
Abstract
Background
Peritoneal dialysis (PD) is a home-based therapy where nurses train patients in its use. There has been no published randomized controlled trial (RCT) evaluating any specific protocol for nurses delivering PD training. A standardized education package based upon the best available evidence and utilizing modern educational practices may lead to improved patient outcomes. The aim is to develop a standardized, evidence-based curriculum for PD trainers and patients aligned with guidelines from the International Society for Peritoneal Dialysis (ISPD), using best practice pedagogy.
Methods
A literature search and clinical audit were conducted to identify current practice patterns and best practice. Results were reviewed by a focus group of practitioners comprising PD nurses, nephrologists, consumers, a medical education expert, and an eLearning expert. From this, a training curriculum and modules were developed.
Results
A comprehensive PD training curriculum has been developed, which includes modules for training PD nurses (trainers) and patient training manuals. The package comprises 2 introductory modules and 2 clinical case modules. The curriculum is designed for both interactive digital media (trainers) and traditional paper-based teaching with practical demonstrations (patients). Assessment is also addressed.
Conclusion
The need for the development of a comprehensive and standardized curriculum for PD nurse trainers and their patients was confirmed. This paper outlines the process of the development of this curriculum. Pilot testing of the modules was launched in late 2017 to examine feasibility, and planning has commenced for a RCT in 2019 to investigate the effect of the modules on clinical outcomes, and their wider application across Australia and New Zealand.
One of the reasons for low utilization of PD is the potential for complications, such as peritonitis, which directly contributed to 65% of PD technique failures and 7% of deaths in 2016 (7). Peritonitis has been associated with an increased risk of mortality up to 6 months after an episode of peritonitis (8). In Australia, the PD peritonitis rate has been found to be unacceptably higher than in many other countries (9). There has been some improvement over the past few years, although rates have now plateaued (10), and a tenfold variation in rates of peritonitis across PD units remains (11). A plausible explanation for such variance may include differences in clinical practices and training.
In light of this, the Nursing Liaison Committee of the International Society for Peritoneal Dialysis (ISPD) has recommended standardization of teaching practices for PD patients and their caregivers (12). Training guidelines, a PD patient training curriculum (13), a review reference, and an online education portal (14) were produced. The syllabus was published in 2016, but is yet to be evaluated (15). A review of 14 PD courses in 10 countries demonstrated large variability between units in training practices and duration of training. In Australia, a survey of PD units on their training practices revealed a large variation in delivery of PD training and competency assessments to meet educational standards recommended by the ISPD (16).
There is a need to develop a curriculum that ensures key learning outcomes in PD are achieved. A formalized PD education program has been shown to significantly reduce peritonitis rates in a retrospective single-arm intervention study involving 31 PD patients at a single center in Uruguay (17). However, an optimal education package has yet to be produced. It is likely that there are unrealized gains to be made for clinical outcomes in PD (18,19). The aim of this paper is to describe the development of the intervention, a standardized, evidence-based educational curriculum for PD nurse trainers and PD patients consistent with ISPD guidelines that will be used as part of a randomized controlled trial (RCT) to test its effectiveness and cost-effectiveness. Use of best practice to reduce the rate of PD-related infections and technique failure, was the underlying goal to keep patients safe, preventing complications, especially PD-related infections and technique failure, and supporting self-management.
Methods
In 2014, a learning needs analysis was undertaken by members of the HOME Network (THN) as part of the annual task-force prioritization. The development of a “Train the Trainer” program for PD nurses to support nurses to gain knowledge, skills, and experience as competent PD trainers was subsequently endorsed. The HOME Network (20) was established in 2010 as an Australian initiative to bring together healthcare professionals in the field of home dialysis with the aims of identifying and addressing the barriers to optimal utilization of home dialysis in Australia. The members include senior dialysis nurses, dietitians, and social workers. The Delphi technique (21) was used in the development of the “Train the Trainer” curriculum and its supporting material. The Delphi technique is an iterative process to collate and refine expert opinions, thus to obtain group consensus. It has been used widely in nursing research and has been useful in educational curriculum development (21,22).
