
Abstract
Bacterial peritonitis continues to be a significant cause of morbidity and mortality in patients undergoing peritoneal dialysis. Episodes of peritonitis due to coagulase-negative staphylococci (CNS) are especially prone to relapse or repeat, often culminating in catheter removal and technique failure. This pattern is thought to be associated with the production of a biofilm that offers protection against antimicrobials and the host defense systems. We report the successful eradication of repeated episodes of CNS peritonitis using an aggressive multipronged therapeutic approach combining several antibiotics and a thrombolytic agent.
Current management of peritonitis relies on the guidelines published by the International Society for Peritoneal Dialysis (ISPD). The initial phase involves the use of empiric antibiotics, such as vancomycin or a first-generation cephalosporin, for gram-positive coverage and a third-generation cephalosporin or an aminoglycoside for gram-negative organisms. Although no antibiotic regimen has been proven to be superior to others, the resolution rate was superior with the use of ceftazidime plus a glycopeptide as initial empiric therapy (2,6).
Data regarding the use of fibrinolytics to dissolve biofilm are conflicting. There is currently no consensus regarding their use as adjunctive therapy (2,6–8). Based on a retrospective analysis, Demoulin et al. concluded that, added to antibiotics, intraperitoneal (IP) urokinase and oral rifampicin led to a successful catheter salvage in 64% of the cases of CNS peritonitis (7). Tong et al.'s results, on the other hand, were negative; in their randomized control trial, the use of IP urokinase failed to show any benefit when added to conventional therapy. Although no significant adverse events were encountered with the IP urokinase, the rates of catheter removal, mortality, and response to therapy were similar in the urokinase + antibiotic vs placebo + antibiotic group (8). Is it important to recognize, however, that of 88 cases in that series, only 3 were caused by CNS.
We report the successful eradication of repeated episodes of CNS peritonitis using an aggressive multipronged therapeutic approach combining several antibiotics and a thrombolytic agent.
Methods and Results
Over a period of 2 years, we encountered 4 patients with multiple episodes of CNS peritonitis. The most common complaint at the time of presentation was abdominal pain, followed by cloudy peritoneal effluent and subjective fever. One of our patients was hypotensive, likely due to concomitant Clostridium difficile colitis, and required a short hospitalization. The others remained as outpatients throughout their course. All patients were using daily topical gentamicin cream or ointment at the catheter exit site. At the time of diagnosis, the patients did not exhibit any signs of exit-site or catheter tunnel infection.
The diagnosis of peritonitis was based on at least 2 of the following: clinical features consistent with peritonitis, i.e., abdominal pain or cloudy effluent, white blood cell count greater than 100/μl with at least 50% polymorphonuclear cells, and positive peritoneal fluid culture. As seen in Table 1, Staphylococcus epidermidis was identified as the pathogen in 3 of the cases; Staphylococcus capitis was isolated from the peritoneal fluid of our fourth patient, who subsequently experienced an infection caused by S. epidermidis. All pathogens were methicillin-sensitive. We had no cases of culture-negative peritonitis. All the patients were retrained on appropriate sterile technique following the episode of peritonitis.
Case Summaries
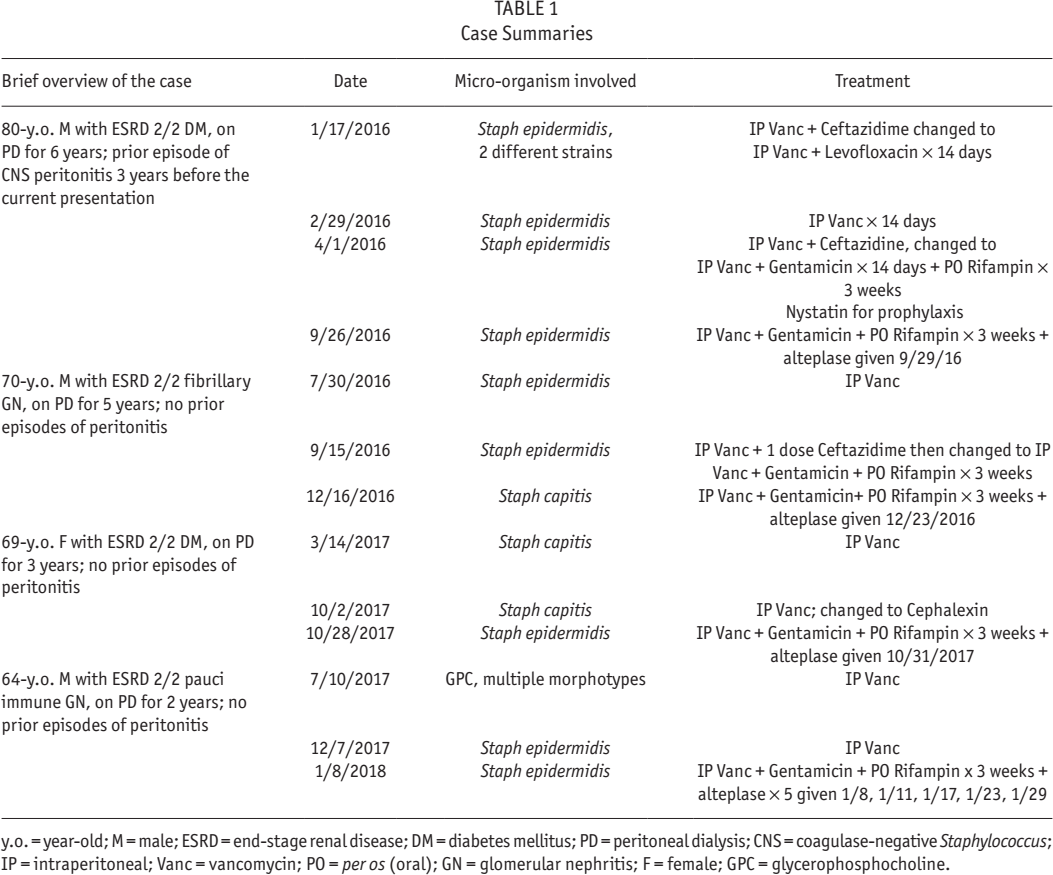
y.o. = year-old; M = male; ESRD = end-stage renal disease; DM = diabetes mellitus; PD = peritoneal dialysis; CNS = coagulase-negative Staphylococcus; IP = intraperitoneal; Vanc = vancomycin; PO = per os (oral); GN = glomerular nephritis; F = female; GPC = glycerophosphocholine.
