
Abstract
Background
Daily gentamicin cream exit-site prophylaxis reduces peritoneal dialysis (PD)-related gram-negative infections. However, there is a concern about the potential for increasing gentamicin resistance with the long-term use of prophylactic gentamicin. This study evaluated the incidence of gentamicin-resistant PD-related infections over more than 2 decades.
Methods
Study data on prevalent PD patients were retrieved from a prospectively maintained institutional review board (IRB)-approved PD registry at a single center from January 1, 1991, to December 31, 2000, and January 1, 2004, to December 31, 2013. The rates of gram-negative infections, fungal infections and those infections with organisms resistant to gentamicin were examined for the 2 periods. Period 1 from 1991 to 2000 when S. aureus prophylaxis consisted initially of oral rifampin to treat nasal carriage with S. aureus, and was then daily exit-site mupirocin ointment for all PD patients, was compared to the period from 2004 to 2013 when daily exit-site gentamicin cream was prescribed as prophylaxis (Period 2).
Results
The study included a total of 444 PD patients (265 and 179 in Period 1 and Period 2, respectively). No significant difference was noted in demographics between the 2 periods except race. The gram-negative exit-site infection rates for Period 1 and Period 2 were 0.109 versus 0.027 (p < 0.0001). Gram-negative peritonitis rates were similar. There were 3 episodes of gentamicin-resistant infections in each period. Fungal infections remained consistently low.
Conclusion
Despite a decade of exit-site gentamicin prophylaxis, gentamicin-resistant PD-related infections and fungal infections remained very low and similar to the prior period.
Keywords
Materials and Methods
Information on all PD-related infections and demographics at a single outpatient home dialysis center was collected from January 1, 1991, to December 31, 2000, and January 1, 2004, to December 31, 2013, on all adult patients who were on home PD participating in an institutional review board (IRB)-approved registry. More than 99% of patients starting PD at the center agreed to participate. Study data included only those patients who consented to be part of the registry.
Prior to 1989, there was no protocol for prevention of exit-site infection in our program. In 1989, PD patients with positive S. aureus nasal culture (done at each monthly clinic visit) were treated with a 5-day course of oral rifampin. From 1992 to 1994, a randomized trial of mupirocin calcium ointment 2% applied to the exit site daily versus cyclic oral rifampin to prevent PD-related infection was performed. After that, exit-site prophylaxis protocols were as follows: Daily exit-site mupirocin was prescribed for all patients. From July 2001 to 2003, a randomized controlled trial of exit-site mupirocin versus gentamicin was conducted, following which daily gentamicin cream prophylaxis was prescribed for all patients. We reviewed the electronic medical records retrospectively and compared 2 periods of time: Period 1 which was mainly for S. aureus prophylaxis (1991 – 2000) and Period 2 in which gentamicin cream was applied for prevention of both S. aureus and gram-negative exit-site organisms (2004 – 2013). Specifically, we examined the rates of gentamicin-resistant gram-negative as well as fungal PD-related infections. The randomized controlled trial period (2001 – 2003) was excluded from the study.
Catheter-related infections were defined as erythema, edema, or drainage at the exit site (exit-site infection) or erythema, tenderness, or swelling over the subcutaneous tunnel (tunnel infection), and were diagnosed by the nephrologist or PD nurse. Peritonitis was defined as cloudy effluent with at least 100 leukocytes/uL, of which more than 50% were polymorphonuclear cells, generally with abdominal pain and/or a positive effluent culture. Demographic characteristics of the PD cohort were analyzed using descriptive statistics. Infection rates among the study periods were presented as episodes per dialysis-year at risk and were analyzed using incident rate ratio analysis. Differences in the infection rates were significant at p ≤ 0.05. All analyses were conducted using STATA 9 (STATA Corp., College Station, TX, USA).
Results
There were a total of 444 prevalent PD patients with 799.26 dialysis-years at risk in our cohort from January 1, 1991, to December 31, 2000, and January 1, 2004, to December 31, 2013. Patient demographics are shown in Table 1. The 2 groups were similar, except there were relatively more African-American patients in the second period. Of the 444 total patients, 155 patients (34.9%) had peritonitis while 107 (24.1%) had exit-site infection.
Demographics of the Cohort of Peritoneal Dialysis Patients
SD = standard deviation.
At the start of dialysis.
Figure 1 shows the rate of infections as well as gentamicin resistance during the 2 periods. Gram-negative peritonitis rates were similar (0.098 and 0.127, p = 0.21). Both gram-positive exit-site infection and peritonitis rates were lower in Period 2 compared to Period 1 (0.093 vs 0.173, p = 0.0002, and 0.111 vs 0.274, p < 0.0001, respectively), likely ascribed to change in connectology. Total peritonitis rate was 0.425 in Period 1 and 0.268 in Period 2 (p = 0.002).
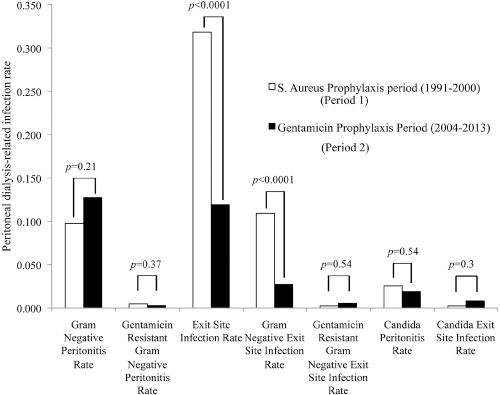
Peritoneal dialysis-related infection rate (as episodes per dialysis-year at risk) in 2 periods.
