
Abstract

Background/Rationale
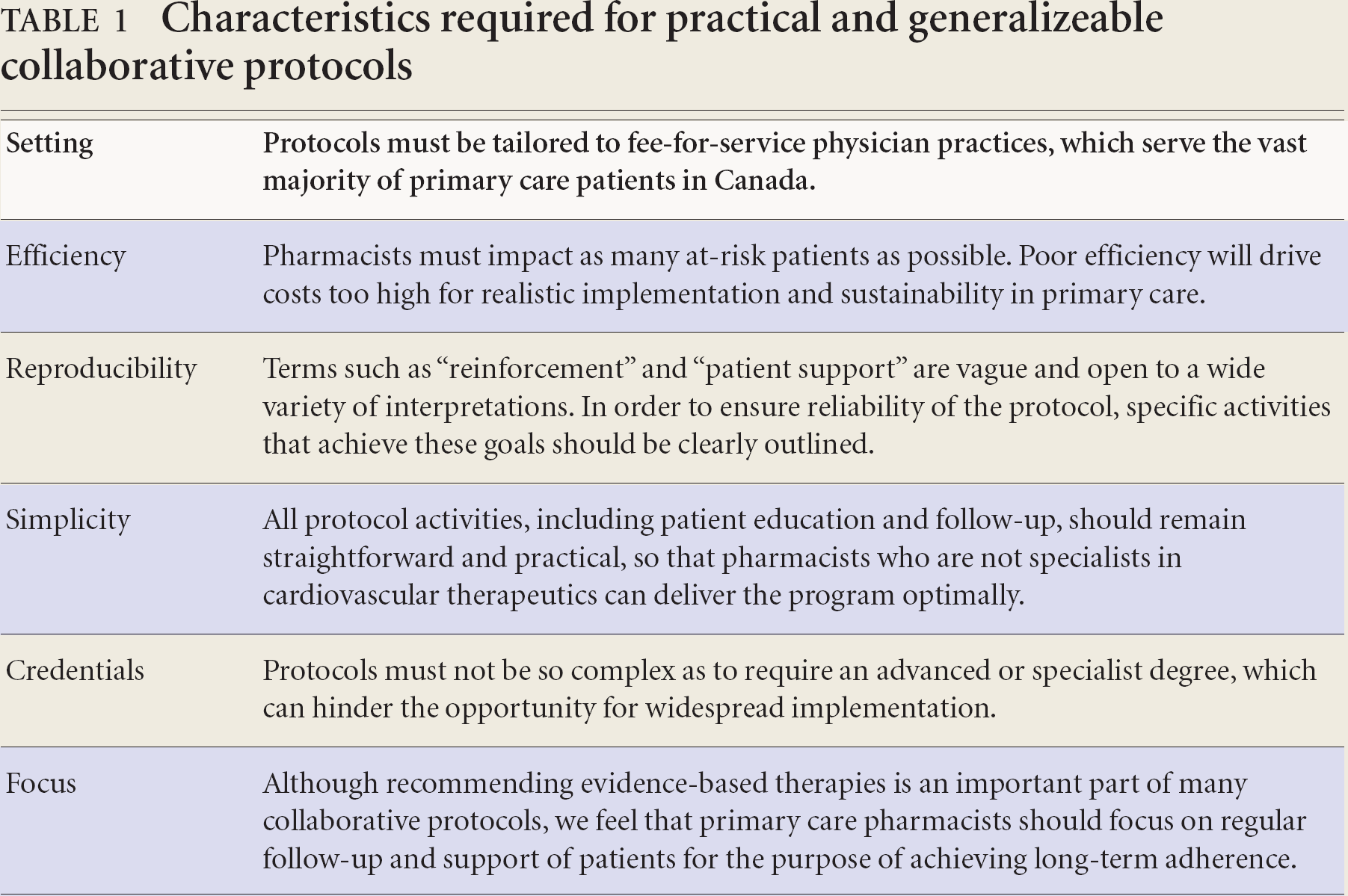
Multidisciplinary and collaborative protocols have been shown to enhance cardiovascular risk reduction strategies in primary care settings.1–10 However, we believe additional studies are required to discover the factors that will facilitate real world success. As such, we have identified several key characteristics that we feel must be in place to make collaborative protocols more realistic and generalizeable to the real world (Table 1).
Characteristics required for practical and generalizeable collaborative protocols
The objective of the Collaborative Cardiovascular Risk-reduction in Primary Care (CCARP) study is to evaluate the success of a specific and reproducible “protocol” of cardiovascular care that is designed for nonspecialist pharmacists who have the opportunity to work collaboratively with a typical fee-for-service physician practice.
