
Abstract

Key point
This paper analyzes why there has been a lack of progress in improving medication adherence and examines possible remedies. Large improvements in adherence can be achieved by a series of interventions through a variety of media, as opposed to a one-time action through a single medium.
Last issue's Part I review of medication adherence initiatives defined nonadherence and detailed the magnitude of the problem and the efforts to improve it, as well as providing a review of recent literature on adherence problems in elderly patients, in heart failure patients, in hypertensive patients, and in those with other cardiovascular diseases. The disease review continues in this issue, and examines goals for pharmacists and establishes some direction for practice change.
Efforts to improve
HIV patients
Targets for adherence in HIV patients have been set high (at 95%), because of evidence of poor outcomes below this level. One study describes the use of electronic monitoring devices (EMD). HIV-infected patients were treated with highly active prescriptions that were placed in a container with an EMD. In this population, the major reason patients gave for not using the EMD as instructed was the concomitant use of dosette-type pillboxes. This use accounted for about 20% of missed EMD data. 1 Of particular interest to pharmacists is the recommendation to avoid the use of EMDs in populations that rely heavily on pillboxes. As pillboxes are often used as adherence tools for patients with numerous medications, EMDs may not be beneficial adjunctive interventions in these populations. A Spanish study also reviewed factors influencing adherence in this same population. 2
A group of pharmacists at St. Michael's Hospital in Toronto has developed a Medication Adherence Support Toolkit (MAST-HIV). The kit includes general information on medications, why adherence is important, readiness to start, barriers to adherence, strategies to improve, and advice for staying informed. It also includes health professionals' telephone numbers, questionnaires, checklists, and tips and interactive charts. 3
Inciardi and Leeds found that the community pharmacy refill record was a valid instrument to measure adherence to antiretroviral agents and to predict viral load outcomes. 4
A news report on a study by Mills at Toronto's Centre for International Health and Human Rights revealed that North American HIV patients have an adherence rate of about 55%, while counterparts in sub-Saharan Africa are at 77%; co-factors identified with poor adherence were “pill fatigue,” poor relationships with the doctor, and depression, alcohol, and drug abuse. 5
A controlled Taiwanese study showed better self-care, including adherence, 3 months into a once-a-week teaching session that was followed by continuity and telephone counselling. 6
A California study suggests that even 60% adherence to non-nucleoside, reverse-transcriptase inhibitors can induce viral suppression; however, more importantly, reduced disease progression and mortality improve with higher levels. 7
Gastrointestinal disorders
Kane reviewed the problems of nonadherence to 5-aminosalicylic acid preparations in ulcerative colitis patients. 8
Psychiatric disorders
A study using a Medication Event Monitoring System to measure the adherence rate to psychotropic medications of monolingual Hispanics, bilingual Hispanics, African Americans, and Caucasians 9 observed significant differences, even after controlling for confounding factors. The adherence rate for Caucasians was 90%, compared with 76% for the other ethnic groups. As identified in other diseases, the presence of depressive symptoms was associated with a lower adherence rate. Pratt et al. present some interesting observations with respect to pill counts, self-reporting of compliance, and other psychiatric medication adherence issues. It appears that self-esteem and attitudes toward health are significant factors in adherence with psychoactive medications. 10
California investigators reviewed adherence issues in mood disorders where nonadherence ranged up to 60%. Among barriers were denial of diagnosis, side effects, dependency fears, and views that the medication was ineffective. Among the promising interventions is concordance therapy, interventions based on the health-belief model, and cognitive behaviour. 11
Lipid disorders
A Montreal study recruited nonadherent patients, defined as taking <80% or >120% of prescribed consumption, and then pharmacists educated patients on lipid disorders, the benefits of therapy, and lifestyle modifications, with subsequent telephone follow-up every 2 months. 12 Adherent patients increased by 15%, days-to-refill were reduced by 11 days, and plasma lipids decreased significantly. Patients were willing to pay $35 for a 30-minute consultation.
Likewise, a recent Montreal study used provincial health records to analyze persistence of statin recipients. Persistence fell to 67% in the first 6 months of treatment and to 39% at 3 years. 13 Lower persistence rates were seen in patients without cardiovascular risk factors, in those using several pharmacies and physicians, and in those taking fluvastatin, lovastatin, and atorvastatin vs simvastatin and pravastatin.
