
Abstract
Background
Automated peritoneal dialysis (APD) is a growing PD modality but as with other home dialysis methods, the lack of monitoring of patients’ adherence to prescriptions is a limitation with potential negative impact on clinical outcome parameters. Remote patient monitoring (RPM) allowing the clinical team to have access to dialysis data and adjust the treatment may overcome this limitation. The present study sought to determine clinical outcomes associated with RPM use in incident patients on APD therapy.
Methods
A retrospective cohort study included 360 patients with a mean age of 57 years (diabetes 42.5%) initiating APD between 1 October 2016 and 30 June 2017 in 28 Baxter Renal Care Services (BRCS) units in Colombia. An RPM program was used in 65 (18%) of the patients (APD-RPM cohort), and 295 (82%) were treated with APD without RPM. Hospitalizations and hospital days were recorded over 1 year. Propensity score matching 1:1, yielding 63 individuals in each group, was used to evaluate the association of RPM exposure with numbers of hospitalizations and hospital days.
Results
After propensity score matching, APD therapy with RPM (n = 63) compared with APD-without RPM (n = 63) was associated with significant reductions in hospitalization rate (0.36 fewer hospitalizations per patient-year; incidence rate ratio [IRR] of 0.61 [95% confidence interval (CI) 0.39 – 0.95]; p = 0.029) and hospitalization days (6.57 fewer days per patient-year; IRR 0.46 [95% CI 0.23 – 0.92]; p = 0.028).
Conclusions
The use of RPM in APD patients is associated with lower hospitalization rates and fewer hospitalization days; RPM could constitute a tool for improvement of APD therapy.
One of the drawbacks of any home-based dialysis treatment is the potential risk that patients, without the frequent monitoring that is readily available during in-center dialysis, may receive inadequate treatment. Low adherence to therapy prescriptions was noted by Bernardini et al. who reported that 30% of their PD patients did not comply with prescriptions (5); failure to do so can be associated with adverse outcomes (5). Ideally, if PD patients’ home treatments could be monitored on a daily basis, this would make it feasible to detect problems early and to correct inadequate dialysis delivery. Technological solutions for remote monitoring of home-based APD treatments are now available; such programs make it possible for the clinical team to become aware of many aspects of the therapy at the patient's home in real time. Based on information obtained by remote monitoring, the clinical team may provide advice and propose interventions that allow the patients to deliver a safer and better-quality treatment (6). Besides the above, the new process of remote monitoring could confer increased confidence and satisfaction with care from the patient's perspective because of the perception of being more closely monitored and adequately supported (7). Therefore, remote patient monitoring (RPM) in APD has the potential to improve therapy outcomes and confer economic advantages (8).
A RPM device that allows remote management of the APD treatment performed in the patient's home was released to the market in May 2015 (HomeChoice Claria with the platform Sharesource; Baxter Healthcare Corporation, Deerfield, Il, USA) (9). The RPM device allows the clinical team to securely review the patient's treatment data that are automatically collected after each PD session and provides the ability to adjust APD prescriptions online.
The Baxter Renal Care Services Colombia (BRCS) PD model was recently described (10). The program is based on a patient's regular monthly comprehensive evaluation and additional on-site visit for preemptive consultations and a continuous quality improvement (CQI) approach to the delivery of care. The APD treatments were performed following individualized needs per patient to achieve adequacy goals including daily sessions, using glucose-based solutions. The RPM program was recently introduced in the BRCS Colombia network and followed by specific training for healthcare professionals, monthly tracking of key performance indicators (KPI) by center, and the development of quality improvement plans (9).
Although the potential benefits of RPM are widely recognized and appreciated (8), there is a lack of studies providing evidence on the association between the use of RPM in an established PD practice and improved outcomes of APD therapy. The objective of the current study was to evaluate the association between RPM use and clinical outcomes (hospitalizations and hospital days).
Methods
Type of Study
A retrospective cohort study was conducted in 28 BRCS units located in 6 cities in Colombia to determine whether use of RPM in incident patients on APD therapy was associated with an improvement in clinical outcomes. The study was approved and monitored by an ethics research committee of Foundation Cardio-Infantil (minutes number 25-2018 of 1 August 2018).
