
Abstract
♦Background
Peritoneal dialysis (PD) solutions containing icodextrin as the osmotic agent have advantages during long dwells. The glucose polymers that constitute icodextrin are a heterogeneous mix of molecules with a polydispersity [ratio of weight-average to number-average molecular weight (Mw/Mn)] of approximately 2.6. The present study evaluates whether modifications in the polydispersity and concentration of glucose polymers can improve ultrafiltration (UF) without an associated increase in carbohydrate absorption (CA).
♦Methods
Computer simulations using a three-pore model of peritoneal transport during a long dwell in PD patients predict that, in general, compared with 7.5% icodextrin, glucose polymers with a Mw greater than or equal to 7.5 kDa, a polydispersity less than 2.6, and concentrations greater than 7% could achieve higher UF without higher CA. Based on the simulations, we hypothesized that, compared with 7.5% icodextrin, glucose polymers with a Mw of 18 – 19 kDa and a polydispersity of 2.0 at 11% concentration could achieve higher UF without a higher CA. We tested this hypothesis in experimental studies using 8-hour dwells in New Zealand White rabbits. In those studies, UF was measured by complete fluid collection, and CA was measured by subtracting the total carbohydrate in the collected fluid from the carbohydrate initially infused.
♦Results
The UF was higher with 11% 19 kDa glucose polymer than with 7.5% icodextrin (mean ± standard deviation: 89 ± 31 mL vs 49 ± 15 mL; p = 0.004) without higher CA (5.2 ± 0.9 g vs 5.0 ± 0.9 g, p = 0.7). Similar results were seen with the 11% 18 kDa glucose polymer, which, compared with 7.5% icodextrin, resulted in higher UF (mean ± standard deviation: 96 ± 18 mL vs 66 ± 17 mL; p < 0.001) without higher CA (4.8 ± 0.7 g vs 5.2 ± 0.6 g, p = 0.2).
♦Conclusions
The findings demonstrate that, compared with 7.5% icodextrin solution, long-dwell PD solutions containing 11% glucose polymers with a Mw of 18–19 kDa and a polydispersity of 2.0 can provide higher UF without higher CA.
An important consideration in evaluating polymer osmotic agents as alternatives to icodextrin in PD solutions that has not been addressed in previous theoretical studies (6,7) is safety profile. This characteristic is influenced by the amount of the osmotic agent that is absorbed from the peritoneal cavity during the dwell, the rate of metabolism of the osmotic agent, and the toxicity of the resulting metabolic breakdown products (“metabolic profile”). When the analysis is limited to glucose polymers, the latter two factors should be similar for all candidates, such that the safety of various glucose polymer formulations should depend primarily on the amount and the metabolic impact of the carbohydrates absorbed.
The concept of UF efficiency, the ratio of UF to the amount of carbohydrate absorbed, has previously been introduced to compare various osmotic agents (3,4,8), with higher UF efficiency resulting from either higher UF or lower carbohydrate absorption. Although UF efficiency is often thought to be intrinsic to a given osmotic agent (3,4), recent work (8) showed that the UF efficiency of glucose-based PD solutions is time- and concentration-dependent, as will also be apparent for glucose polymer-based solutions from the present work. In the latter case, the total amount of carbohydrate absorbed at a given concentration and dwell time is a useful parameter to consider when evaluating the metabolic impact of glucose polymer formulations.
We recently showed that rabbits can be used as experimental subjects for evaluating glucose polymers with low polydispersity as osmotic agents for PD solutions (9). In that study, we demonstrated that a low molecular weight (6 kDa) glucose polymer was more effective at generating UF and had a higher UF efficiency than a high molecular weight (19 kDa) glucose polymer when tested at the same concentration (7.5%). However, the higher UF efficiency for the low molecular weight glucose polymer was achieved at the expense of higher absorption of the osmotic agent from the peritoneal cavity. In the studies described here, we first theoretically evaluated the effect of concentration on UF and carbohydrate absorption for various glucose polymers with low polydispersity. Based on those computer simulations, we then experimentally tested whether higher UF could be produced by certain glucose polymers than by icodextrin, without higher carbohydrate absorption.