A purposive sample of senior dialysis nurses (subject matters expert) and allied health staff from THN (n = 18) participated in the development of the content of the curriculum. The first face-to-face workshop with the 18 subject matter experts was conducted. The aims and objectives for the study and the activities for the workshop were explained prior to the brainstorming sessions. The 18 healthcare professionals were randomly subdivided into 3 groups of 6 members each. The idea of smaller groups maximized the contribution from each participant in a non-threatening and informal manner. The first task each group was requested to complete was to list headings or categories of a successful training curriculum for PD trainers. After the first exercise, each group was required to identify elements for each category. They were given 45 minutes to complete the brainstorming session and score the elements of importance. They were then invited to a plenary session for the final half hour to incorporate all information into a single list. The entire meeting lasted 2 1/2 hours and defined the elements for the potential curriculum. The same methodology was used for the development of the patient training manual. At the end of the first workshop, the group identified and developed the first draft set composition for the curriculum (Table 1).
First Draft Set Composition for the Curriculum
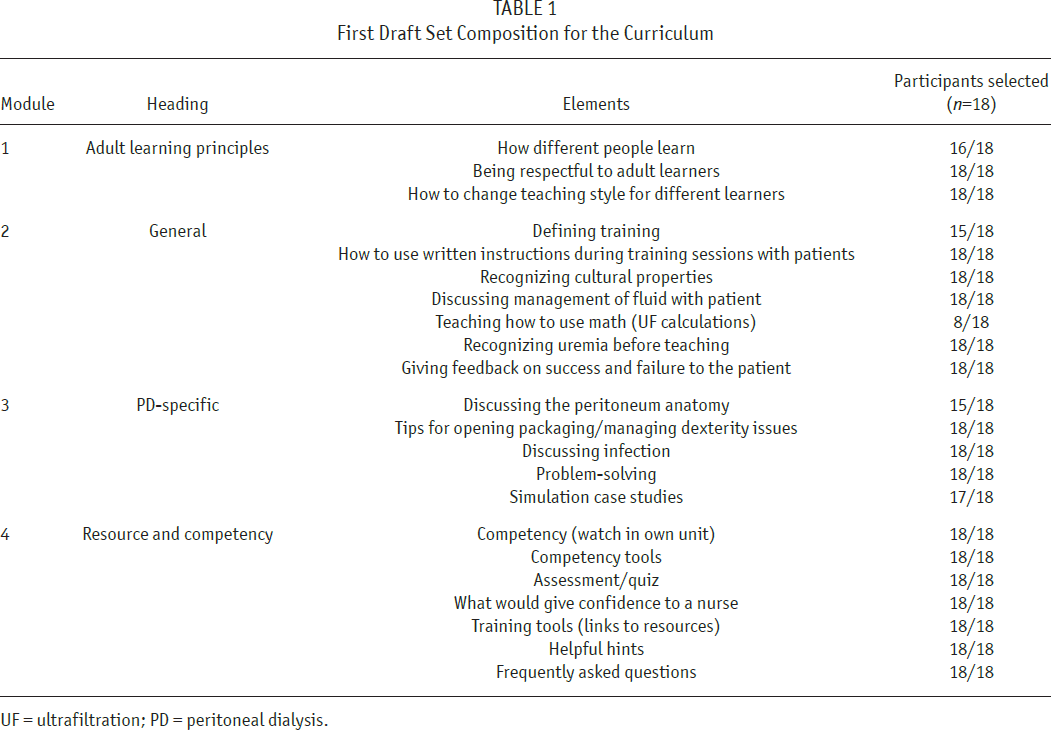
UF = ultrafiltration; PD = peritoneal dialysis.
A series of face-to-face workshops complemented by weekly teleconference calls over 18 months were conducted to develop and review the content of the curriculum and the modules. The investigator facilitated the workshops and teleconference calls. Revised versions of the curriculum and modules were provided to the participants prior to each engagement. The participants were required to identify any deficits and recommendations for improvement. Questions and/or items were discussed among the group. Debate and justification for certain items, with evidence and rationales, were included. The investigator recorded all information and discussion.
