
Abstract
Background:
Many patients who experience a venous thromboembolic event have cancer, and thrombosis is much more prevalent in patients with cancer than in those without it. Thrombosis is the second most common cause of death in cancer patients and cancer is associated with a high rate of recurrence of venous thromboembolism (VTE), bleeding, requirement for long-term anticoagulation and poorer quality of life.
Methods:
A literature review was conducted to identify guidelines and evidence pertaining to anticoagulation prophylaxis and treatment for patients with cancer, with the goal of identifying opportunities for pharmacists to advocate for and become more involved in the care of this population.
Results:
Many clinical trials and several guidelines providing guidance to clinicians in the treatment and prevention of VTE in patients with cancer were identified. Current clinical evidence and guidelines suggest that cancer patients receiving care in hospital with no contraindications should receive VTE prophylaxis with unfractionated heparin (UFH), a low-molecular-weight heparin (LMWH) or fondaparinux. Patients who require surgery for their cancer should receive prophylaxis with UFH, LMWH or fondaparinux. Cancer patients who have experienced a VTE event should receive prolonged anticoagulant therapy with LMWH (at least 3 months to 6 months). No routine prophylaxis is required for the majority of ambulatory patients with cancer who have not experienced a VTE event. Most publicly funded drug plans in Canada have developed criteria for funding of LMWH therapy for patients with cancer.
Conclusions:
Evidence suggests that LMWH for 3 to 6 months is the preferred strategy for most cancer patients who have experienced a thromboembolic event and for hospital inpatients, but this is often not implemented in practice. Concerns about adherence with injectable therapy should not prevent use of these agents. Pharmacists should assess cancer patients for their risk of VTE and should advocate for optimal VTE pharmacotherapy as appropriate. If LMWH is the preferred agent, on the basis of the evidence, the pharmacist should educate the patients appropriately and work with the prescriber to ensure best care. Can Pharm J
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism, is a common complication of cancer and its treatment and occurs more frequently in patients with cancer than in patients without it. Patients with cancer have an annualized risk of VTE 6 to 12 times higher than those without cancer. 1 Among patients with cancer, VTE is strongly associated with reduced survival, 2 and thromboembolism is the second leading cause of death among outpatients who are receiving cancer therapy 1 Clinical trial data have demonstrated that anticoagulation therapy for prevention or treatment of VTE in patients with cancer, especially low-molecular-weight heparins (LMWHs), prevents morbidity and may decrease mortality 3 However, despite evidence demonstrating the efficacy of anticoagulant therapy, VTE often goes unrecognized and may be treated suboptimally. Pharmacists are well positioned to aid in enhancing the management of cancer patients who have or are at risk of VTE.
The purpose of this review is to provide an overview of the epidemiology of thrombosis in patients with cancer, to highlight evidence pertaining to its treatment and prevention in this population and to suggest how pharmacists may play a role in improving the care of patients with cancer and VTE.
Methods
A literature review was conducted by searching MEDLINE, EMBASE and International Pharmacy Abstracts for articles published from January 1995 to August 2010 that examined clinical outcomes related to thrombosis and cancer and the pharmacist's role. Online formularies for Canadian provinces were also reviewed to determine coverage for LMWH used for this indication.
Results
DVT and PE
Patients with cancer have a significantly greater risk of morbidity and mortality from thromboembolism relative to patients without cancer. Overall, 15% of patients with cancer will experience symptomatic DVT at some point, but this rate underestimates the importance of the problem when one considers that fully 50% of cancer patients experience asymptomatic DVT and that post-mortem studies have shown a DVT risk of 50% at autopsy, making VTE a possible cause of death in these cases. 4 In fact, 1 in 7 cancer patients undergoing treatment in hospital dies because of pulmonary embolism. 5 Among patients with cancer, the risk of death within 6 months of a VTE event is 94%, 3 times the risk in patients without cancer. 6 Although most VTE events are not fatal, they cause significant morbidity through post-thrombotic syndrome, pain, possible drug interactions and increased readmission to hospital. 2
Risk of thrombosis
Many factors that increase the risk of VTE are inherent to the patient, including thrombophilia, history of thromboembolic disease, advanced age, obesity and female sex. Other risk factors are related to cancer treatment, including oral contraceptives, hormone replacement therapy, tamoxifen therapy, central venous catheterization, chemotherapy (especially thalidomide and bevacizumab), radiotherapy, erythropoietin-stimulating agents, surgery, immobilization and admission to hospital. The cancer itself can influence the risk of thromboembolic disease and the incidence is higher (relative risk 1.02 to 4.34) among those with advanced disease and those with certain tumour types (specifically cancer of the pancreas or brain and lymphoproliferative disease). 7 The presence of disseminated intravascular coagulation is also a known risk factor. Development of Virchow's triad, consisting of venous stasis secondary to compression by the tumour, secretion of prothrombotic factors and proinflammatory cytokines by the tumour and the endothelium and cancer-related damage to the endothelium, leads to the thromboembolic event. 8
Key points
VTE is common in patients with cancer and results in significant morbidity and mortality. A variety of anticoagulants may be used to prevent VTE in hospitalized patients with cancer. Extended-duration LMWH therapy (3–6 months) has demonstrated superior outcomes in cancer patients with an active VTE event as compared to oral anticoagulants.