Methods
Theoretical
The three-pore model was used to simulate UF and carbohydrate absorption as a function of time during a long dwell based on PD Adequest 2.0 (2) as recently implemented [Galach M, Vonesh E, Akonur A, Waniewski J. Impact of polydispersity of glucose polymers on UF and UF efficiency. Presented at the 10th European Peritoneal Dialysis Meeting (EuroPD 10); Birmingham, England; 21 – 23 October 2011 (presentation O-23)]. Simulations considered a 12-hour dwell for 3 representative patients of high, high-average, and low-average transport type according to UF profiles obtained from previous evaluations (2). A wide range of glucose polymers were considered, with weight-average molecular weights between 1 kDa and 24 kDa, polydispersities between 1.6 kDa and 2.4 kDa, and concentrations between 4.0% and 15.0%. For all glucose polymers, including icodextrin, molecular weight distributions were assumed to be log-normal, and carbohydrate absorption was calculated as the mass of glucose polymer infused minus the mass remaining after 12 hours. It was assumed that the volume of dialysate infused into the peritoneal cavity was 2 L and that the residual fluid volume was equal to the volume measured during dwell studies in patients (2); the residual fluid volume varied between the patients (90 – 235 mL), but remained invariant for each representative patient. Net UF was determined as the volume in the peritoneal cavity after 12 hours minus the residual fluid volume.
Experimental
Special Materials
Experimental 18K and 19K glucose polymers with low polydispersity were obtained by additional fractionation of commercial icodextrin. These fractions were intended to be similar, but were prepared at different times from different starting materials. The target polydispersity of the polymers was 2.0, and the target weight-average molecular weights were 18 kDa and 19 kDa respectively. The molecular weight averages of these glucose polymers were determined by size exclusion chromatography.
Procedures
Female New Zealand White rabbits with body weights ranging between 2.35 kg and 2.90 kg were used as experimental subjects. Intraperitoneal catheters (pediatric Tenckhoff catheters, Kendall– Quinton: Covidien, Mansfield, MA, USA) were surgically implanted in each rabbit by securing the first felt cuff on the catheter just outside the peritoneal cavity. The catheter was then guided through a subcutaneous tunnel, exiting at the subcapsular region and secured with sutures. The rabbits were allowed to recover for 7 days before any solutions were infused into the peritoneal cavity.
Three different studies were performed. Study 1 compared solutions containing 7.5% icodextrin (n = 9) with solutions containing 11% 19K glucose polymer (n = 9). Study 2 compared solutions containing 7.5% icodextrin (n = 12) with solutions containing 11% 18K glucose polymer (n = 12). A control study compared solutions containing 11% icodextrin (n = 9) with solutions containing 11% 19K glucose polymer (n = 9). During all studies, each rabbit was randomly assigned to one of the two glucose polymers. The volume of each infusion or dwell was adjusted for body weight (40 mL/kg), and the dwell time was 8 hours for all experiments. The investigators were blinded to the identity of the test glucose polymer solutions during the experiments.
Test solutions were prepared by combining approximately 7.5 g icodextrin or 11 g of either icodextrin or glucose polymer, 535 mg sodium chloride, 448 mg sodium lactate, 25.7 mg calcium chloride, and 5.08 mg magnesium chloride to make 100 mL of solution. The endotoxin content of the glucose polymers were less than 0.05 EU/ mL when tested using a limulus amoebocyte lysate assay. The solutions were filtered using a 0.2 μm filter and heated to 37°C before use.
Blood samples were taken at 0, 4, and 8 hours, and effluent samples were taken at 2, 4, and 8 hours of each dwell. After complete drainage of the peritoneal cavity, the rabbits were euthanized. The abdominal cavity was then opened, and the remaining fluid was aspirated using a 60 mL syringe. All collected peritoneal fluid was then combined and measured gravimetrically. The net UF volume was calculated as the final collected volume minus the initial infused volume.
Plasma and dialysate concentrations of urea nitrogen and creatinine were measured using an autoanalyzer. Dialysate-to-plasma concentration ratios were calculated by dividing the dialysate concentration by the plasma concentration at 4 and 8 hours. Clearances for urea nitrogen and creatinine were calculated by multiplying the final collected volume by the dialysate-to-plasma ratio divided by the dwell time (480 minutes).
