; a moderate to high level of technical experience, by 93%; and a moderate to high level of computer skills, by 98%. One third of the participants had previous experience with PD (median: 3 years; range: 3 months – 10 years), with 13 having previously used a Baxter cycler, and 2 having previously used both Baxter and Fresenius cyclers. Twenty-seven participants were naive to PD.
Nine experienced PD training nurses used the defined curriculum to teach the 40 participants to use the new cycler. Two nurses trained 6 patients each, 4 trained 5 participants each, 1 trained 4 participants, 1 trained 3 participants, and 1 trained 1 participant.
Median training time was 7 ± 0.13 hours (range: 5 – 8.25 hours). We observed no correlation between the number of hours required to successfully train a participant and the age of that individual (r = 0.30). Training time did not differ significantly by sex, disability, experience with computers or technology, or education level (Table 3). Compared with participants naive to dialysis, those having previous experience with PD required less time for training (6.5 ± 0.7 hours vs 7 ± 0.8 hours), but the difference just missed statistical significance at p = 0.056.
Mean Training Times for Participants
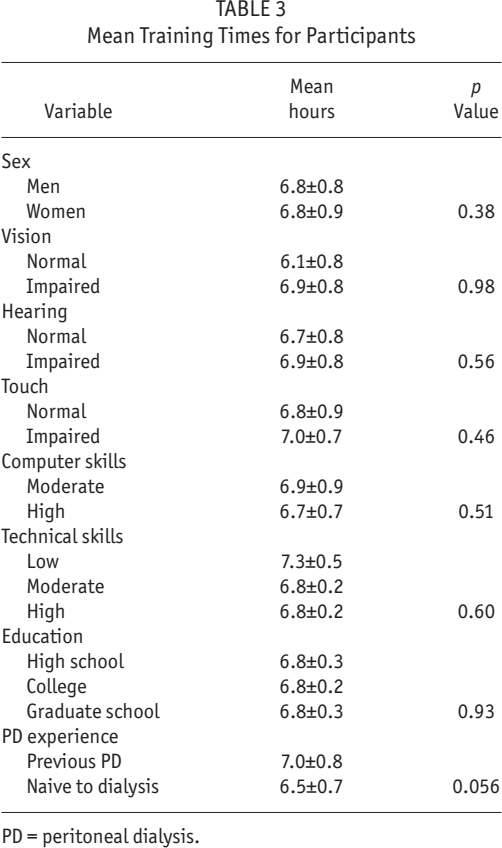
PD = peritoneal dialysis.
Discussion and Conclusions
The most striking finding of this study is that, despite a variety of barriers to learning, all 40 participants were able to meet all the stated objectives of the study with 4 – 8 hours of training. Compared with participants having more education and more advanced technical and computer skills, those with limited education or limited experience with technology or computers were no less able to meet the study objectives. Thus, the highly technical aspect of the new cycler is able to promote learning for a wide range of learners. Illiterate participants were, however, excluded from the current study; future research is needed to evaluate the effectiveness of computer-guided audio and visual cues in their training. The carefully designed automated instruction given by the cycler, using audio, video, and animation, combined with a qualified training nurse using a standardized training script, appears to be both efficient and effective in promoting PD patient learning.
Typically, a patient would require several days of training to learn how to perform PD safely at home. The patient would perform an increasing number of tasks independently while building experience with PD concepts and procedures. Training would continue until the point at which the trainer considers the patient sufficiently competent to perform PD safely at home. Training would vary in length and focus to account for a given user's aptitude, resulting in shorter or longer training periods. However, for the purposes of the present study, the training period was a single day, and participants were trained only on a subset of procedures.
Although use of the new cycler and a standardized training script may reduce the overall training time, the results of our study do not imply that all the procedures and concepts of PD can be learned in a single day. Learning research supports the importance of using spaced practice opportunities (4). Our study also does not suggest that a patient should be taught by the cycler alone without the support and direction of a training nurse. On the contrary, the combination of technology with a structured teaching plan in a one-on-one nurse– patient session appears to be a successful approach. Because repetition is a key part of the learning process, patients require many days to meet all the objectives of a full curriculum for PD training and to be fully prepared to perform PD safely at home. Multiple study opportunities, cued recall, and repeated testing have demonstrated positive effects on learning (5). In the present study, we used a single day of training so that we could evaluate the effectiveness of this new approach to teaching home PD. Use of the new cycler is likely to help standardize the teaching methods and curriculum for PD training, thus enhancing the effectiveness—and perhaps the efficiency—of the learning process for patients. Further study will be needed to determine if patient outcomes are improved with its use.
Previous studies of PD training are scarce. In 2004, Hall et al. (6) published a study in which a new curriculum for PD training was developed based on adult learning principles. The new curriculum was compared with the previous standard training in 32 clinics in the United States. Outcomes in the 246 patients who were thus trained were compared with outcomes in 374 patients who received the standard training. The patients taught with the new curriculum had significantly fewer peritonitis and exit-site infections during the subsequent observation period, indicating an important improvement in patient outcomes. Unfortunately, the curriculum developed by Hall and colleagues was never made available in the public domain and thus was never circulated for further use or validation. Holloway et al. (7) reported that pediatric patients whose training was both longer and more intensely focused on theory and technical skills had lower peritonitis rates. In 2007, Chow et al. (8) reported that patients trained by more experienced training nurses had higher rates of peritonitis than those trained by less experienced training nurses, perhaps because the more experienced nurses had not kept up to date on newer adult learning principles in education. No studies indicate how much training time is needed to properly prepare patients to perform PD safely at home, although one study reported that the average total training time over a number of days in the United States, Canada, and the Netherlands was 25 hours; in Hong Kong it was more than 35 hours; and in South America, it averaged about 20 hours (9).
Our study design was limited in that it lacked a comparison group to allow for an evaluation of differences with current training methods. The sample size of 40 participants was small, and we performed no power calculations. The training capabilities of the training nurses, which were not assessed, may have varied. Most participants had a relatively high education level. Technical and computer skills were evaluated subjectively by each participant; only 3 people reported having low-level technical skills, and only 1 reported having low-level computer skills. Because of the study design, the results of this study may not be generalizable.
Despite the limitations, we conclude that this study opens a window to innovations in patient training for PD. The use of automated instruction with audio, video, and animation embedded in the cycler, combined with a standardized training script, appears to be effective in promoting learning for PD. Further studies are needed to compare computer-assisted training with current APD training methods and to evaluate the effects of training methods on peritonitis rates and technique survival.
Footnotes
JB is a consultant for Baxter Healthcare Corporation and PuraCath Medical Inc. DJD has no financial conflicts of interest.