Based on the results of the analysis, consultation with the addition of 10 nursing staff from 4 PD units, 2 clinical service leads, and 2 renal consultants established further structured content development. A literature search supported by a clinical audit of Australian PD units (16) was conducted to identify practices and teaching content currently in use.
The training curriculum and modules developed were then further refined by THN, senior medical clinicians from the Australasian Kidney Trials Network (AKTN; an international collaborative research group with extensive experience in investigator-initiated clinical trials), medical educators and eLearning experts. Consumer engagement and input was sought extensively through consultation with PD patients by members of THN. Curriculum content was consistent with ISPD guidelines (15), with teaching based on adult learning principles (13–15), and best practice eLearning techniques. Competency-based assessment was also required to evaluate learning and confirm trainers’ skills. This study was approved by the Human Research Ethics Committee prior to the commencement of the study procedures and activities.
Results
A comprehensive PD nurse training curriculum, the “Train the Trainer” program, was developed in an interactive electronic format which included 2 introductory modules and 2 clinical case modules. It is designed for use in the PD unit setting to ensure adequate supervision. The document catered for a continuum of PD training experience and was a complete framework across a range of PD training expertise from beginner through to proficient. It is assumed that the trainers would be registered nurses with varying levels of expertise (Table 2), but also that these trainers may not have had any formal education on how best to teach patients.
Categories of Trainers According to Their Expertise
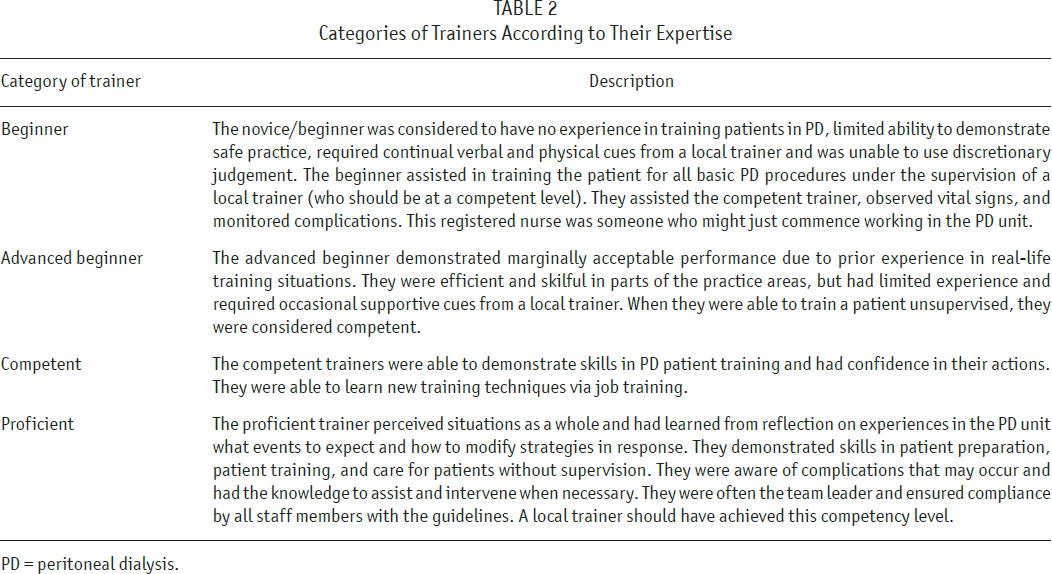
PD = peritoneal dialysis.
The Curriculum
The goal as a trainer is to enable patients to competently manage their own dialysis needs safely at home, preventing complications, especially PD-related infections and technique failure, and supporting self-management. The “Train the Trainer” curriculum included 2 introductory modules and 2 clinical case modules (Figure 1) available in electronic format. They are designed to be used by registered nurses only, while understanding that some countries, such as the United Kingdom, employ non-registered nurses to teach patients on PD. The first 2 modules considered the principles of home PD training, including an overview of clinical practice and the learning process, as it applies to personalized home training. The remaining 2 modules comprised clinical case studies with scenarios and issues that may be encountered during PD training. The program was supported by 2 patient training manuals. The training modules will address PD training for patients whose primary language is not English, and an assessment tool is incorporated for the trainers to assess the patient's level of health literacy before starting PD training, along with dexterity, vision, and other potential barriers to learning.