The total carbohydrate concentration of the glucose polymer was measured using a previously developed analytical method for icodextrin (10). The amount of glucose polymer carbohydrate absorbed from the peritoneal cavity was calculated as the difference between the mass infused into the peritoneal cavity (initial concentration x initial volume) and the mass recovered at the end of the dwell (final concentration x final volume).
All comparisons between the various glucose polymer solutions were performed using an unpaired Student t-test.
Results
Theoretical
The effects of molecular weight, polydispersity, and concentration of the glucose polymers on net UF and carbohydrate absorption during a 12-hour dwell were extensively examined by computer simulations over the entire range of specified parameters. Figure 1 shows exemplar simulation results for a high-transport patient using either glucose polymer with weight-average molecular weights of 6 kDa and 19 kDa and various polydispersity and concentration values, or 7.5% icodextrin. Simulations showed that, compared with 7.5% icodextrin, 7.5% 6 kDa glucose polymer of low polydispersity achieved a higher net UF volume, but with higher carbohydrate absorption. In contrast, compared with 7.5% icodextrin, 7.5% 19 kDa glucose polymer of low polydispersity achieved both lower net UF and lower carbohydrate absorption. These theoretical results are qualitatively comparable to those we reported previously based on experiments in a rabbit model (9). Decreasing the polydispersity of either glucose polymer without altering the weight-average molecular weight had a minor effect on net UF, but resulted in substantially lower carbohydrate absorption.
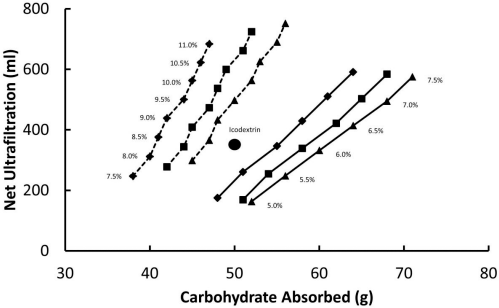
Theoretical predictions from a three-pore model of peritoneal transport: net ultrafiltration and carbohydrate absorbed with different glucose polymers as the osmotic agent for a high-transport patient. The large circle indicates the calculated result for 7.5% icodextrin; the solid and dashed lines indicate the calculated results for glucose polymers with weight-average molecular weights of 6 kDa and 19 kDa respectively. The calculated results for the glucose polymers also reflect various polydispersities—1.6 (diamonds), 2.0 (squares), and 2.4 (triangles)—and various percentage concentrations.
Various concentrations of the glucose polymers were then explored. In these simulations, the concentration of the 6 kDa glucose polymer was lowered to limit carbohydrate absorption and the concentration of the 19 kDa glucose polymer was increased to increase net UF. It can be observed from the simulations shown in Figure 1 that reducing the concentration of the 6 kDa glucose polymer resulted in both lower net UF and lower carbohydrate absorption. When the amount of carbohydrate absorption was lowered to be equivalent to that for 7.5% icodextrin, the predicted UF was less than that for 7.5% icodextrin. Thus, the three-pore model suggests that it would not be possible to achieve a higher UF with a 6 kDa glucose polymer than with 7.5% icodextrin without also incurring higher carbohydrate absorption. Those findings also imply that the UF efficiency of the 6 kDa glucose polymer is concentration-dependent: it decreases when the concentration of that glucose polymer decreases. In contrast, increasing the concentration of the 19 kDa glucose polymer resulted in sharply higher net UF without incurring substantially higher carbohydrate absorption. Here again, the UF efficiency of the 19 kDa glucose polymer is concentration-dependent: it increases when the concentration of that glucose polymer increases. These theoretical results suggest that, compared with 7.5% icodextrin, certain concentrations of a 19 kDa glucose polymer that exceed 7.5% can achieve higher UF with equivalent or even less carbohydrate absorption, provided that polydispersity is low. Similar, but less marked, theoretical results were observed for patients with high-average and low-average transport characteristics.
These theoretical simulations provided the foundation for selecting an experimental formulation containing glucose polymers of 19 kDa at 11% concentration and a polydispersity of 2.0. We then tested this glucose polymer formulation in a rabbit model.
Experimental
Table 1 shows the weight-average and number-average molecular weights of the glucose polymers tested experimentally. The molecular weight distribution of the 19K glucose polymer, compared with that of icodextrin, was independently determined by García–López, Lindholm, and colleagues (11-13); Figure 2 shows the results from those determinations. The polydispersity of the 19K glucose polymer is less than that of icodextrin; it was achieved primarily by reducing the relative mass of low molecular weight polymers and increasing the relative mass of middle molecular weight polymers.