Another Quebec study from the province's insurance registry showed greater 24-month persistence with statins than with other agents (60% vs 43%). 14 Patients over 60 years had higher levels of persistence and adherence than those under 60 (55% vs 43%). Likewise, those with concurrent diabetes or cardiovascular disease showed higher persistence than did those without these diseases (59% vs 37%).
Benner et al. reviewed patients in a Southeastern US managed-care program for patients on statins. They found that greater reduction in LDL cholesterol levels during the first 3 months of statin therapy was associated with greater adherence to drug therapy. 15
Blackburn et al. reviewed Saskatchewan databases to study adherence to statins, beta-blockers, and ACE inhibitors after a first cardiovascular event. 16 On average, adherence dropped to 60% after 1 year. They found that patients who exhibited early adherence tended to maintain it. In another study, this investigator measured cardiovascular morbidity associated with nonadherence. 17 Patients in the adherent group had one-half the chance of another myocardial infarction (MI) vs the nonadherent group.
Peterson conducted a meta-analysis on interventions to improve adherence in hyperlipidemia. Of 484 studies, only 4 met the study criteria. These interventions had little effect on drug adherence, and clearly more studies are needed to assess how to improve drug adherence in patients with hyperlipidemia. 18
A US study revealed that provision of pharmaceutical care by community pharmacists in orlistat therapy could improve both persistence and outcomes. 19
Points clés
Cet article vise à analyser les raisons qui expliquent l'absence de progrès quant à l'observation des traitements et à proposer des solutions pour y remédier. Les traitements prescrits seraient mieux suivis si une série d'actes et différentes méthodes étaient mises en jeu, plutôt qu'une seule intervention par l'entremise d'un procédé unique.
Osteoporosis
In a review of adherence issues in osteoporosis treatment, Silverman and Gold pointed out that 12-month persistence is poor with bisphosphonates (19%–23%) and for raloxifen (16%). 20 They also quote higher values of persistence with weekly versus daily bisphosphonates (44% vs 32%) in another study, but indicate that the curves are parallel and that there is a rapid decrease during the first 3 months of therapy. The complex administration requirements of bisphosphonates are partly responsible, but a poor health attitude and costs are also involved.
Applying some psychology
For long-term interventions, use of the Transtheoretical Model of Change has been shown to improve adherence. 21 The model describes 5 separate stages of change that lead to adoption of new therapies: pre-contemplation, contemplation, preparation, action, and maintenance. The strategies are designed to identify a patient's stage of change and to apply stage-specific interventions to promote adoption of the change. For example, bullying, pushing, or providing in-depth information at the pre-contemplation stage may even delay movement to contemplation; this stage requires empathetic listening or discussion of present behaviour, as well as time.
In other words, pharmacists need to understand that patients do what they choose. Pharmacists should concentrate on educating, empathizing, and supporting good decisions!
Adherence and health outcomes
In evaluating health care, nothing speaks louder than health outcomes: measuring the intervention on major health changes over time. Simpson, in a recent meta-analysis, showed that good adherence to beneficial drug therapy was associated with lower mortality, as was good adherence even to a placebo. 22 Indeed, adherence may be a surrogate marker for overall health behaviour. This Canadian study proposes the existence of a so-called “health adherer” effect. Such an effect is disputed by another Canadian group studying mortality after acute myocardial infarction. 23 The latter group found that lower mortality was associated with adherence to specific drugs, namely statins and beta-blockers, but not with adherence to calcium channel blockers (which had acted as a control), suggesting that this minimizes the “adherer effect” theory at least for these categories.
Two studies among diabetes and post-MI patients indicate a clear relation between poor adherence and high mortality.24,25 The authors emphasize the need to assure continuity of care between the hospital and community.
One recent study deserves serious attention by all pharmacists. Known as the Federal Study of Adherence to Medications in the Elderly (FAME), 26 this prospective randomized trial not only shows that increased adherence leads to improved outcomes, but also provides a model for increasing adherence to unprecedented levels. It involved independently living elderly patients taking 4 or more regular medications, and focused on hypertensive and hyperlipidemic patients. All patients received 6 months of the intervention: medication education, pharmacy care follow-up every 2 months, and special blister packs for their medications. Then, 1 group was randomized to continue this care. After 6 months, pill counts showed that medication adherence increased 36% from prior to intervention. Moreover, a 16-fold increase (from 5%–99%) occurred in those patients who were adherent to 80% of their medications. After 12 months, those who continued on pharmacy care maintained their adherence, whereas adherence declined in the others in “usual care.” In addition, for those followed, there were significant decreases in LDL-cholesterol and systemic blood pressure only in the intervention group. This study has major ramifications for pharmacy practice — for both the cognitive care side and the distributive packaging side.
