
Abstract
Arthritis is the leading cause of disability in North America, with osteoarthritis (OA) the most prevalent disease within this classification. 1 In Canada, the economic impact of muscu-loskeletal disease is second only to cardiovascular disease. 2 It is estimated that, in the next 10 to 20 years, the prevalence of OA will increase by 50%, resulting in a large personal and societal burden. 3 Knee OA, in particular, is common and disabling. Evidence-based management of knee OA involves the use of both nonpharmacological and pharmacological approaches.4–9 Recent studies, however, have shown gaps in identifying knee OA 10 and in delivering the appropriate interventions. 11
In the Pharmacist Identification of New, Diagnostically confirmed OA (PhIND-OA) study, we demonstrated that pharmacists could identify people with previously undiagnosed knee OA. 12 A recent randomized controlled trial by Hay and colleagues indicated that enhanced pharmacist medication review was as effective as exercise in the short-term management of knee pain, and both were more effective than usual care. 13 A strategy, therefore, that uses pharmacists to identify those individuals in the community with knee OA in order to perform a medication review and to provide a referral to other health care practitioners (i.e., primary care physicians and physiotherapists) may prove effective in addressing the care gap for knee OA. We hypothesize that pharmacists could play a role in addressing these gaps in OA patient care.
Resources
The Arthritis Foundation — The Arthritis Society — EULAR Recommendations 2003: an evidence-based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis 2003;62:1145–55. National Institute of Arthritis and Musculoskeletal & Skin Diseases. Handout on Health: Osteoarthritis —
Methods
Methods
Knee OA management
Education, including counselling on the symptoms and other aspects of knee OA. Patients will be provided with an opportunity to participate in the Arthritis Self-Management Program (ASMP).
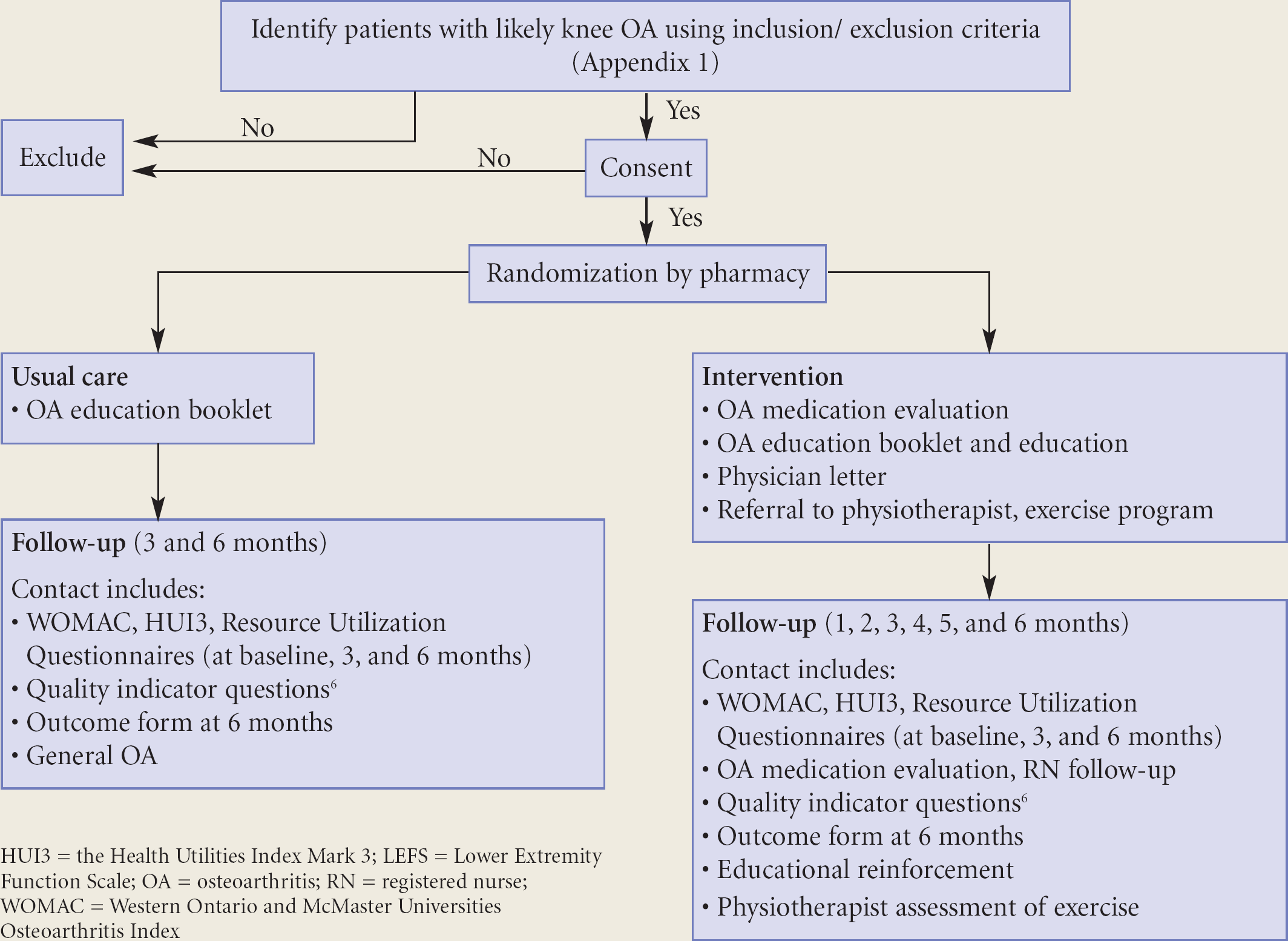
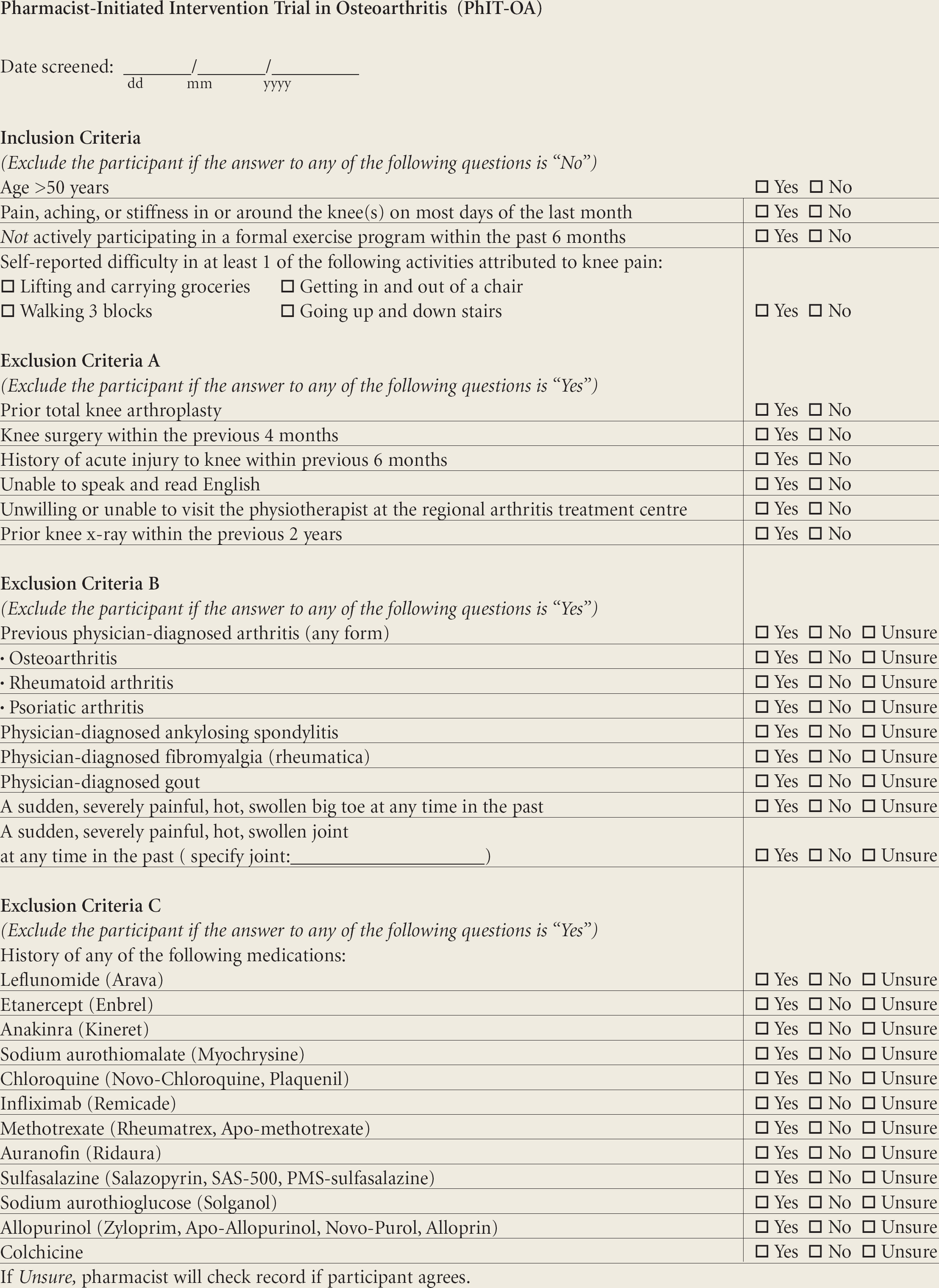
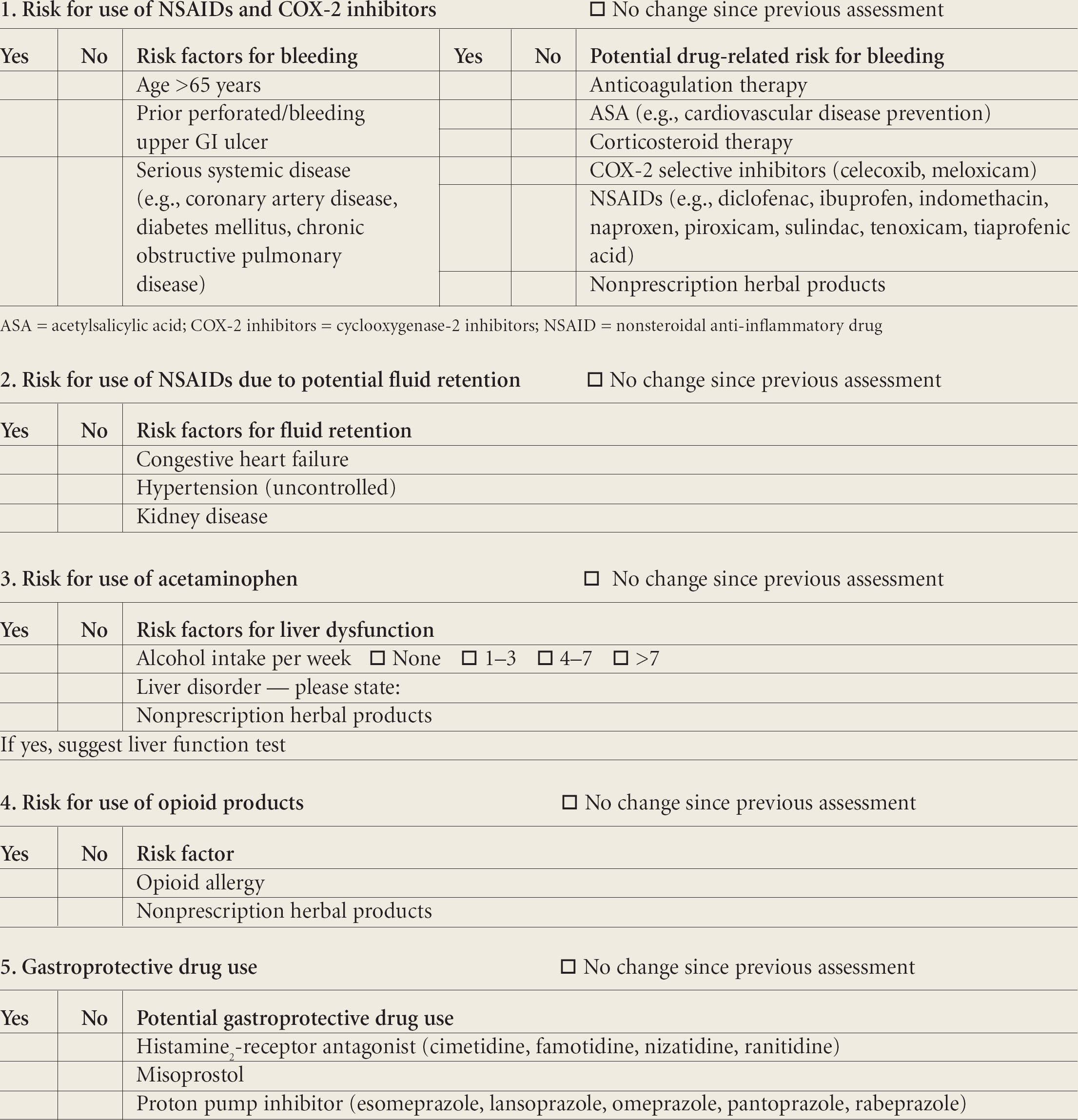
Appendix 1 Inclusion and exclusion criteria Medication management: The pharmacist will conduct a thorough review of the participants' prescription and over-the-counter analgesic use, in concordance with the current guidelines and indicators pertaining to pharmacologic therapy, and the criteria for acetaminophen, nonsteroidal anti-inflammatory drug (NSAID) and gastroprotective use and their contraindications.4,6,13–15 To achieve maximum therapeutic benefit and safety, participants will also be counselled on risks, benefits, and appropriate use. (See Appendix 2 for identification of risk factors.) Communication with primary care physician: The study coordinator will fax a letter to the family physician, identifying the participant as having a high likelihood of knee OA, according to the pharmacist