Measured Molecular Weights of Test Glucose Polymers
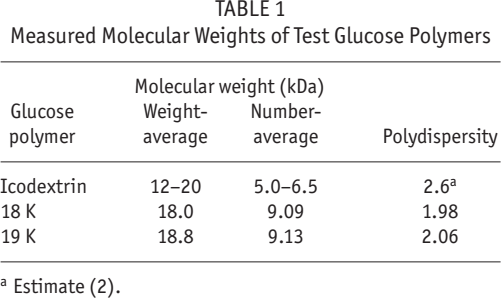
Estimate (2).
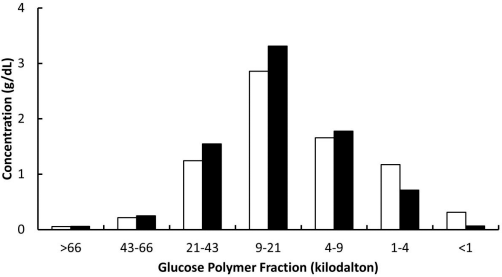
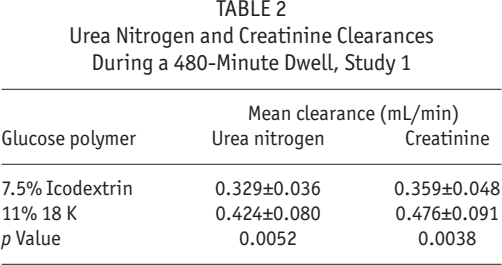
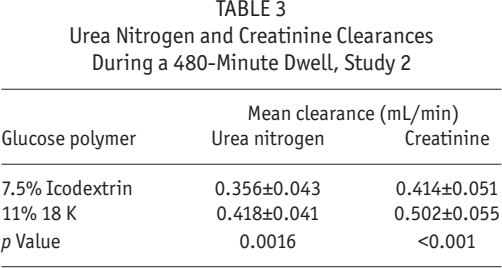
Figure 3 and Table 2 summarize the results from study 1. When using the 11% 19K glucose polymer, net UF was higher than it was for 7.5% icodextrin (p = 0.004), without higher carbohydrate absorption (p = 0.7). This higher net UF was accompanied by higher clearances for both urea nitrogen (p = 0.0052) and creatinine (p = 0.0038). Figure 4 and Table 3 summarize the results from study 2. When using the 11% 18K glucose polymer, net UF was higher than it was for 7.5% icodextrin (p < 0.001), without higher carbohydrate absorption (p = 0.2). The higher net UF was accompanied by higher clearances for both urea nitrogen (p = 0.0016) and creatinine (p < 0.001). The increases in small-solute clearances observed with the use of the 18K and 19K glucose polymers were likely attributable to increased UF and not to altered permeability of the peritoneum.
Urea Nitrogen and Creatinine Clearances During a 480-Minute Dwell, Study 1
Urea Nitrogen and Creatinine Clearances During a 480-Minute Dwell, Study 2
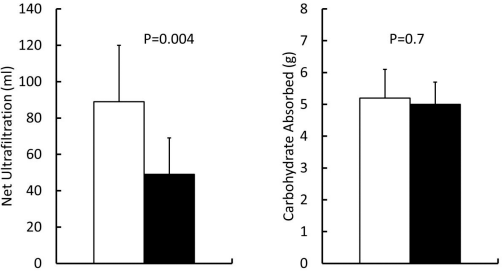
Net ultrafiltration and carbohydrate absorbed during study 1: the 19K glucose polymer at a concentration of 11% (white bars) and icodextrin at a concentration of 7.5% (black bars).
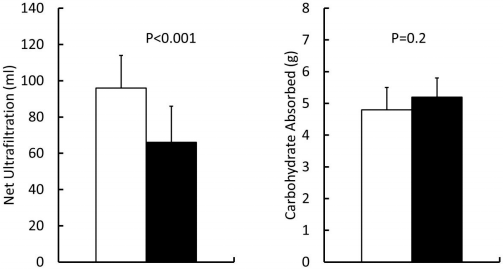
Net ultrafiltration and carbohydrate absorbed during study 2: the 18K glucose polymer at a concentration of 11% (white bars) and icodextrin at a concentration of 7.5% (black bars).