Practice change
Reinforcement of knowledge by various methods (i.e., paper, verbal, media) and opportunities to openly discuss the issues (private counselling area) increase the likelihood of success, and thus require repeating every 2 months.
Osterberg's review 27 of adherence included several strategies for improving adherence (Table 1).
Strategies for improving adherence to a medication regimen
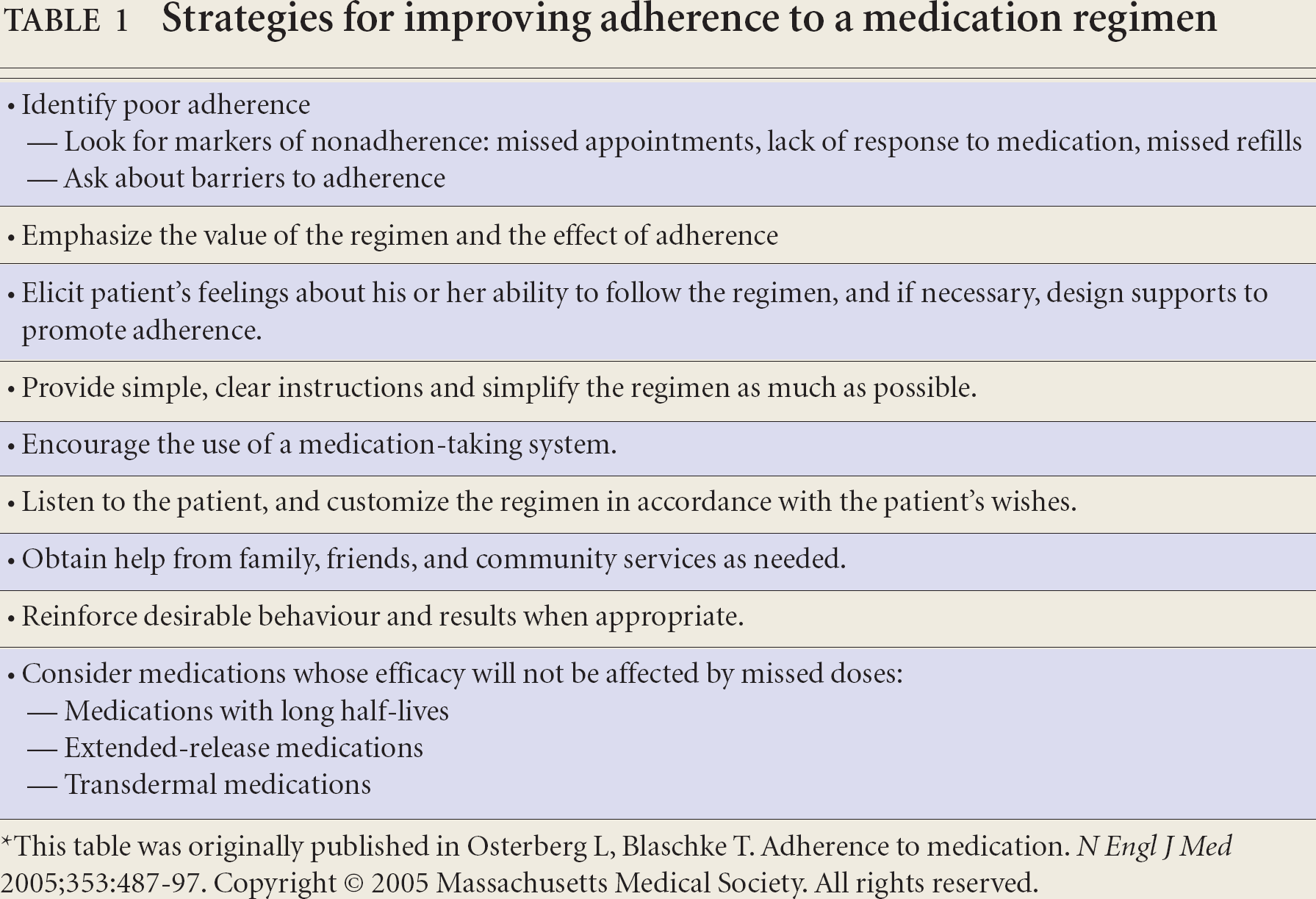
This table was originally published in Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353:487–97. Copyright © 2005 Massachusetts Medical Society. All rights reserved.