Prophylaxis
The frequency of VTE in cancer patients being treated in hospital ranges from 0.6% to 5.4%. 9 Among medical inpatients with cancer, rates of VTE are lower with prophylaxis using LMWH, rather than unfractionated heparin (UFH) or placebo, without significantly higher rates of major bleeding. 10 Three large randomized controlled trials demonstrated the efficacy of enoxaparin, dalteparin and fondaparinux, respectively, in preventing VTE in medical patients being treated in hospital (Table 1). 11 –13 In each of these trials, data were reported for nonrandomized cancer subgroups groups. Although these trials provided information about the efficacy of intervention, they had several limitations, including the limited number of cancer patients (5% to 15% of the patients in each trial) and the fact that bleeding events were not reported for the cancer subgroups.
Clinical trial data for prophylaxis of venous thromboembolism in acutely ill medical inpatients (cancer subgroup)
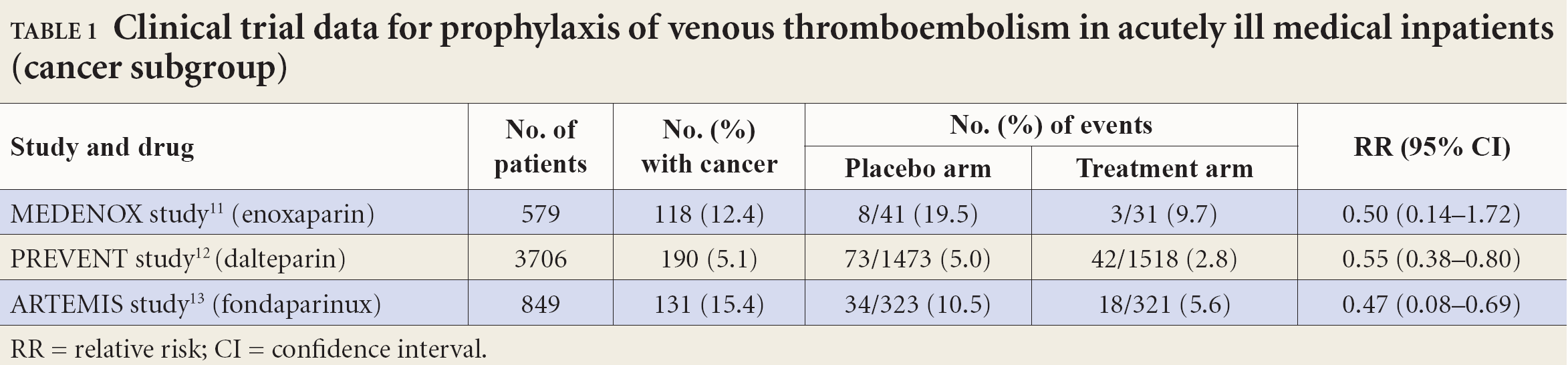
RR = relative risk; CI = confidence interval.
Points clés
La thromboembolie veineuse est fréquente chez les patients atteints de cancer et se traduit par un taux élevé de morbidité et de mortalité.
Divers anticoagulants peuvent ětre utilisés pour prévenir la thromboembolie veineuse chez les patients hospitalisés atteints de cancer.
L'administration d'héparines de faible poids moléculaire sur une longue période (trois à six mois) a donné de meilleurs résultats que les anticoagulants oraux chez les patients cancéreux atteints d'une thromboembolie veineuse active.