Figure 5 shows net UF and carbohydrate absorption for the control study. Net UF was not different (p = 0.2) when using 11% 19K glucose polymer or 11% icodextrin; however, carbohydrate absorption was higher (p = 0.03) when using 11% icodextrin. No differences were observed in the urea nitrogen or creatinine clearances generated by these osmotic agents (data not shown).
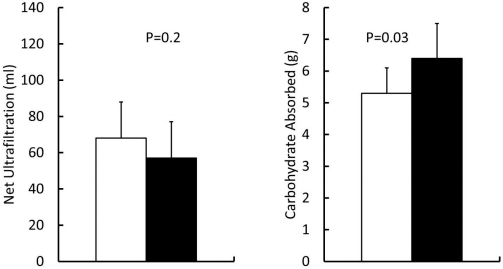
Net ultrafiltration and carbohydrate absorbed during the control study: the 19K glucose polymer at a concentration of 11% (white bars) and icodextrin at a concentration of 11% (black bars).
Discussion
Previous work by other authors has suggested that monodisperse large molecular weight polymers or colloids can be used as osmotic agents based on theoretical calculations from a three-pore model of the peritoneum (6,7); however, those calculations did not consider the amount of osmotic agent absorbed from the peritoneal cavity. The amount of absorbed osmotic agent might be significant when considering glucose polymers of low polydispersity as alternatives to icodextrin, given that use of the latter osmotic agent is associated with elevated serum levels of icodextrin metabolites (oligosaccharides) (14) that can lower serum sodium and chloride concentrations and might induce rare adverse side effects such as rash or exfoliative dermatitis (15). Although the use of glucose polymers that result in higher carbohydrate absorption might be useful clinically, the occurrence of adverse side effects could depend directly on the amount of carbohydrate absorbed. Further, an increase in carbohydrate absorption might contribute to metabolic syndrome (16), increase visceral fat mass, and enhance dyslipidemia in PD patients (17). Thus, any glucose polymer proposed as a new osmotic agent would have the greatest likelihood of clinical success if it were not associated with higher carbohydrate absorption. Based on that reasoning, our theoretical simulations took into consideration the amount of carbohydrate absorption from the peritoneal cavity during a long dwell.
Our theoretical computer simulations using a three-pore model of peritoneal transport showed that glucose polymers of low polydispersity and low weight-average molecular weight (<7.5 kDa) cannot achieve the goal of higher net UF without higher carbohydrate absorption. The higher net UF with these low molecular weight glucose polymers is accompanied by enhanced carbohydrate absorption because of the more rapid diffusion of smaller polymers from the peritoneal cavity. If lower concentrations of such glucose polymers are considered (so as to reduce carbohydrate absorption), UF is also reduced substantially because of the reduction in osmotic driving force. In contrast, our theoretical simulations demonstrated that glucose polymers of low polydispersity and a high weight-average molecular weight (>7.5 kDa) can achieve the desired goal. Indeed, additional theoretical simulations (not shown) have demonstrated that any glucose polymer with a weight-average molecular weight greater than or equal to 7.5 kDa can achieve the desired goal, with the specific concentration range and polydispersity depending on the weight-average molecular weight (18). It should be emphasized that the criteria chosen in this study and the current theoretical predictions are exclusive for polymers of glucose with the same metabolic fate as icodextrin.
Our experimental studies demonstrate that a glucose polymer with a polydispersity of approximately 2.0 and a weight-average molecular weight of 18 – 19 kDa at a concentration of 11% can achieve higher UF without higher carbohydrate absorption than occurs with 7.5% icodextrin. Routine use of a PD solution comprising such osmotic agents would presumably allow patients to safely reduce the number of hypertonic glucose solutions used in daily therapy. Our experimental findings also demonstrate that the same goal might not be achievable simply by increasing the concentration of icodextrin to 11% because of potential safety concerns related to higher carbohydrate absorption.
