
Abstract
No clear consensus has been reached regarding the optimal time to remove the peritoneal dialysis catheter (PDC) after kidney transplantation (KT). This retrospective observational study, conducted in a single peritoneal dialysis (PD) unit including all PD patients who received a KT between 1995 - 2015, was undertaken to evaluate the clinical outcomes and potential complications associated with a PDC left in place after KT. Of the 132 PD patients who received a KT, 20 were excluded from the study. Of the remaining, 112 (85%) patients with functioning KT were discharged with their PDC left in place and had it removed in a mean interval of 5 ± 3 months after KT, after achieving optimal graft function. During this follow-up period, 7 patients (6%) developed exit-site infection and there were 2 cases (2%) of peritonitis; all of them were successfully treated. Delayed PDC removal after KT is associated with low complication rates, although regular examination is needed so that mild infections can be detected early and therapy promptly instituted.
Infections are a major concern in the post-transplant period and therefore this potential risk should be weighed against the possible need for dialysis support immediately after KT, especially in cases of delayed graft function (DGF) or primary graft non-function (PNF) (8–10).
Very few studies have reviewed the potential risks of a PDC left in place after KT in adult recipients (6,7), and thus we aimed to evaluate the outcomes and potential complications associated with the PDC in the post-transplant period.
Methods
This was a retrospective, observational study in a population cohort of adults on PD at Ramón y Cajal Hospital who underwent KT between May 1995 and July 2015. All patients had a double-cuff Tenckhoff catheter inserted by the standard technique. Demographic features and the following clinical parameters were included: age, gender, comorbidities, type of transplant, PD vintage, and previous history of catheter-related infection. A period of 4 weeks without peritonitis was necessary to receive a KT. Before transplantation, the peritoneal cavity was emptied, the catheter was flushed, and the system was left closed until catheter removal. Where dialysis support was required right after KT, patients were transferred to hemodialysis.
The removal of the PDC at the time of KT was only considered in cases of pre-existing exit-site and tunnel infection. In the rest of the cases, the PDC was left in situ and removed during the late post-transplant period after achieving stable allograft function, unless a significant catheter-related complication occurred in the meantime. After discharge from hospital, the PDC was neither used nor manipulated (flushed or heparinized) in order to avoid complications. Patients were instructed to perform their daily washing of the exit site using saline solution and sterile gauze pads. Exit sites were regularly inspected for signs of infection. Peritoneal dialysis catheter infections identified during the study period were treated with topical or intravenous antibiotics depending on the type of infection and according to antibiogram. The decision to remove the catheter depended on the degree of the infection and clinical course. Due to the retrospective study design, no informed consent was needed, although the study was conducted according to the Declaration of Helsinki.
Descriptive statistics are presented as mean and standard deviation, or median and interquartile range (IQR) for continuous variables, and absolute values and percentages for categorical variables. Statistical analyses were performed using IBM SPSS Statistics 21.0 (Armonk, NY, USA).
Results
One hundred and thirty-two patients were analyzed: 91 men and 41 women, with a mean age at the time of KT of 50 ± 13 years. The median time on PD was 27 months (range: 1 – 157 months). A flowchart of the patients included in the study is presented in Figure 1. Overall, 130 KT were from deceased donors, including 6 combined pancreas-kidney, and 2 were from living donors. Triple immunosuppressive therapy with prednisone, tacrolimus, and mycophenolate mofetil was the most frequent regimen. Only 7% received cyclosporine, and 9% mammalian target of rapamycin inhibitors (everolimus or sirolimus). Twenty patients were excluded from the study (Figure 1): 17 patients due to early removal of the PDC and 3 patients who had non-functioning KT and returned to PD, with no catheter-related infections were documented within 3 months after resuming PD. The remaining 112 (85%) patients with functioning KT were discharged with their PDC left in place and had it removed under local anesthesia in a mean interval of 5 ± 3 months after achieving optimal graft function (mean creatinine of 1.7 ± 0.7 mg/dL).
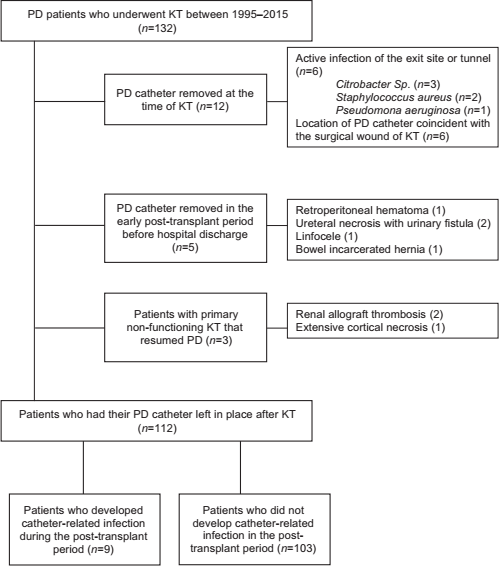
Flow chart of patients included in the study. PD = peritoneal dialysis; KT = kidney transplantation.
The main clinical characteristics of these patients are presented in Table 1. During the follow-up period, 9 patients (8%) developed a catheter-related infection while waiting for catheter removal. Previous history of exite-site infections or peritonitis was similar, but patients who developed catheter-related infections after KT had a higher previous incidence of infections caused by Staphylococcus aureus (44% vs 4%). In addition, the number of surgical complications was higher in the group of patients who eventually developed catheter-related infections (22% vs 3%). Overall, the main surgical complications were urinary fistula (3 cases), acute infarction of the lower pole of the renal allograft (1 case), and ureteric stenosis causing allograft hydronephrosis (1 case).