Combine convenient care, counselling, reminders, and self-monitoring. Create individualized instruction with written material or visual aids
The importance of improving strategies to encourage persistence of patients with these chronic therapies cannot be underestimated. The cost savings to the health care system is far superior to the cost of the drug in an adherent patient; conversely, nonadherent patients cost the health care system thousands of additional dollars and “deceive” the health care community because of the belief that they are, in fact, on the recommended therapy and therefore forego any further interventions.
Other advances
Our own study of RxCanada's “Health Inform,” a patient education program that is mailed every 2 months for a year, revealed significant impact. 28 Our analysis of 2005 persistence rates at 12 months revealed a 6% increase for those who used inhalers to 14% for those using antihypertensives, compared with those patients who did not receive the information. Rx Canada has also developed a “Reminder Call Program” to notify patients whose refill prescriptions are overdue. Pharmacists contact these patients and counsel them on adherence. An automated reminder call system is also available. A new program, Initial Prescription Program, is being developed to replace drug sampling, particularly for patients with chronic diseases where pharmacist counselling on adherence during the initial visit is critical. A Professional Pharmacy Consultation Program is also available following the first 7 to 14 days after initiating a new therapy. Pharmacists call patients to discuss their medication and address any related questions. In all the Rx Canada—developed programs, pharmacists are remunerated for these services, including provision of additional counselling.
Telephone calls to review problems that might lead to discontinuance are part of the adherence story. Studies indicate that adherence rises significantly when patients are called a few days after beginning therapy to review drug-related problems (a month after for statins) and then regularly to review problems, changing attitudes, or other reasons for discontinuing therapy. 29 A recent Montreal controlled study found that a pharmacist call on Day 3 of antimicrobial therapy did not lead to improved adherence or infection outcomes, but did permit more identification of drug-related problems. 30 A Hong Kong study showed that telephone counselling by a pharmacist midway between clinic visits over a 2-year period led to a significant reduction in all-cause mortality on patients. 31
A hospital pharmacist discharge counselling and follow-up telephone call within 3 to 5 days lowered the incidence of drug-related problems from 11% to 1% at 1 month. These problems involved discrepancies between preadmission and discharge orders in 68% and nonadherence issues in 23%. 32
The use of a check-off form when a patient has a refill and questioning the patient about drug-related problems (DRPs) allow specific pharmacist intervention and saves time. Reimbursement for check-off forms for patients and subsequent resolution of the DRP can lead to better adherence. Many small interventions are possible, leading to greater adherence. Some have been researched, while others still need to be.
There is also room for industry to sponsor more programs, such as the Study of Cardiovascular Risk Intervention by Pharmacists (SCRIP) program, where patients at risk of a certain disease are identified for appropriate therapy. 33 This is a vast area for improving the health of undiagnosed Canadians who are unaware of the health hazards that they carry each day. It is estimated, for example, that only 50% of patients with hypertension are identified, with similar figures for those with diabetes. For lipid disorders and osteoporosis prevention, the figures are even more significant. Providing reimbursement and encouragement to pharmacists to identify these patients means that patients are being introduced to appropriate care at a much earlier stage, before complications from these diseases cause major damage, hospitalizations, and other morbidity.