It is important to note that the osmotic pressure of solutions containing 11% of the 18K or 19K glucose polymers tested in our experimental studies should have an osmotic pressure similar to that for solutions containing 7.5% icodextrin despite the difference in total glucose polymer concentration. The calculated osmotic pressure, expressed as an osmolar concentration, contributed to the solution by 7.5% icodextrin is 11.5 – 15 mmol/L, assuming a number-average molecular weight of 5 – 6.5 kDa; for the 11% 18 kDa or 19 kDa glucose polymers in Table 1, the calculated pressure is approximately 12 mmol/L. [Note that the osmolar concentration relevant for determining the osmotic pressure of polymer solutions is the mass concentration divided by the number-average molecular weight (19).] These calculated osmotic pressures were not validated in the present study because they are difficult to measure accurately.
Our experimental results were obtained in a rabbit model that we have previously used to study glucose polymer osmotic agents (9). The current experiments were similar in design, except that the dwell was extended to 8 hours from 4 hours. The use of a longer dwell time was based on additional studies in this rabbit model using radiolabeled albumin as a volume marker. Those studies showed that the maximum peritoneal volume when using icodextrin as the osmotic agent occurred after approximately 4 - 6 hours [Hoff CM, Piscopo D, Carr S, Svatek JM, Holmes CJ, Wang R, et al. Evaluation of glucose and icodextrin-based bimodal PD solutions in a rabbit model. Presented at the 10th European Peritoneal Dialysis Meeting (EuroPD 10); Birmingham, England; 21 - 23 October 2011 (presentation P-1)]. There are two advantages of using a rabbit model rather than a rat model to evaluate dialysis solutions containing glucose polymers as osmotic agents:
Levels of serum amylase in rats are higher than those in rabbits by a factor of 10 (≅2000 U/L vs ≅200 U/L).
When icodextrin is used as the osmotic agent, the UF kinetics in rat models of PD have been reported to differ significantly from those in PD patients (10,20-22).
It should be emphasized that our theoretical work was developed for PD patients, but that our experimental results were obtained in a rabbit model. Thus, certain quantitative discrepancies between our theoretical work and our experimental findings might be expected; nonetheless, the combined results clearly demonstrate proof of principle.
Additional limitations to this study require further discussion.
First, the accuracy of our computer simulations depends on the relative validity of the three-pore model to predict UF and carbohydrate absorption. It is known that the three-pore model cannot predict UF profiles in all patients during long dwells when using icodextrin (23), and the ability of the model to predict carbohydrate absorption has not yet been quantitatively validated.
Second, the computer simulations assumed a constant residual volume within the peritoneal cavity for each patient. Theoretical work by our group (24) recently demonstrated that large amounts of residual fluid within the peritoneal cavity before a long-dwell exchange using icodextrin solution can substantially reduce UF; however, the differential effect of residual fluid volume on icodextrin or an 18 - 19K glucose polymer solution is expected to be small.
Third, it should be emphasized that the rabbit model used in the current study is nonuremic; thus, plasma concentrations of urea nitrogen and creatinine are low (that is, within the normal range). The low plasma concentrations of these solutes magnify small biases in analytical methods that make precise evaluation of small-solute transport across the peritoneum difficult.
Fourth, the use of an 8-hour dwell in our rabbit experiments might be considered somewhat arbitrary. As already mentioned, our unpublished data suggest that dwell studies between 4 hours and 8 hours in the rabbit provide an approximate plateau in net UF, similar to that observed in PD patients from 10 hours to 14 hours (25). The relative equivalency of 4- to 8-hour dwell studies in the rabbit and 10- to 14-hour long-dwell exchanges in PD patients are approximately those predicted by Rippe (26) by scaling fluid and solute peritoneal transport appropriately by body weight and body surface area.
Finally, the UF measurements in our rabbit experiments could potentially be affected by residual volume that might have been present before the dialysis solution was infused.
Conclusions
Taken together, the theoretical and experimental evidence suggest that an alteration in both the molecular weight distribution and the concentration of glucose polymers is needed to provide new and improved long-dwell glucose polymer–based osmotic agents. Further, compared with 7.5% icodextrin solutions, long-dwell PD solutions containing 11% 18 – 19 kDa glucose polymers with low polydispersity can provide higher UF without higher carbohydrate absorption.
Footnotes
Acknowledgments
The authors thank Dean Piscopo, Seraya N. Carr, and Jessica M. Svatek for technical support. All funds for this work were provided by Baxter Healthcare Corporation.
All authors are employees of Baxter Healthcare Corporation with ownership interest.