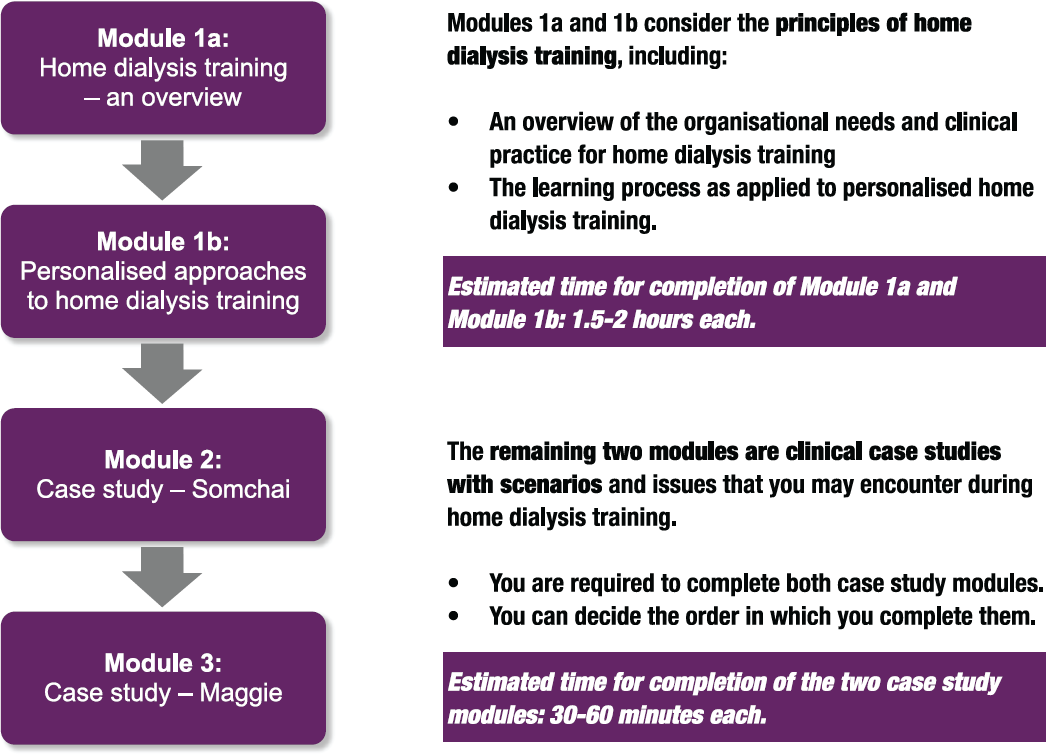
Outline of the trainer modules.
All electronic modules in the program applied a conversational approach, modelling the patient-to-trainer (or learner-to-teacher) feedback cycle consistent with optimal learning processes (23). In the modules, trainers were asked to answer a question or predict an outcome on the basis of their existing experience or knowledge before seeing the solution and its rationale. This encouraged them to reflect upon their own life and clinical experiences and build on prior knowledge, given additional information. Answers were used for feedback on learning but were not assessable.
Audio insights were embedded throughout each module to operationalize the conversational approach. Insights sharing real-world experience were presented by experts in the field and helped to extend on-screen information. Finally, the trainers were encouraged to keep a learning journal to document and reflect on their learning experiences (23) as they progressed through the modules. This may have been hard copy or electronic and included notes of any particular points or resources of interest, reflections on experiences, responses to activities, and questions for their mentor/ accredited assessor.
Assessment Methods
Competency assessment focused on performance in caring for and teaching a PD patient. It included assessing learning about how to teach patients, adequacy of documentation, and integration of knowledge through skills, using established standards of care, policies, and procedures. Trainers needed to identify a mentor/accredited assessor from their PD unit to assess their competencies as part of the requirement for the program. In addition, an understanding of all clinical content areas (i.e., theory-based and practical knowledge), covered by the PD Patient Training Manual had to be demonstrated.