Both total and gram-negative exit-site infection rates were lower in Period 2 compared to Period 1 (0.318 vs 0.119, p < 0.0001, and 0.109 vs 0.027, p < 0.0001, respectively). Peritoneal dialysis-related candida infection was also low. There were 11 episodes of fungal peritonitis in Period 1 and 7 episodes in Period 2. The incidence of fungal exit-site infection was 1 in Period 1 and 3 in Period 2. Two episodes in Period 2 were in the same patient 1 year apart without associated fungal peritonitis or recurrence of PD-related fungal infection after the second episode. The rate of gentamicin resistance was also consistently low. Only 3 episodes in each period had PD-related infections with gentamicin-resistant gram-negative organisms (Table 2).
Gentamicin-Resistant Peritoneal Dialysis-Related Infection
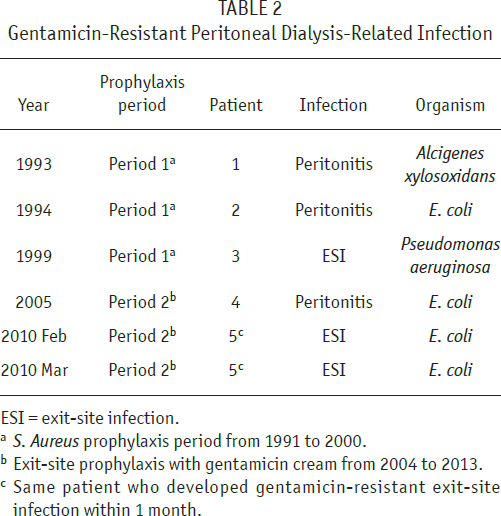
ESI = exit-site infection.
S. Aureus prophylaxis period from 1991 to 2000.
Exit-site prophylaxis with gentamicin cream from 2004 to 2013.
Same patient who developed gentamicin-resistant exit-site infection within 1 month.
Discussion
The International Society for Peritoneal Dialysis (ISPD) guidelines recommend using some type of antibiotic prophylaxis to prevent exit-site infection in PD patients (7,8). However, in some programs there is some reluctance to use an antibiotic such as gentamicin cream due to the fear that resistance will develop. We have shown in this study that after a decade of use of exit-site gentamicin in a PD program, gentamicin-resistant PD-related infections were infrequent and had not increased compared to the prior period.
The literature on this topic is sparse. In one report, 2 patients developed gentamicin-resistant exit-site infection after using gentamicin cream as prophylaxis (5). One of them had last applied gentamicin prophylaxis about 1 to 2 years before the development of the gentamicin-resistant exit-site infection episode, while the other was a nursing home patient with multiple prior episodes of PD-related infections. One of the exit-site infection episodes with Pseudomonas infection was treated with gentamicin cream (5). Another retrospective study described an increasing trend of gentamicin-resistant PD-related infections with the application of gentamicin cream (n = 101) compared to mupirocin (n = 120) but the difference was not statistically significant (6). In a third retrospective study, there was no significant increase in bacterial infections resistant to gentamicin after changing exit-site prophylaxis to gentamicin cream once a day (9). These results were similar to our study but with a shorter follow-up.
Another concern raised with the use of gentamicin for prophylaxis is a possible increased risk of PD-related candida infections. The literature related to that concern is also sparse. The study comparing gentamicin and mupirocin cream as exit-site prophylaxis showed an increased rate of fungal exit-site infection with gentamicin cream (p = 0.05) but no increase in candida peritonitis. These candida exit-site infections were readily treated with a course of antifungal agents (4). We showed that with a decade of use of gentamicin prophylaxis, PD-related fungal infections remained very low.
In this observational study covering an extensive period of time, gram-negative peritonitis rates were similar in the 2 periods of prophylaxis. In the randomized trial of gentamicin versus mupirocin cream applied to the exit site for prophylaxis to prevent exit-site infections, gram-negative peritonitis as well as overall exit-site infections were reduced significantly by the use of gentamicin cream at the exit site (4). The randomized trial was designed and powered to examine the difference in exit-site infections (particularly Pseudomonas exit-site infections) between the 2 arms of the study. Peritonitis was measured primarily for safety reasons and therefore the reduction in gram-negative peritonitis was an unexpected finding and required further study to support. In the present study, the likely absence of a reduction in gram-negative peritonitis despite a reduction in gram-negative exit-site infection may be because most of the gram-negative peritonitis was due to a pathway other than exit-site infection, such as an enteric source. An enteric source for gram-negative peritonitis would not be influenced by the type of antibiotic cream used at the exit site.
The weakness of the present study is that this was a longitudinal observational study from a single center. A strength is that the data were collected prospectively. Our cohort was larger and the duration of follow-up was longer than other studies in the literature. In addition, because this was a single-center study, the protocol was followed by all the physicians providing consistent care to the patients. One limitation is that data collected on infectious complications in the registry were restricted to PD-related infections such that resistance in organisms causing pneumonia, cellulitis, or other infections was not collected. However, we think the data on the PD-related infections are quite convincing in showing no increased risk of gentamicin resistance in PD-related infections, an important finding.
Footnotes
The authors have no financial conflicts of interest or grant support to declare. This research has not been previously published except in abstract form.