
Abstract

Editor:
Hepatic portal venous gas (HPVG) is a rare but serious condition that has been associated with a poor prognosis. It occurs when intraluminal gas or gas produced by intestinal bacteria enters the portal venous circulation. Hepatic portal venous gas has been reported in many illnesses, ranging from benign conditions to potentially lethal diseases that require urgent surgical intervention. Intestinal obstruction is a common manifestation in patients with encapsulating peritoneal sclerosis (EPS). However, among the various diseases, HPVG-associated EPS has not been described. We report on a patient with EPS complicated by intestinal obstruction that lead to the development of HPVG. The patient made an uneventful recovery with medical treatment.
A 76-year-old female patient who had had end-stage renal disease for 15 years received maintenance hemodialysis 3 times a week. She had stopped peritoneal dialysis (PD) 2 years prior due to EPS. The patient presented to our emergency department with progressive worsening of abdominal pain over the previous 3 days. On examination, she was hypothermic, with a body temperature of 35.1°C, blood pressure 80/40 mmHg, respiratory rate 20 breaths per minute, and heart rate 111 beats per minute. Abdominal examination revealed a soft abdomen with no guarding or rigidity on light palpation. The patient's bowel sound was hypoactive. The abdomen and pelvis computed tomography (CT) scan showed a large quantity of ascites and free air in the intrahepatic portal veins and along the falciform ligaments (Figure 1). Disproportional dilatation of the proximal small bowel and collapse of the distal ileum and colon were also found. These findings suggested intestinal obstruction at the jejuno-ileal junction. In addition, a large quantity of loculated fluid accumulation was noted in the anterior peritoneum, with peritoneal thickening. The walls of the small bowel were calcified. Her ascites tap showed the presence of bloody fluid collection. A diagnosis of EPS was made based upon her clinical symptoms and radiological features. After being admitted to the intensive care unit, the patient was found to have a white blood cell count of 19,430 cells/μL and C-reactive protein of 38.4 mg/dL. Because of high anesthetic and surgical risks, a laparotomy was not performed. We had kept the patient on nothing per os and gave her 500 mg intravenous meropenem daily as the empirical antibiotic of choice and parenteral nutrition. The patient's blood pressure improved after fluid resuscitation. The blood culture results yielded growth of Enterococcus raffinosus, and she received teicoplanin 400 mg daily intravenously in addition to meropenem. The patient's clinical condition gradually improved, with decreased abdominal pain and increased bowel movement. On day 6 after admission, she was transferred to a regular ward and started intake of free water. Her blood cultures on day 10 showed negative bacterial growth. On day 14, an abdominal CT showed a patent portal vein without any air retention (Figure 2). On day 15, she was discharged home.
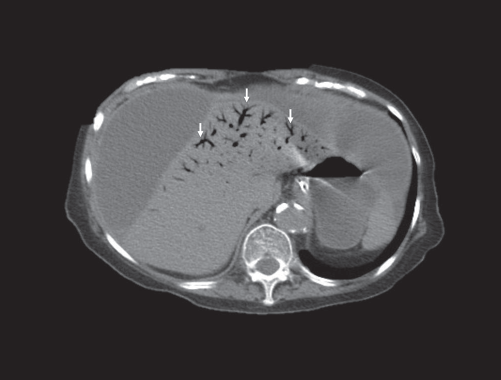
Computed tomography in a patient with peritoneal sclerosis. A large amount of loculated fluid had accumulated in the anterior peritoneum, with peritoneal thickening. Intestinal obstruction at jejuno-ileal junction was found due to an adhesion band around the jejuno-ileal junction. Air was noted in the intrahepatic portal veins and along the falciform ligament (arrows).

Computed tomography in the patient after medical treatment. Computed tomography showed resolution of hepatic portal venous gas (HPVG). Hepatic portal veins were patent without air retention.
Although intestinal obstruction is known to be a cause of HPVG, patients with EPS complicated with bowel obstruction have not been reported as developing HPVG. Furthermore, E. raffinosus bacteremia has been reported in increased frequency in patients with catheter-associated blood stream infection (1). This notion was reflected in the risk of E. raffinosus bacteremia in our patient, who had a permanent catheter as a vascular access in hemodialysis. The presence of HPVG may result in a life-threatening complication but does not always require surgical management (2), which is warranted only if there is evidence of peritonitis or bowel perforation. Conservative management may be applied in clinically stable patients without evidence of bowel perforation (3). Due to the complicated nature of EPS in our patient, both anesthesia and surgical risks precluded surgery as medical treatment. She was therefore treated conservatively with fluids and analgesics, with eventual improvements in her symptoms and CT results. In summary, we have described a case of HPVG in a female EPS patient. This case illustrates the need to recognize a rare complication in PD patients with EPS. Our patient's HPVG was effectively managed conservatively.