Assessments included multiple-choice quizzes covering progressive knowledge and learning processes; written reflection, for example, on complications, and what could be done differently to prevent them; analysis of clinical case studies; and practice competency.
The Training Framework for the trainers (Figure 2) and patients (Figure 3) was thus developed. These frameworks were designed to outline the guiding principles and key structural elements of the curriculum. For the trainers, they were required to complete a prerequisite clinical knowledge online multiple-choice assessment in addition to a practical assessment prior to the commencement of the modules. There were online multiple-choice assessments at the end of each module with digital certificates of completion. The trainers were required to complete case study assessments and assess which patient factors and barriers impacted on PD training. Finally, the trainers prepared a personalized lesson plan for a specific PD training step.
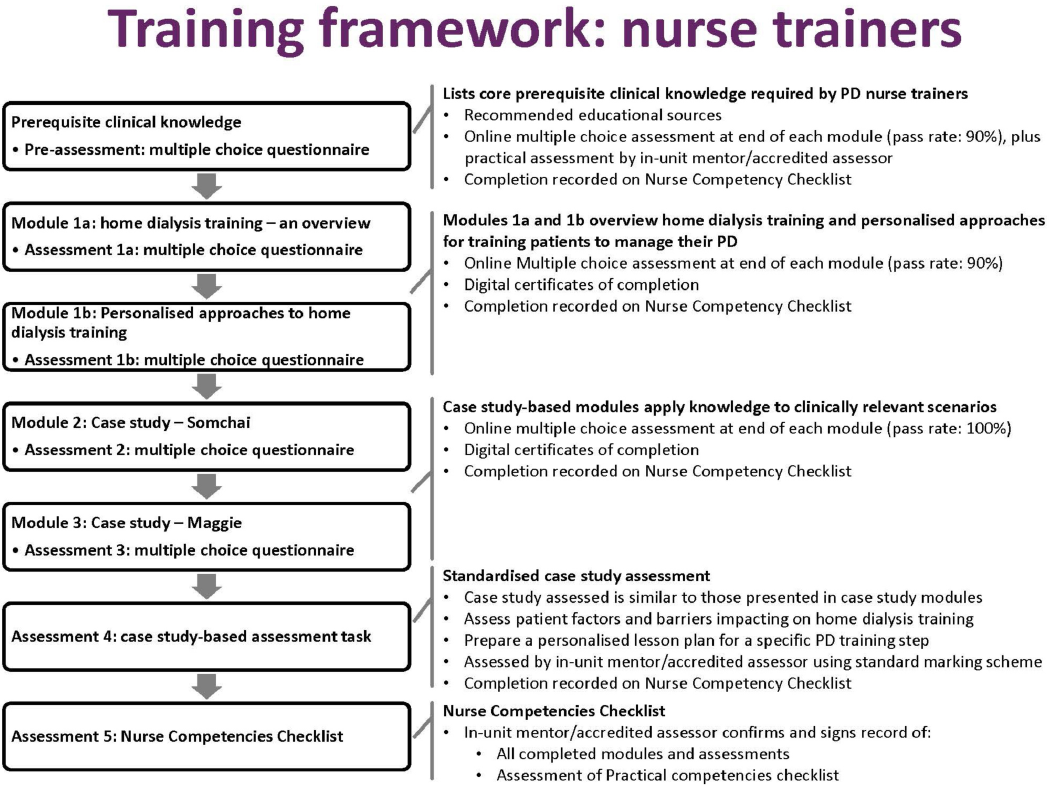
Training framework for PD nurse trainers. PD = peritoneal dialysis.