Patients with cancer who undergo surgery are at high risk of VTE. Without prophylaxis, rates of proximal vein thrombosis of 10% to 20% and rates of PE of 4% to 10% have been reported in surgical populations. 14 The rate of PE after abdominal surgery in cancer patients is 14 times higher than among patients without cancer. 15 The data clearly demonstrate the efficacy and safety of LMWH for prophylaxis of VTE in this population and the risk of VTE events declines by about 50% with prophylaxis. 16
Prophylaxis in ambulatory patients
Preliminary data from randomized controlled trials involving ambulatory patients with cancer are conflicting. This, in combination with the known risk of bleeding in patients with cancer, suggests that prophylaxis is likely not warranted in the majority of ambulatory cancer patients given the benefit to risk ratio. Conversely, thromboprophylaxis with a fixed, low dose of warfarin (1–2 mg/day) or a LMWH may be warranted for patients with multiple myeloma who are receiving thalidomide- or lenalidomide-based combination therapy 17 Further data are required for this population.
Treatment of VTE
Use of anticoagulants to treat VTE in cancer patients is associated with both substantial benefits and high rates of complications. Most cancer patients with VTE require anticoagulation, but anticoagulation may be withheld for a small subset of patients if there is no therapeutic advantage (e.g., for patients with a high risk of complications of VTE treatment, those whose expected survival is short, those with no planned oncological intervention and those for whom no palliative benefit is anticipated).
