
Abstract
Quality of life (QOL) is an important indicator of quality of healthcare. Measuring QOL and its correlates for peritoneal dialysis (PD) patients is important for public health policy, intervention, and clinical decision-making. Data from 62 patients treated at 6 dialysis centers were collected using short form (SF)-36. Multiple linear regression was used to assess the relationship between QOL and several covariates. Results indicated most patients were ≥ 60 years old (51.6%), retired (40.3%), diagnosed with end-stage renal disease (ESRD) > 1 year (82.3%), with diabetes as primary cause of ESRD (38.7%), and performing daily dialysis (77.4%). After adjustment of covariates, males (P = 19.03, p = 0.0001) scored on average 19.03 higher on QOL than females. Patients 41 - 60 years (P = 11.4, p = 0.018) scored on average 11.4 higher than those ≥ 60 years. Kuwaitis (P = -9.61, p = 0.057) scored on average 9.61 lower than non-Kuwaitis. Patients living with family/others (P = 13.02, p = 0.076) scored on average 13.02 higher than those living alone. Patients satisfied with their dialysis (P = 28.37, p = 0.001) scored on average 28.37 higher than non-satisfied patients. Performing dialysis at home (P = -15.52, p = 0.006) resulted in an average decrease of 15.52 in QOL compared with those in dialysis centers. Finally, patients with diabetes as the primary cause of ESRD (P = -9.8, p = 0.047) saw an average 9.8 decrease in QOL compared with patients with other ESRD causes. Gender, age, nationality, living status, satisfaction and place of dialysis, and causes of ESRD are independent predictors of QOL. Healthcare providers should pay more attention to females, those living alone, and those older than 60 years. Patients performing PD at home should have assistance from a nurse or health practitioner.
Quality of life (QOL) is a multi-dimensional concept that affects the performance of individuals in physical, psychological, and social aspects of their lives. It can be affected by cultural and economic factors and by spiritual beliefs (5). Measuring QOL is important for public health policy, evaluation, and clinical decision-making (5). Quality of life is also an important indicator of quality of healthcare (6). Diminished QOL for ESRD patients may negatively affect their social and psychological wellbeing, and even their mental status. Therefore, it is important to identify factors that may influence QOL among peritoneal dialysis (PD) patients (7). Our goal was to investigate associations between QOL and some covariates regarding PD patients in Kuwait.
Materials and Methods
Study Design and Data Collection
A cross-sectional design with a non-probabilistic sample (N = 62) was implemented. Patients on PD for more than 3 months, with no cerebral-vascular disease or serious mental impairment, and over 21 years of age were included. To reduce recall bias, patients not oriented to time, place, and person were excluded. Acute cases suffering from infection, cerebral-vascular diseases, acute coronary syndrome, or malignancy 4 weeks prior to data collection were excluded. Informed consent was approved and obtained from all subjects.
The self-administered short-form (SF-36) questionnaire used in the US Medical Outcomes Study (8) was used for data collection. Its English version was translated into Arabic and back translated into English by 2 independent individuals. It consists of 36 items measuring physical and mental health status in relation to 8 health domains. Each domain is scored from 0 to 100. Higher scores indicate better QOL according to the US Medical Outcomes Study (8). R statistical software was used for data analysis (https://www.R-project.org/). All tests were 2-tailed, and a p value < 0.05 was considered significant.
Results
Patients’ mean (standard deviation [SD]) age was 58.4 (15.4) years. Patients’ socio-demographic and disease profile characteristics are presented in Table 1. The QOL mean score was right-skewed. Patients with a higher median QOL were: males, Kuwaitis, married, with a university degree or higher, retired, with income > 1,000 KD, 41 – 60 years old, diagnosed with ESRD < 1 year, with causes of ESRD being hypertension/other, and on dialysis for 6 – 12 months. Results showed gender, age, marital and employment status, satisfaction with dialysis, and time on dialysis significantly associated with QOL.