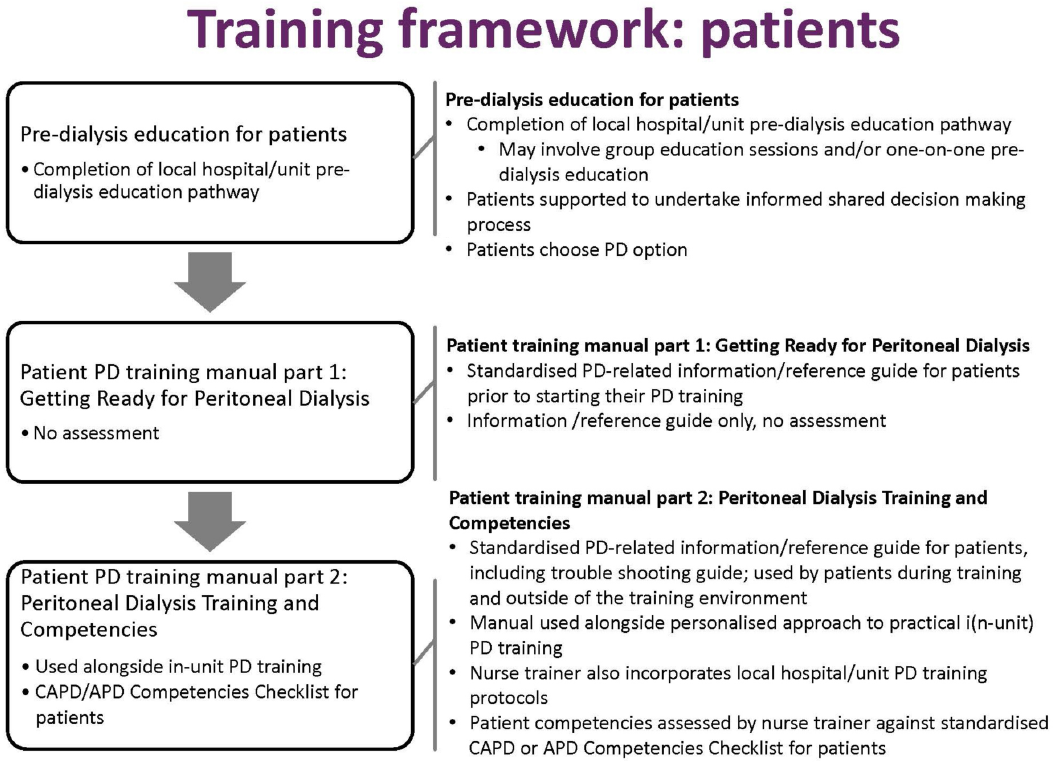
Training Framework for PD Patients. PD = peritoneal dialysis; CAPD = continuous ambulatory PD; APD = automated PD.
Patient Training Manuals
A traditional paper-based version of the Patient Training Manuals with practical demonstrations was available. Assessment was also addressed. Patients were required to follow their hospital's predialysis education pathway, which may have involved group education sessions and/or one-on-one predialysis education. Once the decision to transition into PD was made by the patient, they were provided with “Patient Training Manual 1: Getting Ready for Peritoneal Dialysis,” which had been designed to provide the patient with information that facilitated this transition. On commencing PD training, the patients were provided with “PD Training Manual 2: Peritoneal Dialysis Training and Competencies,” which had been designed to provide the patient with information and knowledge that allowed the patient to move into PD training and prepared them to go home safely on PD. It included an overview of PD, how to perform a PD exchange safely, and how to troubleshoot. The trainers assessed the patients’ competencies against a standardized PD Competencies Checklist for patients. The readability of the Patient Training Manuals was determined by the use of the Flesch Reading Ease score and the Flesch-Kincaid Grade Level (FKGL) (24,25). The Flesch Reading Ease score and the FKGL were selected because both are commonly used and are suitable to assess the readability of patient educational material and health information. These readability tools have been previously validated. The recommended reading grade level of health information for patients is 8 on the FKGL (26). The Flesch Reading Ease Score for the Patient Training Manual was 63.6 and the FKGL was 8. This paper is the first step toward the implementation of the designed intervention.
Discussion
The development of a standardized, evidence-based curriculum for PD trainers and patients aligned with ISPD guidelines used best practice pedagogy and included a large number of multidisciplinary stakeholders from different backgrounds. This provided fundamental and critical elements to ensure the quality and relevance of the curriculum, online modules, and training manuals. The patient training manuals were also reviewed by a number of PD patients periodically throughout the development. This active involvement of consumers in the development of the TEACH-PD curriculum was integral to its success.