Several trials have assessed treatment of VTE with LMWH in patients with cancer (summarized in Table 2). The largest of these, the CLOT trial, compared dalteparin with vitamin K antagonists. 18 Dalteparin was associated with a 52% relative risk reduction (RRR) in the incidence of recurrent VTE during the 6 months of follow-up. There were no significant differences between the 2 treatment groups in the rates of major bleeding or any bleeding. The CANTHANOX study, which was stopped early because of low recruitment, demonstrated a reduction in the primary end point (defined as either recurrent VTE or major bleeding or both) with enoxaparin therapy (7 vs 15 patients, p = 0.09). 19 The end point was driven by major bleeding (which occurred in 5 patients in the enoxaparin arm and 12 in the warfarin arm). The 3-armed ONCENOX study demonstrated no differences between the enoxaparin and warfarin groups in terms of recurrent VTE, major bleeding or death; however, the small sample size precludes strong conclusions. 20 Tinzaparin was more effective than warfarin for 200 patients with cancer in the LITE study 21 In that study tinzaparin reduced the rate of recurrent VTE by about 50%, but the difference was not statistically significant. There were no differences in bleeding rates.
Randomized trials comparing low-molecular-weight heparin and warfarin in patients with cancer
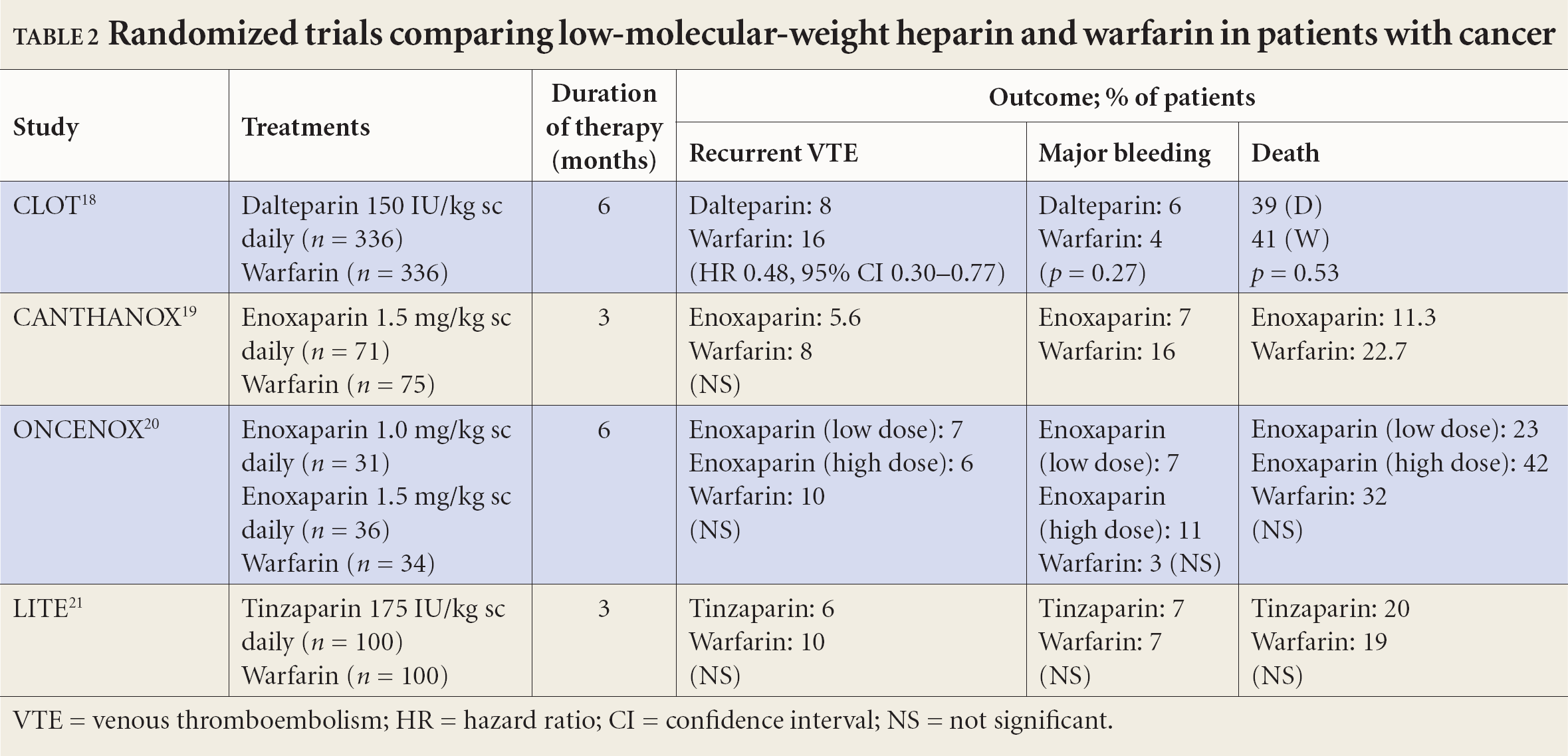
VTE = venous thromboembolism; HR = hazard ratio; CI = confidence interval; NS = not significant.
Guidelines
Given the prevalence and impact of VTE in patients with cancer, as well as the wealth of data demonstrating the efficacy and safety of prophylaxis and treatment of VTE in this population, several groups, including the American Society of Clinical Oncology (ASCO), 9 the American College of Chest Physicians, 22 the European Society for Medical Oncology 23 and the National Comprehensive Cancer Network, 24 have published guidelines for clinicians on this topic (summarized in Table 3).
Summary of antithrombotic guidelines for patients with cancer
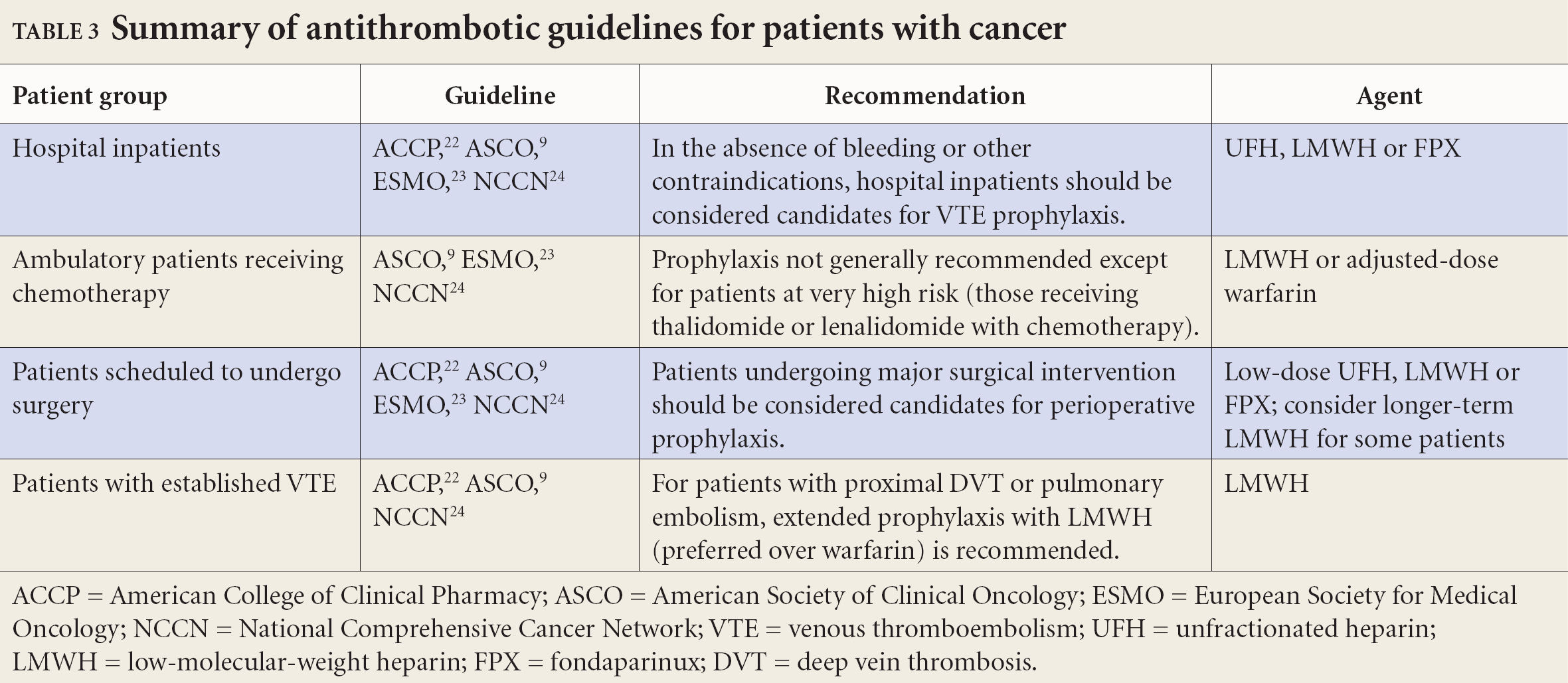
