
Abstract

Dear Dr. Wallace,
Thank you for your thoughts and comments on our paper “Travel distance and home dialysis rates in the United States”. With regards to the designation of home dialysis units, our data came from the end-stage renal disease (ESRD) networks directly and not from the USRDS database. As such, we were able to request more specific detail for this study. Each facility designated as a home dialysis facility had at least 1 patient there on a home dialysis modality (either peritoneal dialysis (PD) or home hemodialysis (HHD)) and this was confirmed with ESRD network 10, where the data was compiled.
With regards to the distances presented in the paper, we ran 2 separate analyses for the paper (not mentioned in the abstract because of space limits) – 1 with all patients in the study (177,606) and 1 with only the patients who dialyzed at units with both in-center hemodialysis (IHD) and a home dialysis modalities (PD, HHD or both). The adjusted analyses contained many factors that were felt to potentially influence modality utilization in addition to travel distance. It was felt by our reviewers that the patients attending facilities without home dialysis options may not truly have a choice of modality, hence we limited the sample to patients attending facilities with both IHD and home modalities. When all 177,606 patients were included in the distance calculations, the median travel distances to patients’ initial dialysis facilities were 5.7 miles, 12.6 miles, and 17.8 miles, respectively for IHD, PD, and HHD patients, respectively (Table 1). Comparatively, these respective distances for the group attending facilities with home dialysis and IHD options were 5.4 miles, 3.5 miles, and 6.5 miles, respectively (Table 1).
Distances to Initial and Closest Facilities for Limited Sample and Excluded Patients
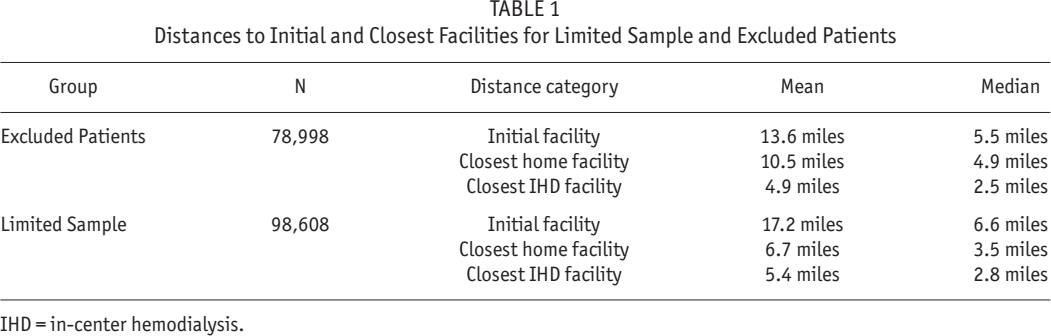
IHD = in-center hemodialysis.
Although the median distances are similar, the mean distances indicate that the limited sample patients may live further from IHD facilities, but closer to home dialysis facilities and also traveled farther to their initial facilities. For the overall sample (177,606 patients), the distances to initial, closest home and IHD facilities were 2.7, 4.0, and 6.1 miles, respectively.
The main concern is that limiting the sample may have influenced our results. Travel distance may have a varying effect on modality choice. We therefore present the adjusted analyses for predictors of PD and HHD utilization in the overall sample of 177,606 patients in the supplemental Tables 2 and 3, respectively. Patients with an increased distance to closest in-center dialysis facility were more likely to utilize PD. Although the distance to closest home dialysis facility significantly impacted PD utilization in the limited sample, this was not the case for the overall sample. The main difference between the limited and overall sample results for PD utilization was that the former group contained the vast majority of the home dialysis patients and there were very few home dialysis patients in the group attending facilities without home modalities (by default). For HHD utilization, the limited sample showed higher HHD use in patients living further from home dialysis facilities and less use of HHD with increased distance to an in-center dialysis facility. However, in the overall analyses, distance was not a significant predictor of HHD utilization, though there was a trend towards less use of HHD with increased distance to a home dialysis facility.
As mentioned in the original paper, the main limitation for HHD was that we could not separate the facilities offering PD vs HHD vs both. This would have allowed us to get a more accurate estimate of travel distances for HHD patients. We were not able to separate the percentage of facilities offering PD vs HHD and we suspect, given travel distances, that fewer facilities offer PD than IHD and still fewer offer HHD than PD. However, this might be looked at in future studies. A registry study may not be the most optimal way to determine the relationships between dialysis modality utilization and travel distance. Several issues, such as wanting to dialyze at a facility where one's nephrologist works, that are not captured in the registry may be more influential to modality utilization and better studied using other methods. Our study provided an initial estimate of travel distances for each modality and further examination of this is warranted, especially in rural areas.
The limited sample had similar percentages of patients in rural, micropolitan and metropolitan areas as the overall sample. Some of the differences shown in Table 1 of the original article that are statistically significant may not necessarily be clinically significant. For example, although the numbers in Table 1 of the original paper are significant, there likely is not a clinical difference between 2.1 and 2.2% rural population. For the overall sample (refers to 177,606 patients), 152,933 (86.6%) resided in metropolitan areas, 19,555 (11%) in micropolitan areas, and 3706 (2.2%) in rural areas. Hence, as stated in the original paper, we cannot assume these results are reflective of rural areas which, due to the study limitations, we were not able to assess in more detail. We agree with Dr. Wallace that travel distances and distribution of dialysis options should be more specifically examined in rural areas.
Yours Sincerely,
Footnotes
The analysis upon which this publication is based were performed under Contract Number ESRD Network 9, contract number HHSM-500-2010-NW009C entitled End Stage Renal Disease Networks Organization for the States of California, Arizona, New Mexico, Colorado, Utah, Pennsylvania, Delaware, Hawaii, Illinois, Kentucky, Ohio and Indiana, sponsored by the Centers for Medicare & Medicaid Services, Department of Health and Human Services. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented. This article is a direct result of the Health Care Quality Improvement Program initiated by the Centers for Medicare & Medicaid Services, which has encouraged identification of quality improvement projects derived from analysis of patterns of care, and therefore required no special funding on the part of this contractor.