Study Population
Patients were selected at all BRCS units located in cities where RPM was introduced. Eligibility criteria included the following: 1) both genders, age 18 years or older; 2) diagnosis of ESRD; 3) being an incident patient on home-based APD therapy (defined as undergoing the first 90 days of APD therapy); and 4) initiation of APD between 1 October 2016 and 30 June 2017. Exclusion criteria were: 1) pregnancy; 2) life expectancy of less than 6 months; and 3) ESRD comorbidity index (ESRD-CI) > 8 (11). The patients were divided into 2 cohorts based on the RPM use: 1) APD-RPM cohort: patients using the HomeChoice Claria device with Sharesource technology and 2) APD-without RPM cohort: patients using APD systems HomeChoice Legacy without RPM. The RPM program started when the incident patients initiated APD. Patients completed at least 12 months of follow-up. During the follow-up, patients were censured for all drop-out events.
Remote Patient Monitoring Program
The RPM program was implemented with a staffing ratio of 1 nurse per 50 PD patients. The mean daily time invested by the nurse reviewing the Sharesource platform was approximately 30 minutes per 25 patients (9). An alarm code was developed and guided the team for direct clinical intervention if the patient missed a treatment, lost connectivity, or had 3 “yellow flags” or 1 “red flag,” i.e., symbols that signaled the occurrence of any form of deviation in the delivery of therapy (9). The platform was reviewed on a daily basis by PD nurses, who checked the ultrafiltration profile, initial drainage, blood pressure, body weight, and the source of any alarm, while the entire clinic team performed a comprehensive evaluation of the information on a weekly basis (9). The employment of the RPM device was assigned to consecutive patients according to the (limited) availability of the device in the BRCS clinics; there was no specific clinical criterion for the allocation of a patients to the RPM program.
Variables
The primary outcomes were numbers of hospitalizations per patient-year and hospital days. The latter was defined as the time in days from hospital admission to discharge, per patient-year. All outcome variables were registered up to 365 days after the start of APD therapy.
The exposure variable of interest was APD with or without RPM. The following variables were used to control for possible confounding factors: 1) sociodemographic variables: age, gender, educational level, and city of residence; and 2) clinical characteristics at the beginning of the APD: cause of chronic kidney disease (CKD), ESRD-CI, hemoglobin, phosphorus, and albumin.
Statistical Analysis
Socio-demographic and clinical characteristics of all patients were summarized descriptively by treatment cohort (i.e. APD with or without RPM). Subsequently, differences between cohorts in the distribution of variables that could serve as confounders were assessed, according to the type of distribution found and using standardized differences.
To evaluate the association between RPM exposure and clinical outcomes, matching methods were used to compensate for the lack of randomization (confounding and selection bias) and to obtain unbiased estimators (12–14). Propensity score matching was used to evaluate the association of RPM exposure with numbers of hospitalizations and hospital days. The propensity score for each subject was calculated from a logistic regression model that included all clinical and demographic variables as predictors of the exposure status. The logistic regression model included possible confounding factors, as well as the characteristics that presented statistical differences in the descriptive analysis. A 1:1 matching without replacement utilizing the nearest neighbor within caliper was utilized to match each APD-RPM subject with an APD-without RPM subject. All APD-RPM cases were then randomly ordered and an APD without RPM case with a propensity score closest to the first treatment case was selected. Different calipers (0.025, 0.045) were used, and the one that produced a better balance (0.045) between the baseline variables was selected. The balance between exposed and unexposed groups in the matched sample was evaluated based on standardized differences, with a target value of < 0.1 (13). Additionally, all categorical variables were compared with Pearson's χ2 test and continuous variables were analyzed with paired t-test. The association of RPM exposure on the count of hospitalization events (and days of stay) per year of patient follow-up was estimated with incidence rate ratio (IRR) from negative binomial regressions. According to a recommendation by Weaver et al. (15), the count model (i.e. negative binomial) with the best performance was selected using both the Akaike's information criterion (AIC) and Bayesian information criterion (BIC); 95% confidence intervals (CI) were estimated based on robust standard errors. See Supplemental Table 1. Stata Statistical Software: Release 14 (StataCorp LP, College Station, TX, USA) was used to perform statistical data analysis.