ACCP = American College of Clinical Pharmacy; ASCO = American Society of Clinical Oncology; ESMO = European Society for Medical Oncology; NCCN = National Comprehensive Cancer Network; VTE = venous thromboembolism; UFH = unfractionated heparin; LMWH = low-molecular-weight heparin; FPX = fondaparinux; DVT = deep vein thrombosis.
Although the guidelines support use of LMWH for VTE prophylaxis in cancer patients who are being treated in hospital, a number of contraindications exist. In particular, the ASCO guidelines 9 cite the following as relative contraindications: active uncontrollable bleeding; active cerebrovascular hemorrhage; dissecting or cerebral aneurysm; bacterial endocarditis, bacterial pericarditis or active peptic or other gastrointestinal ulceration; severe, uncontrolled or malignant hypertension; severe head trauma; and placement of an epidural catheter.
Knowledge into practice
Pharmacists can play an important role in preventing and managing thrombosis. Pharmacists are well placed to educate patients about the risk of venous thromboembolism and bleeding, and what to do in case such events occur. Pharmacists can educate patients about both oral and injectable anticoagulant therapy and how to maximize outcomes with these agents Pharmacists can work with clinicians and patients to ensure that patients with VTE and cancer receive therapies demonstrated to provide the best outcomes
Discussion
Despite the data pertaining to the efficacy and safety of prophylaxis and treatment of VTE in cancer patients and several guidelines suggesting appropriate strategies, data from cohort studies suggest that only about half of patients eligible for appropriate therapy receive it. 4,17,23 In understanding this treatment gap, it is important to consider various contributing factors, including whether patients are able to adhere to or gain access to available prophylactic or treatment regimens.