screening questionnaire and the list of evidence-based quality indicators for knee OA management (Appendix 1). In addition, the pharmacist will provide to the participant's family physician a recommendation on medications, as well as a form for referral to a physiotherapist at the Arthritis Centre. Physiotherapy guided exercise program: If the participant is referred, the physiotherapist will schedule a meeting to determine an appropriate, individualized home exercise program.
For the usual care group, research staff, blinded to the outcomes, will perform outcome assessments at baseline and at 3 and 6 months.
Outcomes
The primary outcome measure will be the Arthritis Foundation Quality Indicators for the Management of OA. 6 Specifically, consistent with other investigators, we will calculate the summary scores of OA quality of care for each subject. 7 This indicates the percentage of indicators passed for a particular patient who may have been eligible for indications, ranging from 0 to 8. We will calculate the summary score as the total number of indicators passed, divided by the total number of indicators for which the patient was eligible. Summary scores will be compared across study groups.
Secondary outcomes will be a reduction in NSAID use, appropriate gastroprotective agent use, compliance with the exercise program and medications, pain control, functional status, and quality of life, as measured by the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index, 16 Health Utilities Index Mark 3 (HUI Mark 3), 17 and the Lower Extremity Function Scale. 18 Adverse events will be monitored.
Ethics
This study has been approved by the University of British Columbia Clinical Research Ethics Board. We will obtain informed written consent from each patient. The study protocol was registered with www.clinicaltrials.gov to comply with international standards of trial reporting.
Statistical considerations
Appendix 2 Identification of risk factors
Current status of the study
We began recruiting for a pilot to ensure that the procedures are feasible and streamlined. Full recruitment for this study began in May 2007.
Footnotes
Acknowledgements:
This study was funded by a pilot grant from the Canadian Institutes of Health Research/Canadian Arthritis Network New Emerging Team Grant (Tooling Up for Early Osteoarthritis) and by peer-reviewed operating grants from the Michael Smith Foundation for Health Research and the Canadian Arthritis Network. Dr. Marra is a Health Services Scholar, supported by the Michael Smith Foundation for Medical Research, and is a Government of Canada Research Chair in Pharmaceutical Outcomes. Dr. Cibere is supported by a JW McConnell Family Foundation Scholar Award and a CIHR Clinical Scientist Award. Dr. Tsuyuki is supported by the Merck Frosst/Aventis Chair in Patient Health Management at the University of Alberta. Dr. Khan is a New Investigator at the Canadian Institutes of Health Research.