Baseline Characteristics of Full Study Population According to Exposure Status
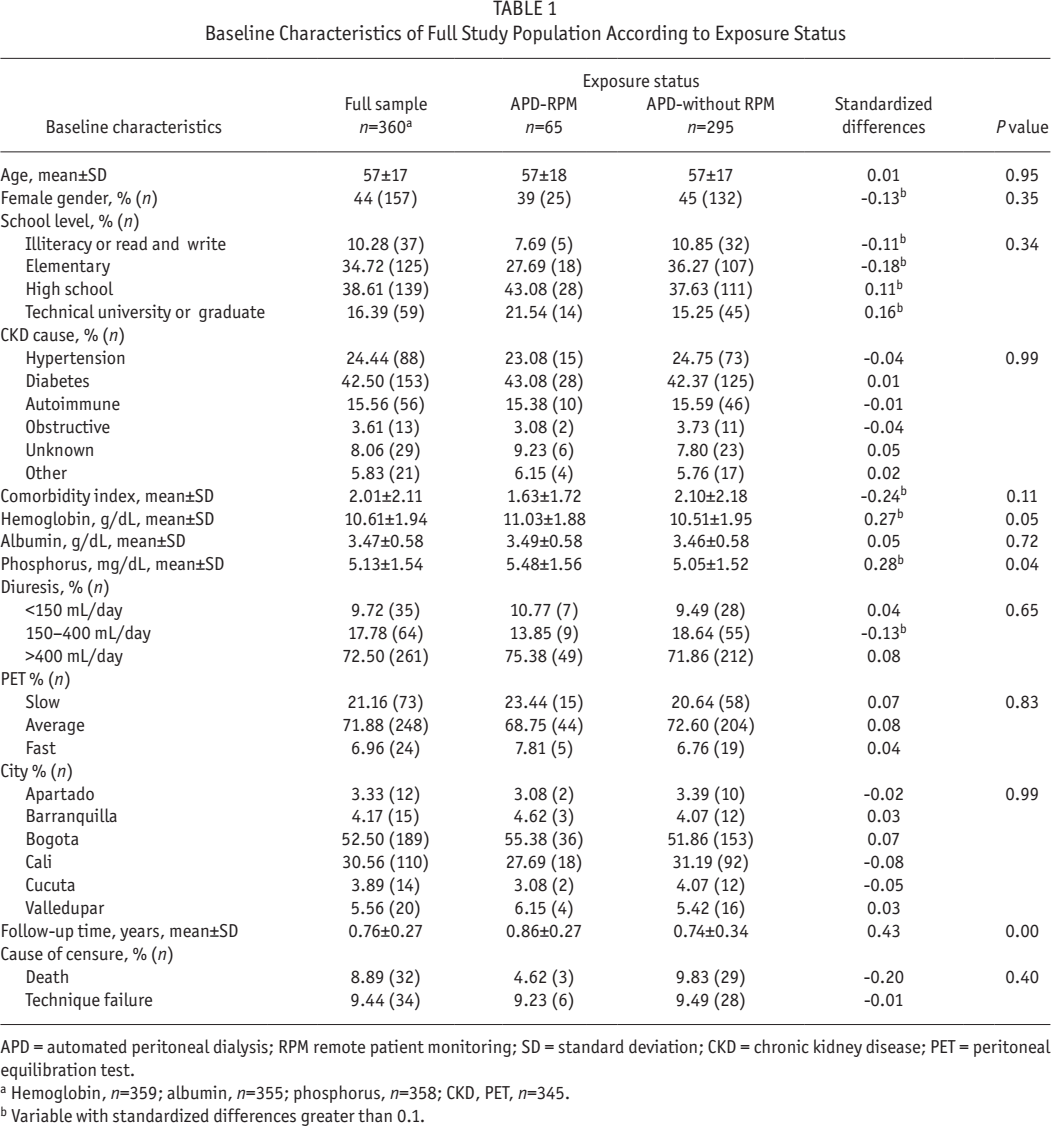
APD = automated peritoneal dialysis; RPM remote patient monitoring; SD = standard deviation; CKD = chronic kidney disease; PET = peritoneal equilibration test.
Hemoglobin, n=359; albumin, n=355; phosphorus, n=358; CKD, PET, n=345.
Variable with standardized differences greater than 0.1.
Results
Descriptive Analysis
A total of 360 patients were included: 65 (18.1%) in the APD-RPM cohort and 295 (81.9%) in the APD-without RPM cohort. The baseline characteristics of the included patients, for the full sample and each of the cohorts, are presented in Table 1. The mean age was 57 years, and the most frequent cause of CKD was diabetes (42.5%). Most patients were recruited in Bogota (52.5%). Several baseline characteristics showed standardized differences between cohorts greater than 0.1.