Available data suggest that patients are able to adhere to the LMWH regimens and find them acceptable as treatment strategies. For example, adherence to daily enoxaparin therapy was 94% to 97% in the ONCENOX trial, which exceeded the 92.8% adherence for warfarin. 20 Lee et al. reported that 78% of eligible patients in the CLOT study found long-term self-injection of dalteparin acceptable. 18
In terms of accessibility, the various public drug plans across Canada are divergent in terms of coverage of these agents (Table 4). 25 –31
Provincial coverage for low-molecular-weight heparin therapy
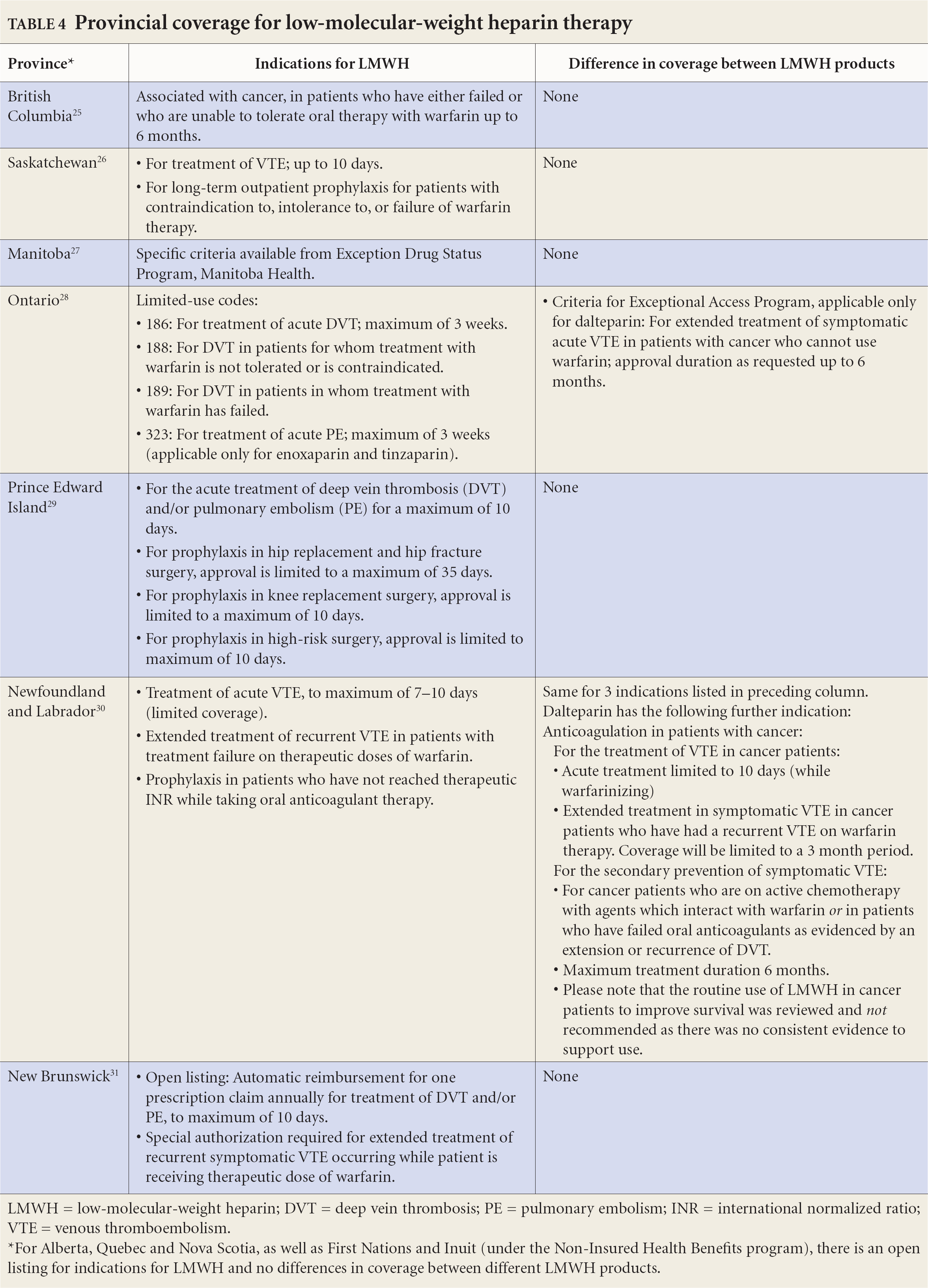
LMWH = low-molecular-weight heparin; DVT = deep vein thrombosis; PE = pulmonary embolism; INR = international normalized ratio; VTE = venous thromboembolism.
For Alberta, Quebec and Nova Scotia, as well as First Nations and Inuit (under the Non-Insured Health Benefits program), there is an open listing for indications for LMWH and no differences in coverage between different LMWH products.