Demographic and Clinical Characteristics of Patients Discharged with PDC Left In Place after KT
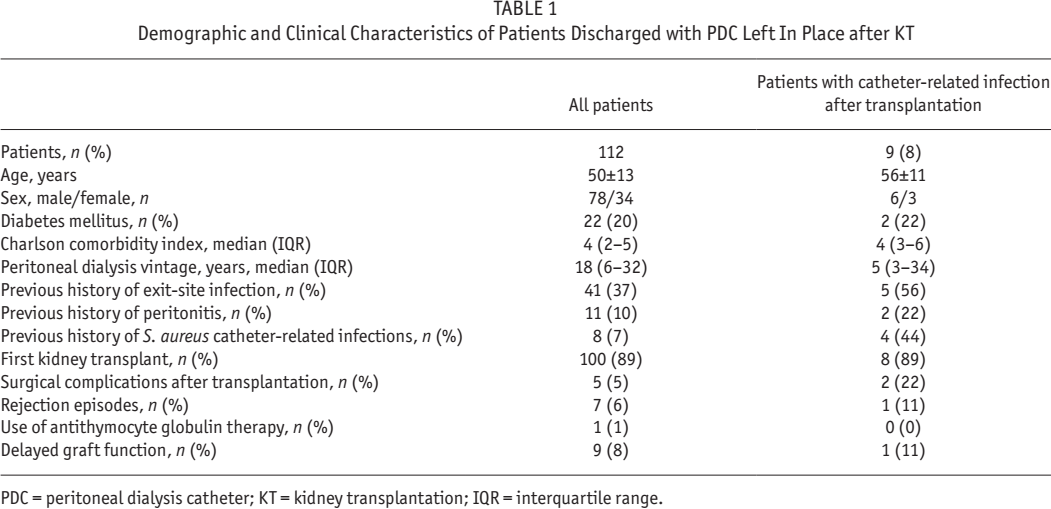
PDC = peritoneal dialysis catheter; KT = kidney transplantation; IQR = interquartile range.
Seven of the 9 patients (6%) developed exite-site infection, which resolved with antibiotic therapy except for 1 case, due Pseudomona aeruginosa, that required catheter removal without incident. The remaining 2 patients (2%) developed peritonitis in a mean time of 36 days after KT: in 1 case, the infection was due to S. epidermidis, and in the other, no causative microorganism could be identified. Both of these patients were treated with intraperitoneal antibiotic therapy. Of note, 56% of these infections were due to gram-positive bacteria, whereas gram-negative accounted for only one-third of the cases. None were due to methicillin-resistant S. aureus. No significant complications occurred after PD catheter removal, and the median length of hospital stay was 2 days.
Discussion
The results of this study reveal that late removal of the PDC after KT is associated with a low incidence of complications in adult patients treated with current immunosuppresants. Moreover, this study shows that PDC-related infections after KT are generally mild and can be successfully treated with antibiotics in most cases. The literature on this topic is scarce, mostly based on pediatric populations (3,12,13), and yet no randomized controlled trial has been conducted. However, this is still a matter of controversy, as different conclusions have been drawn in previous studies (3,7,13).
The low incidence of catheter-related infections in our study (only 1 episode every 56 months for patients at risk) compared with previous reports could be partly explained by the fact that we only included adult patients. It is well known that the frequency of infectious complications among children undergoing PD regularly exceeds that in adults. In addition, the PD system was not manipulated during the post-transplant period, patients were retrained in the proper maintenance and hygiene of the PDC, and exit sites were regularly inspected on each visit. This allowed early diagnosis and treatment of infections.
Bakir et al. found that more than 2 rejection episodes, PNF, and urinary leakage were significantly associated with peritonitis after KT (6). In contrast to this study, our patients received current standard immunosuppressive therapy and the number of rejection episodes was low. Therefore, patients were not exposed to strong immunosuppressive regimens, further reducing the chances of severe infections. One of the main concerns regarding the early removal of the PDC is delayed graft function or PNF, and the consequent need for dialysis. Although PD is feasible after KT, an increased risk of wound infection and leakage has been reported (6,7,11). Our center's policy is to avoid PD early after KT in order to decrease the risk of these complications, and whenever dialysis support is required, we place a central venous catheter (CVC), even though blood stream infections might also pose a threat.
The probability of delayed graft function is increased in grafts coming from deceased donors and especially from expanded criteria donors (14). In addition, since KT recipients are becoming progressively older, with greater comorbidity and prior allosensitization, the risk of PNF is sometimes higher (15 16-17). Therefore, we advocate for leaving the PDC in situ until stable graft function is achieved. In our opinion, resuming PD after hospital discharge in patients with PNF might be less traumatic than starting hemodialysis, and may also shorten hospitalization.
This study has several potential limitations. Firstly, due to the observational and retrospective nature of the study no causal relationship could be established. Secondly, the overall number of cases was small, follow-up time was short, and no control group was available for comparisons. Despite these limitations, this study gives a current view of a still controversial topic in the medical literature, providing additional evidence that the PDC can be left in situ a few months until stable graft function is achieved. In conclusion, late removal of the PDC after KT is associated with a low incidence of complications in adult patients when the PDC is not used. Nonetheless, infectious complications can occur, and therefore patients should be followed closely and should be properly instructed in their daily catheter care. Further prospective studies are warranted to better determine the optimal time to remove the PDC.
Footnotes
The authors have no financial conflicts of interest to declare.