The full sample showed means of 0.65 hospitalization events per patient-year and 5.28 hospital days per patient-year. The most frequent causes of hospitalization were cardiovascular (20.4%), gastrointestinal (12.8%), cerebrovascular (11.1%), metabolic (8.9%), and peritonitis (7.2%); hospitalization details are presented in Table 2.
Hospitalization Causes of Full Study Population According to Exposure Status
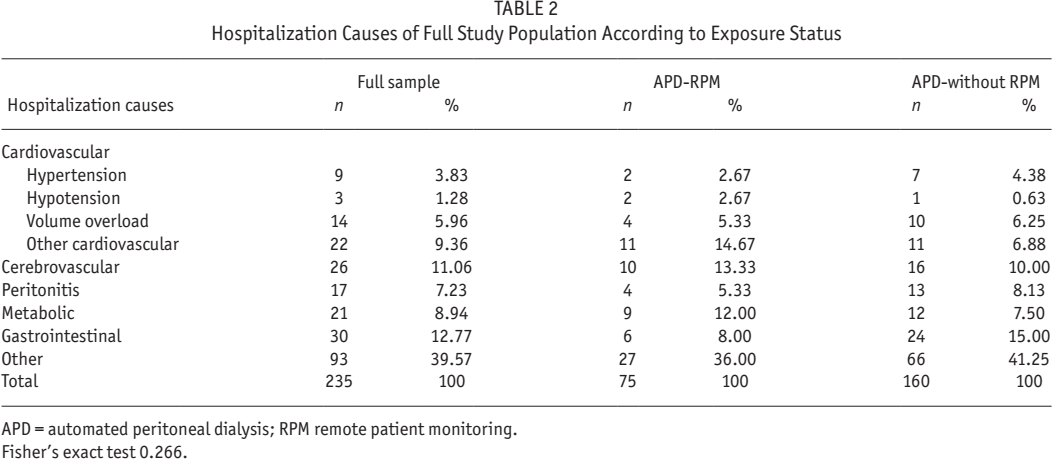
APD = automated peritoneal dialysis; RPM remote patient monitoring.
Fisher's exact test 0.266.
Matching Analysis
Matching analysis was performed to balance the baseline characteristics between cohorts. Table 3 presents the balance assessment of the matched sample with caliper radius of 0.045. An absolute value of standardized difference greater than 0.1 indicates unbalance (13). The results show that basic patient characteristics were well balanced after the matching process. The final matched sample included 63 patients in the APD-RPM cohort and 63 patients in the APD-without RPM cohort. Two patients in the APD-RPM cohort were excluded because of incomplete data sets (missing values for hemoglobin and phosphorus); see also the Supplemental Graph 1 illustrating the successful matching accomplished by the propensity score matching (PSM) procedure.
Baseline Characteristics of Final Matched Sample According to Exposure Status
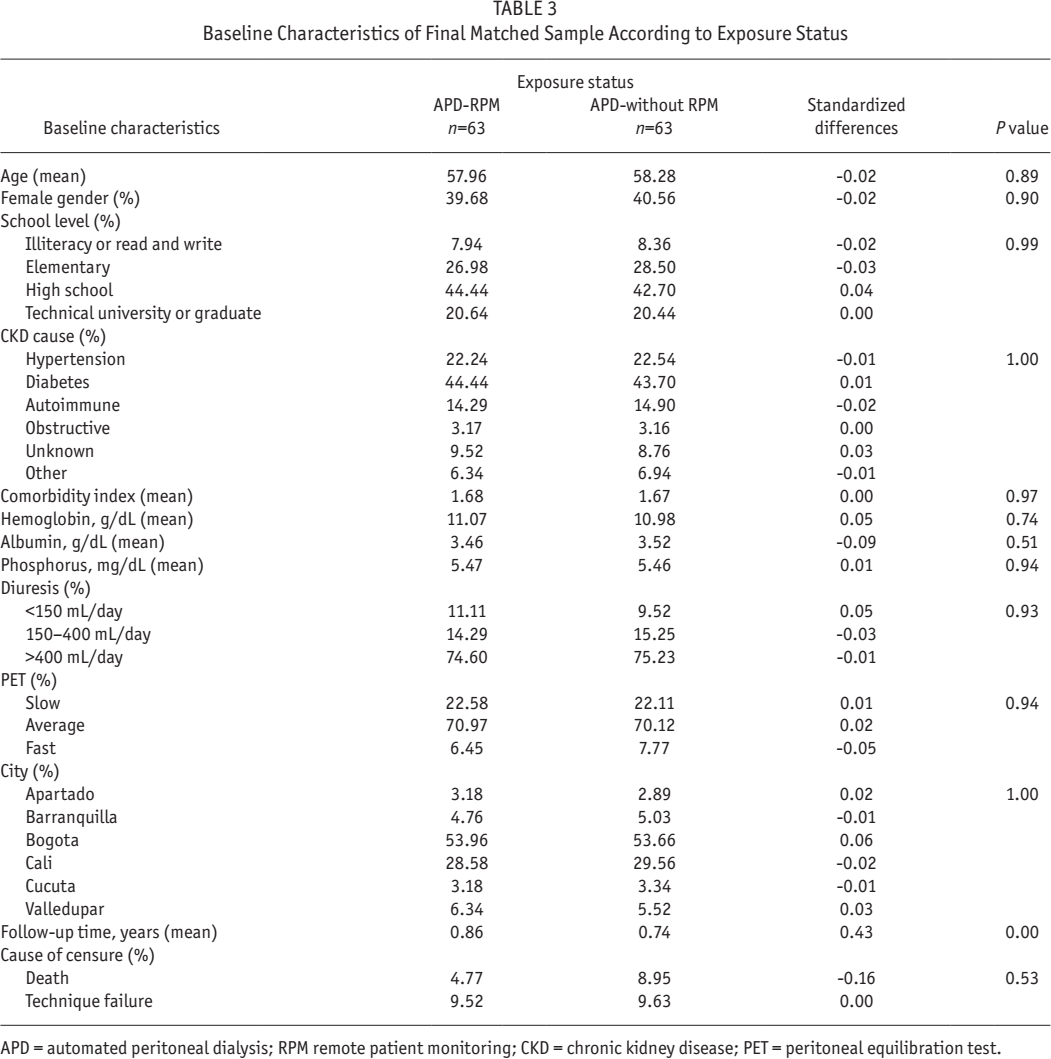
APD = automated peritoneal dialysis; RPM remote patient monitoring; CKD = chronic kidney disease; PET = peritoneal equilibration test.
For the matching samples, the mean follow-up times were 0.86 (standard deviation [SD] 0.27) and 0.74 (SD 0.34) years for APD-RPM and APD-without RPM, respectively; the percentages of technique failure in the 2 groups were 9.52% and 9.63%, and the proportion of deaths were 4.77% and 8.95%; see Table 3.