Despite recent evidence demonstrating the efficacy and safety of LMWH in the treatment of VTE in patients with cancer, vitamin K antagonists and UFH continue to be used in some settings. 5 Although the acquisition cost of vitamin K antagonists may be lower than those of LMWHs, these agents may be less effective and more challenging to use in this population. Even in patients who do not have cancer, warfarin control is often suboptimal in the community setting and the time within the therapeutic range is well under 50%. 32 If warfarin dosing is managed traditionally, maintenance of the dose within a therapeutic range, as indicated by time within target INR range, is likely worse for cancer patients than for noncancer patients and is challenging even if dosing is managed by an anticoagulation clinic. Suboptimal INR control may result from multiple drug and food interactions, which may be more likely in cancer patients who are receiving chemotherapy and antiemetic therapy. Liver dysfunction, borderline vitamin K deficiency and gastrointestinal disorders such as vomiting and diarrhea, which are common among cancer patients, may affect the response to vitamin K antagonists. Furthermore, maintaining therapeutic warfarin control may necessitate weekly INR monitoring, which can be inconvenient for patients.
Pharmacists should ensure that the therapeutic approach to anticoagulant therapy for cancer patients is evidence-based and consistent with the literature, published guidelines and patient preferences. As well, pharmacists should be vigilant in reviewing the patient's medication profile for agents such as hormone replacement therapy, oral contraceptives, tamoxifen, thalidomide, bevacizumab and erythropoietin-stimulating agents to ensure that consideration is given to prevention and treatment of thrombosis risk that may be increased by these agents. The authors of the Oncology Workforce Study in the United States recommended that oncology pharmacists can play an important role in preventing and managing thrombosis. 33 Given the impact that pharmacists have had in a wide variety of other disease states, it is only logical that they work to ensure optimal care of cancer patients who have experienced or are at risk of experiencing VTE. Through discussions with patients, pharmacists can better understand the options that have been offered and the choices that have already been made. For example, if the patient has active VTE and is being treated with warfarin, the pharmacist can determine if LMWH has been offered and, if not, can collaborate with the patient and the physician to determine if this might be a preferable treatment strategy, given currently available evidence and the limitations and challenges associated with warfarin anticoagulation. If warfarin is the preferred strategy, the pharmacist should work with the patient and the physician to optimize warfarin control. Bungard et al. recently published a practice tool and practical management tips that pharmacists may find helpful in ensuring best outcomes with warfarin therapy. 34 The Anticoagulation Forum has suggested that patients who are taking warfarin must receive information about the common signs and symptoms of thrombosis and bleeding and what to do if they occur. The common signs of thrombosis include shortness of breath and painful, swollen calves. Bleeding events that are commonly associated with anticoagulant therapy include bruising, minor bleeding, nosebleeds and more significant bleeding events, which may manifest as black stools, blood in the stool, rectal bleeding and vomiting of material with the appearance of coffee grounds. Patients should be advised that if any of these events occur (other than bruising, minor nosebleeds and other types of minor bleeding), they should seek medical attention. 35
Regardless of the selected antithrombotic therapy, pharmacists are in a position to educate patients about the risk of VTE, the risk of bleeding and directions for care if such an event occurs. They can also emphasize the importance of adherence with therapy. Pharmacists should also work with the patient and other caregivers to minimize the impact of drug interactions involving anticoagulant therapy.
Mise en pratique des connaissances
Les pharmaciens peuvent jouer un rôle important dans la prévention et la prise en charge d'une thrombose. Ils sont tous en mesure d'informer les patients du risque de thromboembolic veineuse et de saignement, ainsi que de ce qu'il faut faire dans une telle situation.
Les pharmaciens peuvent expliquer aux patients les différences entre les anticoagu-lothérapies par voie orale et par injection, ainsi que la façon de maximiser les résultats de chacune d'elle.
Les pharmaciens peuvent collaborer avec les cliniciens et les patients pour s'assurer que les patients atteints de cancer et de thromboembolie veineuse reçoivent les traitements qui se sont avérés les plus efficaces.
Conclusions
Patients with cancer are at high risk of VTE, which can result in significant morbidity and mortality. Recent evidence has demonstrated the value of anticoagulant therapy and the use of LMWHs in these patients. All provincial drug plans in Canada have recognized the value of this therapeutic approach and have made these agents available either on an open-listing basis or with specific criteria. In addition, utilization of these agents is acceptable to patients. Given the efficacy and safety data pertaining to LMWH and the challenges of using warfarin in patients with cancer, pharmacists are well positioned to advocate for the approach that best meets patients' needs and to ensure that the selected approach is implemented.