Methods
We designed a randomized, controlled trial that compares a pharmacist intervention (following the CCARP “protocol”) with that of usual care for the purpose of reducing cardiovascular risk among primary care patients. The setting for this study is a large family medicine practice in Saskatoon, Saskatchewan. The study has received ethics approval from the University of Saskatchewan's Biomedical Ethics Board.
Patient selection/recruitment
Eligible patients include those with a high-moderate or high-risk classification (≥15% 10-year risk of cardiac death or non-fatal myocardial infarction) as determined by the Framingham risk calculation, or those exhibiting a coronary artery disease risk equivalent (coronary artery disease, peripheral artery disease, cerebrovascular disease, or diabetes mellitus). 11 Exclusion criteria include those with severe psychiatric conditions or dementia, symptomatic heart failure (NYHA class III or IV), terminal illness, concurrent participation in an investigational study, or women who are pregnant or lactating. Due to privacy concerns, patients can only be recruited through physician or self-referral.
Treatment groups
After informed consent has been obtained, the pharmacist completes a medication history of the patient. Patient's individual risk factors are identified and his or her 10-year risk for cardiac death or non-fatal myocardial infarction is determined. Basic information on cardiovascular disease (CVD) risk reduction strategies is discussed and written material is provided. An emphasis is placed on clinical targets and the recommended pharmacological management, as outlined by current clinical practice guidelines.11–14 Patients who meet all the inclusion criteria are randomized into 1 of 2 treatment groups: the follow-up group (intervention) or the single contact group (usual care). Randomization lists were generated in permuted blocks of 4 and stratified for each physician.
Patients randomized into the single contact group will receive no further contact with the pharmacist, and will return to their usual physician care. Those randomized to the follow-up group will receive continuous follow-up and reinforcement by the pharmacist at a minimum of every 8 weeks. Follow-up occurs in person, by telephone, mail, or electronic mail.
Although the delivery of information during follow-up visits is patient-specific and does not require that a standardized content be covered, form letters and patient contact strategies have been developed to provide a “protocol” to help guide pharmacists in their ongoing support for patients. Providing a large amount of information during a single follow-up, unless specifically requested by the patient, is discouraged. Emphasis is placed on short follow-up contacts that focus on reminding and “congratulating” or encouraging patients with respect to adherence and clinical targets. Potential triggers for patient follow-up are outlined in Box 1. Each patient contact is documented to include the date, method of intervention and information provided.
Triggers for patient follow-up in treatment group
Communication of relevant laboratory results in comparison to goals
Within 7 to 10 days after the initiation or change of medication to assess tolerability
Within 7 to 10 days after experiencing an adverse event to ensure resolution
To ensure patient was able to procure necessary follow-up appointments
In patients who are at goal or are stable: mailouts providing patients with clinical goal reminders, disease-specific information, exercise program, or dietary information as appropriate
A list of baseline and follow-up laboratory tests was pre-determined (Box 2), and is ordered by physicians at the time of patient referral. Other relevant laboratory tests may be ordered at the request of the pharmacist. All patients are to be followed for a minimum of 6 months.
Outcome measures
The primary endpoint is the mean reduction in global cardiovascular risk status as measured by the Framingham risk calculator. Because Framingham risk scores are not validated for secondary prevention situations, we have developed and are currently testing another indicator of global cardiovascular risk improvement, the CRI20 (not discussed here), that will be used to measure risk reduction success. Secondary endpoints include individual modifiable CVD risk factors, development of cardiovascular events, optimal drug utilization rates, and long-term medication adherence.
Baseline and follow-up laboratory tests
Lipid panel
Fasting blood glucose
HbA1c (if applicable)
Renal function tests (creatinine, microalbumin, electrolytes)
Liver function tests (AST, ALT)
Thyroid-stimulating hormone (TSH)
Sample size
A sample size of 154 (77 in each treatment group) will provide 80% power to detect a 2-point reduction in the 10-year coronary artery disease risk score with a one-tailed alpha of 5%. The expected effect size was estimated from an unpublished primary care initiative previously conducted in Saskatchewan.
Current status of the study
The first patient was randomized in August 2006, and as of March 2006, 158 patients have been randomized. The study is expected to be completed late summer 2007.
Footnotes
Unrestricted funding for this study was provided by a Rexall Research Trust Grant administered through the College of Pharmacy & Nutrition, University of Saskatchewan. Charity Evans is funded through a Clinical Research Initiative Fellowship from the Canadian Institute of Health Research (CIHR).
Acknowledgements:
A special thank-you to the physicians of City Centre Family Physicians, Saskatoon, Saskatchewan, for their continued participation in the study: Drs. A. Doig, D. Stefiuk, F. Wardell, S. Goluboff, L. Ledray, T. Gabruch, I. Basker, D. Andres, S. Fenton, C. Mensah, L. Illamperuma, L. Merryweather.