After PSM (Table 4), APD-RPM compared with APD-without RPM was associated with 0.36 fewer hospital admissions per patient-year, 0.56 (0.34 – 0.78) vs 0.92 (0.73 – 1.11) admissions/year, corresponding to a significantly lower IRR of 0.61 (95% CI 0.39 – 0.95); p = 0.029, and patients with APD-RPM compared with APD-without RPM had on average 6.57 fewer hospital days, 5.59 (2.36 – 8.82) vs 12.16 (7.59 – 16.74) days/ year, corresponding to significantly lower IRR of 0.46 (95% CI 0.23 – 0.92); p = 0.028.
Clinical Outcomes Associated with RPM in Matched Sample Based on Negative Binomial Regression

RPM remote patient monitoring; APD = automated peritoneal dialysis; CI = confidence interval.
Negative binomial regression.
Incidence rate ratio is defined as APD-RPM/APD-without RPM
p<0.05.
Additionally, to confirm the robustness of these findings, we performed analyses with multivariate models using Poisson and negative binomial regressions, to estimate the IRR for the number of hospitalizations and the number of days of hospitalization associated with RPM (Supplemental Table 3).
Finally, given the differences found in the follow-up times, both in raw samples and in matched samples, a model was made in which the follow-up time was included as one of the variables independent of propensity score, and this model led to an adequate balance of the follow-up times in the new matched sample (Supplemental Table 4). Because not all variables were balanced in the final sample (standardized differences > 0.10) and following the recommendations of Austin et al. and Nguyen et al. (16,17), double propensity-score adjustment was used showing IRR = 0.64 (95% CI 0.41 – 0.98; p = 0.04) and IRR = 0.57 (95% CI 0.30 – 1.10; p = 0.09) for hospitalization rate and hospital days, respectively. These results suggest that, when controlling for follow-up time, the use of RPM was associated with a lower rate of hospitalization and hospital stay.