Socio-Demographic and Disease Profile Characteristics of PD Patients in Kuwait (N=62)
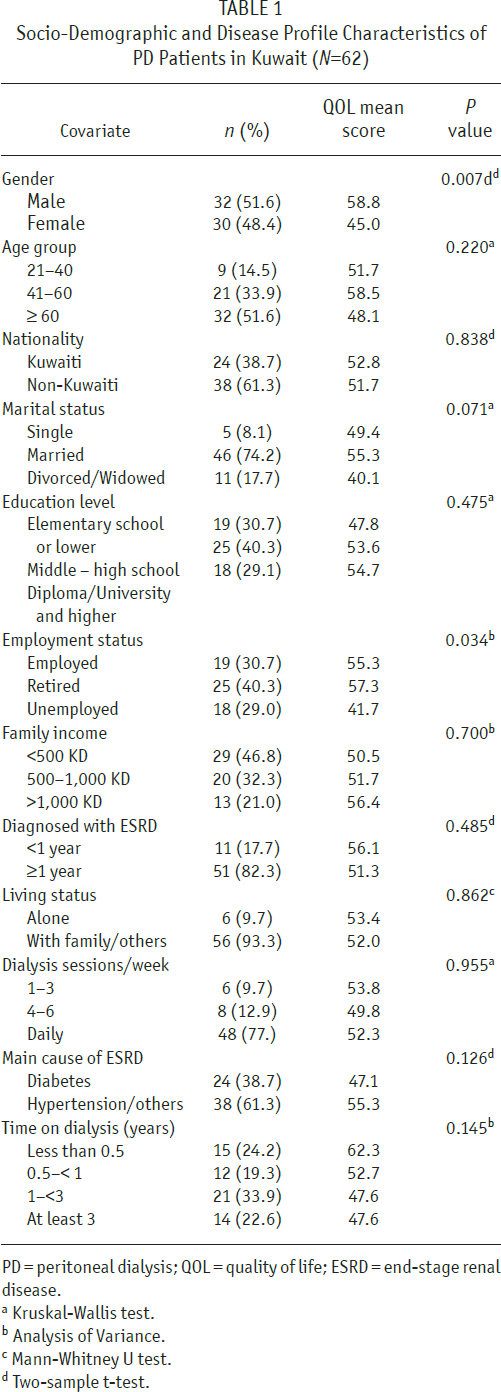
PD = peritoneal dialysis; QOL = quality of life; ESRD = end-stage renal disease.
Kruskal-Wallis test.
Analysis of Variance.
Mann-Whitney U test.
Two-sample t-test.
The regression model that predicts QOL, taking into account all variables, is presented in Table 2. Gender, age, nationality, living status, satisfaction with dialysis, place of dialysis, and causes of ESRD were significantly associated with QOL. After adjusting for other covariates, males scored on average 19.03 higher than females. Patients 41 – 60 years scored on average 11.40 higher than those ≥ 60 years. Kuwaitis scored on average 9.61 lower than non-Kuwaitis. Patients living with family/others scored on average 13.02 higher than those living alone. Patients satisfied with their dialysis scored higher than unsatisfied patients. Patients performing dialysis at home score on average 15.52 lower than those at the dialysis centers. Patients with diabetes as the primary cause of ESRD scored on average 9.8 lower than those with other causes of ESRD. All model diagnostics indicated good model fit.
Multiple Linear Regression Estimates Using Forward Selection of QOL for PD Patients in Kuwait (N=62)
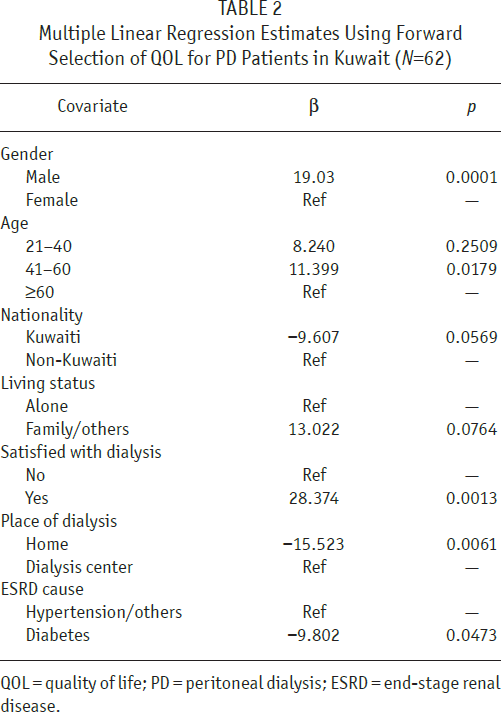
QOL = quality of life; PD = peritoneal dialysis; ESRD = end-stage renal disease.
Discussion and Conclusions
Gender, age, nationality, living status, satisfaction with dialysis, place of dialysis, and cause of ESRD are independent predictors of QOL. Males tend to have higher QOL. This is consistent with previous studies (4,9). Patients 41 – 60 years have the highest QOL. It may be due to the higher expectation of young patients and the low social interaction of older patients due to worse physical status. The middle-aged group, with a mature mind and well-developed social network, may adapt better to PD. However, Kuwaiti patients who should have more social connections and sense of affiliation than expatriates have a lower QOL. Reasons behind this association deserve further exploration.
Patients with ESRD caused by diabetes tend to have lower QOL than non-diabetic patients. This may be due to high comorbidities in diabetic patients. Patients who have dialysis at the dialysis center and are satisfied with the treatment are more likely to have better QOL. A limitation of this study is that clinical characteristics and comorbidities were not included, which could be important predictors of QOL.
Footnotes
The authors have no financial conflicts of interest to declare.