Conclusions
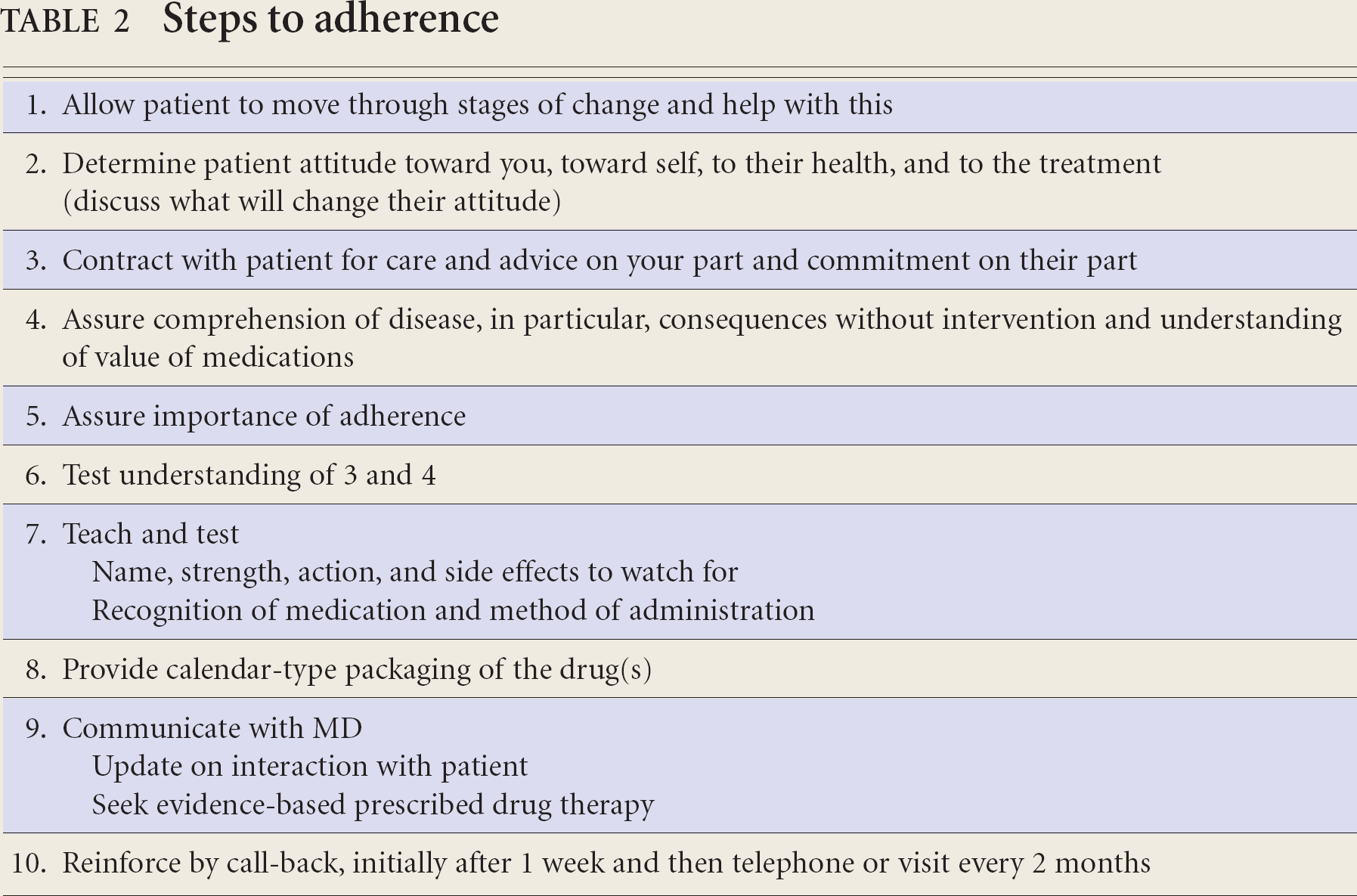
The remedial road to adherence is steeped in complexity. Clearly, the causes differ in individuals, thus making individualization necessary. Research continues to show that a one-time single intervention by only one medium has been disappointing and produces insignificant results. 34 Several approaches appear necessary for success. Based on our knowledge to date, Table 2 outlines a series of interventions that will increase general adherence; such interventions address a variety of causes.
Steps to adherence
The future
The problem of nonadherence will continue unless there are efforts to decrease it. Although awareness by all involved (i.e., patient, pharmacist, physician, manufacturer, and insurer) is one step, it needs to be continual. Health professionals need to re-allocate how they spend their time. The offering of pharmaceutical care, which always considers the level of adherence, along with the principles of concordance therapy, would significantly improve patient health outcomes and decrease the overall costs to the health care system. Taking steps toward including the elements of pharmaceutical care would be a logical strategy. Consumer demands for this level of service would also help advance this.
Clearly, manufacturers and payers still have much that can be done. To that end, tested adherence-inducing packaging and reminders should be advanced. The need to individualize approaches to concordance is critical. But it is also evident that a multi-pronged approach is valuable, as well as the use of reinforcement by a variety of methods, such as telephone calls, interviews, paper information, and medication calendars. The provision of prescription medication should be seen as an occasion when we ask patients to commit to a contract. For this reason, we should be prepared to provide all the available information and reminder tools to facilitate this task.