In order to cater to a range of learning styles and settings as recommended by the ISPD (15), the patient training manuals need to be converted to digital format and evaluated. This will provide patients with flexibility in terms of their approach to learning, and bring the patient modules in line with the train-the-trainer (nurse) modules. It will improve the understanding/treatment of the dialysis disease burden and also provide an opportunity for PD patients to be engaged in the development and evaluation of the digital format of the patient training manual.
A number of anticipated barriers to completion of the training modules, such as competing workloads, can affect commitment to training (27). It is therefore important that PD units provide trainers with time release from their usual work activities in order to complete the program. However, even when time is allocated, there is a need to identify ways of addressing departmental cultures. This program requires trainees to be supported by a departmental mentor (28) to help overcome any resistance to change. Development of communities of practice should also be promoted so that newly trained staff are not isolated (29). Bringing trainers from different PD units together to identify effective practices (30) has also been found to change departmental cultures.
The developed curriculum and modules will undergo an interventional study titled: “A Targeted Education ApproaCH to improve Peritoneal Dialysis Outcomes (TEACH-PD Trial)” and this paper is the first step to developing the intervention. A TEACH-PD pilot study is underway to support the development of the TEACH-PD curriculum. The primary objective of this pilot study is to evaluate and further refine the TEACH-PD training tools and collect data that will assist in the planning of the larger implementation trial. The TEACH-PD pilot study will identify the gaps and barriers to the curriculum and its implementation. This is vital for the integrity, feasibility, and applicability of the curriculum.
After completion of the pilot study and review, planning will commence for a RCT to begin in 2019 across all PD units in Australia and New Zealand to investigate the effect of the comprehensive training curriculum on clinical outcomes. The program can then be used to develop standard operating procedures for training modules, which will provide opportunities for building an evidence base for future research and improve external validity.
Conclusion
There have been no published RCT data evaluating any specific protocol for training PD nurse trainers. It is highly likely that there are unrealized gains to be made for PD clinical outcomes with the adoption of best practice guidelines. A comprehensive PD training curriculum has been developed by experts, utilizing adult learning principles and eLearning techniques, following the guidelines outlined by the ISPD. This curriculum includes an interactive electronic format for training PD staff and paper-based training manuals for patients. The long-term plan for the pilot study and subsequent RCT is to introduce the program to all PD units in Australia and New Zealand, translating current evidence into clinical practice.
Footnotes
Acknowledgments
Funding was received from the following organizations to support the Train the Trainer modules development: Baxter Healthcare Competitor Educational Grant; Kidney Health Australia Enabling Grant: BEAT-CKD Program Grant; Western Australia Health; and New South Wales Health. DJ is supported by an Australian National Health and Medical Research Council Practitioner Fellowship. GZS's contribution was supported by funding from a National Health and Medical Research Council (NHMRC) – Australian Research Council (ARC) Dementia Research Development Fellowship (#1102532). YC is supported by an Australian National Health and Medical Research Council Early Career Fellowship.
JC has previously received speaker's honoraria and research funds from Baxter Healthcare, Fresenius Medical Care, Roche Pharmaceuticals and Amgen. DJ has previously received consultancy fees, research funds, travel sponsorships and speakers’ honoraria from Baxter Healthcare and Fresenius Medical Care. YC has previously received research funds from Baxter Healthcare and Fresenius Medical Care. As a medical research institute, NICM receives research grants and donations from foundations, universities, government agencies, individuals, and industry. Sponsors and donors provide untied funding for work to advance the vision and mission of the Institute. The project that is the subject of this article was not undertaken as part of a contractual relationship with any organization other than the funding declared. NB has received speaker's honoraria, advisory board honoraria, travel grants, and unrestricted educational grants from Roche Pharmaceuticals, Astra Zenaca, and Amgen. AF has received speaker's honoraria and research funds from Baxter Healthcare.