During their initial presentations, all patients were treated with IP vancomycin dosed by trough levels. This was subsequently changed to oral (PO) antibiotics based on culture sensitivities, for a total duration of 14 days. Unfortunately, each of the patients experienced a relapse, repeat, or new infection. Aminoglycosides provide synergistic antistaphylococcal activity and have been reported to better penetrate biofilm than do other antibiotics (9). Therefore, the second episode was treated with a combination of IP vancomycin + 0.6 mg per kg IP gentamicin administered as a single dose. Similarly, rifampin has been reported to be beneficial in the treatment of infections associated with biofilm (10). Therefore, 300 mg PO rifampin twice daily for 3 weeks was added in 2 out of 4 cases. This approach, which did not include the use of a thrombolytic, was also unsuccessful and was therefore not employed for the subsequent 2 patients. One last trial of salvaging the access was attempted. All 4 patients were treated with 6 mL of intraluminal alteplase (1 mg/mL), which was allowed to dwell for at least 6 hours, in addition to IP vancomycin, IP gentamicin, and PO rifampin 300 mg twice daily for a total of 21 days. The alteplase was administered at variable times within the first 10 days of the diagnosis. Catheter salvage was achieved in all 4 cases using the combination of IP vancomycin, IP gentamicin, oral rifampin, and intraluminal alteplase. The therapeutic regimens employed for each infection are depicted in Table 1. For each of the patients, more than 18 months has elapsed since the last course of treatment and none of them has experienced a repeat intraperitoneal infection.
Discussion
When added to sensitivity-based antibiotic therapy, the use of rifampin and fibrinolytics has been reported to achieve catheter salvage and help treat resistant and recurrent peritonitis. It was hypothesized that they were doing so by dissolving the biofilm—a media where the sessile bacteria are protected from the effect of antibiotics. This remains a controversial topic, as several studies have reported no improvement in outcome with the addition of urokinase. The studies are limited mainly as a result of a low patient sample size, randomization bias, and difference of the medication protocol. Addition of gentamicin to vancomycin, rifampin, and a thrombolytic agent as employed in this case series has, to our knowledge, not been previously described.
The ISPD defines a relapse of peritonitis as an infection occurring within 4 weeks of completion of therapy of a prior episode with the same organism or a sterile episode. An episode of infection with the same organism that occurs more than 4 weeks after completion of therapy of a prior episode is considered repeat peritonitis. Infections with a different organism that occur more than 4 weeks after completion of a course of therapy for a prior peritonitis are considered new infections. Over a period of 2 years, we encountered 4 patients with multiple episodes of CNS peritonitis. As seen from the timelines given in Table 1, these were a mix of relapses, repeat peritonitis, and new infections. We successfully treated all 4 cases with IP vancomycin with the addition of intraluminal alteplase, IP gentamicin, and PO rifampin. It should be recognized that this case series represents the clinical experience of a single center; this was not meant to be a controlled trial and therefore no comparator is available. Yet, the combination of vancomycin, gentamicin, rifampin, and alteplase proved uniformly successful. Unfortunately, this treatment was not employed in a consistent fashion: as can be seen in Table 1, while patients 1 – 3 received but a single dose of alteplase which proved to be effective, patient 4—due to a communication error—inadvertently received multiple doses. Overall, therefore, use of this regimen can be regarded as “hypothesis-generating” at best. Further studies are needed to determine whether this multipronged therapeutic approach—employed with a consistent protocol—is indeed effective in eradicating multiple episodes of CNS peritonitis.
Footnotes
The authors have no conflicts to declare.