Discussion
The present study is, to our knowledge, the first one aimed at establishing whether there is an association between the use of remote patient monitoring (RPM) in APD patients and improved therapy outcomes. We found that APD therapy with RPM was associated with significant reductions in hospitalization rate (0.36 fewer hospitalizations per patient-year) and hospitalization days (almost 7 days fewer per patient-year). These results, showing that the use of RPM was associated with improved clinical outcomes, appear to be clinically relevant and suggest that RPM could be of value from the perspective of the patients as well as from an economic point of view.
We hypothesize that these results can be the product of several advantages that RPM may confer to the APD program such as better adherence, the achieving of an improved ultra-filtration profile, better blood pressure control, early detection of catheter dysfunction, timely modification of the treatment, reduction in the frequency of visits to the clinic, and—not least—enhanced communication between the patient and the clinical team (8,9,18,19).
It is important to highlight that when outcomes are expressed as counts, the magnitude of the effect in observational studies may vary substantially depending on the statistical analysis used (14,15); thus, the effect size should be interpreted with caution.
One important aspect of our study is that it adresses an evidence gap regarding the influence of RPM on hard outcomes such as hospitalization. In this sense, our study sheds light on how a RPM program can influence results of the APD therapy similar to what has been reported in other fields like cardiac arrhythmias, congestive heart failure, and other chronic diseases (20–22).
The present study has the strength of using statistical matching to control for potential confounding variables, which are frequent in observational studies. Matching included the city where the patient was attended to, comorbidity, and other baseline variables, thus generating sub-populations with and without RPM respectively but matched by the other variables as recommended for propensity score matching (12–14).
Some limitations of the study should be noted. First of all, because of the observational retrospective study design, no conclusions can be made regarding causality. Nevertheless, different analytical approaches were applied showing consistency in the direction of the observed associations; however, a randomized clinical trial would be required to confirm the effects of a RPM program. Second, the number of patients in the RPM group was low, reflecting the recent introduction of RPM technology. Third, the study included incident patients and thus may not reflect hospitalization outcomes in prevalent patients with long dialysis vintage time. The clinical context of Baxter Renal Care Services Colombia and its particular model of attention needs to be taken into account when extrapolating results to other patient populations (9,10,23,24). Fourth, we did not register outcomes from the patient's perspective such as measures of quality of life or satisfaction with care, nor additional variables such as time from PD catheter insertion to initiation of PD and/or history of predialysis care; these factors should be considered in future analysis. Fifth, the retrospective study design hinders a meaningful assessment of the temporal relationship between the RPM intervention and hospitalization.
While more research is needed to understand the implications of RPM from the point of view of the patients and caregivers, it is likely that lower hospitalization rates and hospital days could confer savings for the healthcare system as reported by Makhija and colleagues (25,26).
Conclusions
In conclusion, the use of a standardized RPM program for the management of APD patients was associated with lower hospitalization rates and fewer hospitalization days, supporting the value of RPM as an effective tool to improve clinical outcomes of APD therapy.
Footnotes
Acknowledgments
The authors wish to express their gratitude to all the PD clinical teams who participated in the study.
MS and AB are employees of Baxter Renal Care Services (BRCS)-Latin America, Bogotá, Colombia; BL is employed by Baxter Healthcare, Stockholm, Sweden; JV is employed by BRCS Colombia, Bogotá, Colombia; LGN is employed by Baxter Healthcare, Renal Care GBU Medical, Lund, Sweden; DY is employed by Baxter Healthcare Corporation, Deerfield, Illinois, USA, and, AR is employed by BRCS Global, Chicago, Illinois, USA. GB has received grant/research support from Baxter and served as a statistical consultant for the study. Baxter Novum is the result of a grant from Baxter Healthcare to Karolinska Institutet.
The study was supported by Baxter Renal Care Services Colombia, an independent entity owned by Baxter International, Inc. Funding to support the preparation of this manuscript was provided by Baxter Healthcare Corporation, Deerfield, Illinois. Baxter Healthcare Corporation participated in reviewing the manuscript for scientific accuracy.